Mastoid obliteration
Information for patients provided by the Otology Department
What is mastoid obliteration?
You have been recommended for mastoid cavity obliteration surgery to eliminate a troublesome
mastoid cavity. The most common reason for a troublesome mastoid cavity is recurrent or
persistent infections.
Here we explain some of the aims, benefits, risks, and alternatives to the proposed operation. The
operation itself will also be explained.
We want you to be informed about your choices so that you can be fully involved in making any
decisions about your operation. Please ask about anything you do not fully understand or wish to
have explained in more detail.
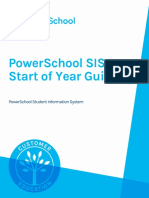
How does the ear work?
The ear consists of the outer, middle,
and inner ear. Sound travels through
the outer ear and reaches the eardrum, Ear Bones
causing it to vibrate. The vibration is
then transmitted through three tiny
bones, called the ossicles, in the
middle ear.
Air
The vibration then enters the inner ear,
which is a snail-shaped bony structure
filled with fluid. The nerve cells within
the inner ear are stimulated to produce
signals which are carried to the brain, Wax
where they are interpreted as sound. Ear Drum Eustachian Tube Adenoids
1 of 7 Mastoid obliteration (January 2024)
What is the mastoid bone?
The mastoid bone is the bony prominence that can be felt just
behind the ear (see diagram).
It contains a number of air spaces, the largest of which is called
the antrum, and connects with air space in the middle ear.
Ear diseases in the middle ear can extend into the mastoid bone.
Diagram showing the
mastoid bone
Why have I been referred for mastoid cavity obliteration?
Following your previous surgery, one or more of the structures in your ear (such as your ear drum,
ossicles, and part of your mastoid bone) have been removed, resulting in a mastoid cavity.
You have been recommended for mastoid obliteration surgery as your mastoid cavity is continually
discharging or accumulating dead skin, and it has not improved with regular cleaning and antibiotic
drops.
The purpose of this surgery is to remove the disease from your ear, whether it is infected tissue or
cholesteatoma (dead skin that collects in your ear and can destroy the structures around it), and
then to reconstruct your ear.
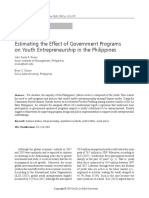
Ear canal with mastoid
Ear canal without
cavity mastoid cavity
What are the intended benefits of mastoid cavity obliteration?
• The main benefit of this procedure is to give you a dry, waterproof, and trouble-free ear.
• Sometimes, if the hearing mechanism of your inner ear is still working, it may be possible to
improve your hearing in the affected ear. Your surgeon will be able to advise and discuss this
with you. It is not always possible to improve hearing, even when the hearing function of your
inner ear still works