You might also like
- LymphDocument9 pagesLymphAlyesha Maloney100% (1)
- (Methods in Molecular Biology 1323) Rémy Bosselut, Melanie S. Vacchio (Eds.) - T-Cell Development - Methods and Protocols (2016, Humana Press) PDFDocument295 pages(Methods in Molecular Biology 1323) Rémy Bosselut, Melanie S. Vacchio (Eds.) - T-Cell Development - Methods and Protocols (2016, Humana Press) PDFfrancisca100% (1)
- Rheumatoid ArthritisDocument77 pagesRheumatoid ArthritisTalal SafdarNo ratings yet
- ESR Verification FormDocument2 pagesESR Verification Formlance tabinas83% (6)
- Gopu.R:::: Patient Age / Sex 30 Y / Male BranchDocument1 pageGopu.R:::: Patient Age / Sex 30 Y / Male BranchGopu RNo ratings yet
- Infection Control: The New York RequirementDocument3 pagesInfection Control: The New York RequirementLiezel100% (1)
- HIV in PregnancyDocument7 pagesHIV in PregnancyYwagar YwagarNo ratings yet
- Agglutination TestDocument34 pagesAgglutination TestAJAYNo ratings yet
- COVID-19 (Coronavirus) Exposure Questionnaire: Please Answer The Following Questions in As Much Detail As PossibleDocument2 pagesCOVID-19 (Coronavirus) Exposure Questionnaire: Please Answer The Following Questions in As Much Detail As PossibleDharm prakashNo ratings yet
- Health Checklist Form For Visitors: Nakaranas Ka Ba NG Mga Sumusunod: Oo HindiDocument2 pagesHealth Checklist Form For Visitors: Nakaranas Ka Ba NG Mga Sumusunod: Oo HindiCoin CharNo ratings yet
- CIF TemplateDocument2 pagesCIF Templateluvaire23No ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument2 pagesCoronavirus Disease (COVID-19) : Case Investigation FormShiela E. EladNo ratings yet
- 6.1 Health Declaration Form - VisitorDocument1 page6.1 Health Declaration Form - VisitoryyNo ratings yet
- INDIVIDUAL Form Mandatory For ALL Passengers Arriving in Spain. Print in Capital (UPPERCASE) Letters. Leave A Blank Space Between WordsDocument2 pagesINDIVIDUAL Form Mandatory For ALL Passengers Arriving in Spain. Print in Capital (UPPERCASE) Letters. Leave A Blank Space Between WordsAndreea PuscaNo ratings yet
- GERMANY Aussteigekarte - Luftverkehr - EN PDFDocument2 pagesGERMANY Aussteigekarte - Luftverkehr - EN PDFE-Printing MureșNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormMizraim TupazNo ratings yet
- 6.2 Health Declaration Form - EmployeeDocument1 page6.2 Health Declaration Form - EmployeeyyNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormmaelisaNo ratings yet
- CoViD19-Covid Investigation FormDocument1 pageCoViD19-Covid Investigation FormMc Arem PaghunasanNo ratings yet
- 23 PH Health Declaration Form (Crew)Document1 page23 PH Health Declaration Form (Crew)Ali WaleedNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormPresinto Dos Parañaque KnightsNo ratings yet
- CoViD19-CIF-v6-Fillable QCv3-2Document1 pageCoViD19-CIF-v6-Fillable QCv3-2Patrice De CastroNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormChum ChitaruNo ratings yet
- Coronavirus Self-Declaration Form: First Name: Last Name: Appointment Date & Time: Contact Person in SMCDocument3 pagesCoronavirus Self-Declaration Form: First Name: Last Name: Appointment Date & Time: Contact Person in SMCswati durejaNo ratings yet
- Guests DeclarationDocument2 pagesGuests DeclarationRuddy NaranjoNo ratings yet
- Case Investigation FormDocument2 pagesCase Investigation FormVerge Kat PauleNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument2 pagesCoronavirus Disease (COVID-19) : Case Investigation FormJudeLaxNo ratings yet
- Combined PLF HDF 1.7.21Document2 pagesCombined PLF HDF 1.7.21Margarida TeixeiraNo ratings yet
- Print in Capital (UPPERCASE) Letters. Leave A Blank Space Between WordsDocument2 pagesPrint in Capital (UPPERCASE) Letters. Leave A Blank Space Between WordsDino Diego PennestriNo ratings yet
- Aaron Teodosio - MECQ-Health-AssessmentDocument5 pagesAaron Teodosio - MECQ-Health-AssessmentRon TeodosioNo ratings yet
- Annex 2i Investigation Form 29092020Document6 pagesAnnex 2i Investigation Form 29092020nik mohamad zulfikriNo ratings yet
- Coronavirus Disease (COVID-19) : Philippine National Police Health Service PNP General HospitalDocument1 pageCoronavirus Disease (COVID-19) : Philippine National Police Health Service PNP General HospitalKarsenley Cal-el Iddig BurigsayNo ratings yet
- Spain FCS Inglés Avión v02 SEDocument2 pagesSpain FCS Inglés Avión v02 SEGodwin E OrumwenseNo ratings yet
- Print in Capital (UPPERCASE) Letters. Leave A Blank Space Between WordsDocument2 pagesPrint in Capital (UPPERCASE) Letters. Leave A Blank Space Between WordsDan PopescuNo ratings yet
- FCS EnglishDocument2 pagesFCS EnglishOana NemteanuNo ratings yet
- Spain FCS Inglés - Avión v02 - SEDocument2 pagesSpain FCS Inglés - Avión v02 - SEQuad WorkoutNo ratings yet
- Declaration of Good Health Form - With Covid QDocument2 pagesDeclaration of Good Health Form - With Covid QRajnish YadavNo ratings yet
- Coronavirus Self-Declaration Form: Lsnurse@islux - LuDocument2 pagesCoronavirus Self-Declaration Form: Lsnurse@islux - LuSiddharth SoporiNo ratings yet
- Viral Haemorrhagic Fever - Case Reporting Form IDSR Viral Hemorrhagic Fever Case Report FormDocument1 pageViral Haemorrhagic Fever - Case Reporting Form IDSR Viral Hemorrhagic Fever Case Report FormSalihu MustaphaNo ratings yet
- 2019 Coronavirus Disease (Covid-19) : 1. Patient ProfileDocument1 page2019 Coronavirus Disease (Covid-19) : 1. Patient ProfileMarythel CamachoNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument2 pagesCoronavirus Disease (COVID-19) : Case Investigation FormChamee MallillinNo ratings yet
- Health Center/Clinic/Hospital: Out Patient Department (OPD) RegisterDocument4 pagesHealth Center/Clinic/Hospital: Out Patient Department (OPD) RegisterGetu Tadele100% (2)
- COVID-19 Vaccination Pre-Registration Form - 1 Dose: 1. BiodataDocument2 pagesCOVID-19 Vaccination Pre-Registration Form - 1 Dose: 1. BiodataMaimoon AliNo ratings yet
- Dhiraj Mishra: COVID-19 (Coronavirus) Exposure QuestionnaireDocument3 pagesDhiraj Mishra: COVID-19 (Coronavirus) Exposure QuestionnaireadiNo ratings yet
- Released: Sunpower Philippines Medical Screening Form (MSF)Document2 pagesReleased: Sunpower Philippines Medical Screening Form (MSF)glenn dalesNo ratings yet
- COVID-19 Travel FormDocument2 pagesCOVID-19 Travel FormJoe Spector25% (4)
- COVID-19 (Coronavirus) Exposure QuestionnaireDocument2 pagesCOVID-19 (Coronavirus) Exposure QuestionnaireadiNo ratings yet
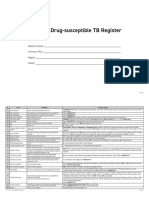
- Form 6a. Drug Susceptible TB RegisterDocument4 pagesForm 6a. Drug Susceptible TB RegisterAllen ChesterNo ratings yet
- Arrival To Egypt Declaration Form: Yes: NoDocument2 pagesArrival To Egypt Declaration Form: Yes: NoMarkus TrautmannNo ratings yet
- B.L.I.S.T.T Health Declaration Form: Baguio - La Trinidad - Itogon - Sablan - Tuba - TublayDocument1 pageB.L.I.S.T.T Health Declaration Form: Baguio - La Trinidad - Itogon - Sablan - Tuba - TublayLC LeeNo ratings yet
- 3-COVID Line List 03042020Document30 pages3-COVID Line List 03042020lorenaNo ratings yet
- Residents & Guests - HEALTH & TRAVEL DECLARATION FORM - FillableDocument1 pageResidents & Guests - HEALTH & TRAVEL DECLARATION FORM - FillableSlumberland TradingNo ratings yet
- COVID-19 (Coronavirus) Exposure QuestionnaireDocument3 pagesCOVID-19 (Coronavirus) Exposure QuestionnairePrabhuNo ratings yet
- Boris Johnson TranscriptsDocument15 pagesBoris Johnson TranscriptsGvantsa MandzulashviliNo ratings yet
- Health Screening Questionnaire For F2FDocument1 pageHealth Screening Questionnaire For F2FJacquelyn GuchoneNo ratings yet
- Health Symptoms Questionnaire For F2FDocument1 pageHealth Symptoms Questionnaire For F2FMarc CaurelNo ratings yet
- COVID-19: Client & Employee Screening QuestionnaireDocument2 pagesCOVID-19: Client & Employee Screening QuestionnaireAlyssa MirabellaNo ratings yet
- ESR Form GrezDocument2 pagesESR Form Grezlizabernard.hernandezNo ratings yet
- Self Declaration For Covid 19 1st PageDocument1 pageSelf Declaration For Covid 19 1st PagedfjasdhgfjkasdgsNo ratings yet
- Self Declaration Form MeluhaDocument1 pageSelf Declaration Form MeluhaSandy BergerNo ratings yet
- 3 Self Declaration Form All International Passengers Arriving Into India 6Document1 page3 Self Declaration Form All International Passengers Arriving Into India 6Ankit SharmaNo ratings yet
- C Ovid Data AnalysisDocument3 pagesC Ovid Data Analysismuhammad shoaibNo ratings yet
- Tanauan City Integrated High School Trapiche 1, Tanauan City, Batangas Health Declaration FormDocument4 pagesTanauan City Integrated High School Trapiche 1, Tanauan City, Batangas Health Declaration FormKurt VillaNo ratings yet
- Imo Circular Ship Crew Changes - Crew Self Health Declaration and Temperature RecordsDocument2 pagesImo Circular Ship Crew Changes - Crew Self Health Declaration and Temperature RecordsVasil RaykovNo ratings yet
- Sample OHIP Application Form: A. Personal InformationDocument1 pageSample OHIP Application Form: A. Personal InformationSreeman MypatiNo ratings yet
- Combating The Global Food Crisis: Worldwide Food Supply ChallengesDocument2 pagesCombating The Global Food Crisis: Worldwide Food Supply ChallengesMOHAMMED DEMMUNo ratings yet
- Publi MDocument81 pagesPubli MMOHAMMED DEMMUNo ratings yet
- Discrete DependentDocument53 pagesDiscrete DependentMOHAMMED DEMMUNo ratings yet
- The Hand in Hand Initiative: 1. ConceptDocument22 pagesThe Hand in Hand Initiative: 1. ConceptMOHAMMED DEMMUNo ratings yet
- Effective PGDocument30 pagesEffective PGMOHAMMED DEMMUNo ratings yet
- Public Economics: Lecture 4: Public Goods and ExternalitiesDocument91 pagesPublic Economics: Lecture 4: Public Goods and ExternalitiesMOHAMMED DEMMUNo ratings yet
- Derivation Offer Curve ABVMDocument13 pagesDerivation Offer Curve ABVMMOHAMMED DEMMUNo ratings yet
- Deriving The Offer Curve For Analysis of Changes in TradeDocument4 pagesDeriving The Offer Curve For Analysis of Changes in TradeMOHAMMED DEMMUNo ratings yet
- Aspects of Project Preparation and Analysis To Design and Analyze Effective ProjectsDocument8 pagesAspects of Project Preparation and Analysis To Design and Analyze Effective ProjectsMOHAMMED DEMMUNo ratings yet
- What Is Comparative AdvantageDocument6 pagesWhat Is Comparative AdvantageMOHAMMED DEMMUNo ratings yet
- Concept of Production Possibility CurveDocument4 pagesConcept of Production Possibility CurveMOHAMMED DEMMUNo ratings yet
- Meaning and Reasons For International TradeDocument6 pagesMeaning and Reasons For International TradeMOHAMMED DEMMUNo ratings yet
- Export Trade: All You Need To KnowDocument4 pagesExport Trade: All You Need To KnowMOHAMMED DEMMUNo ratings yet
- Modul Hematoimun (Dr. Fakhri) - Immunity To Parasitic InfectionsDocument17 pagesModul Hematoimun (Dr. Fakhri) - Immunity To Parasitic InfectionsFajr Muzammil100% (1)
- Phadiatop Rev 051605Document1 pagePhadiatop Rev 051605Kat Chique BNo ratings yet
- Nnate Mmune Ecognition: Charles A. Janeway, Jr. and Ruslan MedzhitovDocument22 pagesNnate Mmune Ecognition: Charles A. Janeway, Jr. and Ruslan MedzhitovMaximeNo ratings yet
- YersiniaDocument46 pagesYersiniajamal nasir50% (2)
- Gonorrhea Fact SheetDocument2 pagesGonorrhea Fact SheetRebecca Richardson0% (1)
- Read The Text What Is A Coronavirus?Document2 pagesRead The Text What Is A Coronavirus?Erick Sayd ContrerasNo ratings yet
- CD Summer Review 1Document157 pagesCD Summer Review 1Nikko MelencionNo ratings yet
- CHAPTER 16 MicroparaDocument46 pagesCHAPTER 16 MicroparaKathlyn LopeñaNo ratings yet
- Statement of Virus Isolation SOVI by Morell Cowan and KaufmanDocument4 pagesStatement of Virus Isolation SOVI by Morell Cowan and Kaufmancrossx14100% (3)
- Faecal Calprotectin Indicates Intestinal InflammatDocument2 pagesFaecal Calprotectin Indicates Intestinal Inflammatakbar011512No ratings yet
- Reaction Paper: Editorial Text About Covid-19Document1 pageReaction Paper: Editorial Text About Covid-19Gaea AngelaNo ratings yet
- T & D - DERMATOLOGY - 2022 - QuestionDocument6 pagesT & D - DERMATOLOGY - 2022 - QuestionVyserionNo ratings yet
- Dynamics of Disease Transmission2Document45 pagesDynamics of Disease Transmission2Tarique KhanNo ratings yet
- COVID-19 Response - Living With COVID-19Document63 pagesCOVID-19 Response - Living With COVID-19eman mamdohNo ratings yet
- Dengue Fever: A Statistical Analysis Regarding Awareness About Dengue Among University Students in Azad KashmirDocument8 pagesDengue Fever: A Statistical Analysis Regarding Awareness About Dengue Among University Students in Azad KashmirIm jungkook JUSTIN SEAGULL A.K.A jungshookNo ratings yet
- Bacterial Infection On Upper Respiratory Tract Hemofillus Moraxella Fusobacterium Ed 1Document29 pagesBacterial Infection On Upper Respiratory Tract Hemofillus Moraxella Fusobacterium Ed 1Cintya Risti MawarniNo ratings yet
- Hepes ZosterDocument12 pagesHepes ZosterChino RamirezNo ratings yet
- Rd-15 Bartholin Cyst and Abscess 10-12Document2 pagesRd-15 Bartholin Cyst and Abscess 10-12Chong Hui ChekNo ratings yet
- AMENDMENT DIRECTIVE TO CONTROL COVID 19 PANDEMIC No 933 2022 EthiopiaDocument3 pagesAMENDMENT DIRECTIVE TO CONTROL COVID 19 PANDEMIC No 933 2022 EthiopiaAhmed AdemNo ratings yet
- Academicians Pentavalent Vaccine 2Document6 pagesAcademicians Pentavalent Vaccine 2Mld OnnetNo ratings yet
- Annex A and B For Dengvaxia ProfilingDocument3 pagesAnnex A and B For Dengvaxia ProfilingAnne 닌 야 PiedadNo ratings yet
- DAFTAR PUSTAKA Proposal Nongki KariDocument2 pagesDAFTAR PUSTAKA Proposal Nongki KariNongki KariNo ratings yet
- Health Teaching Plan SampleDocument4 pagesHealth Teaching Plan SampleLicha Javier100% (1)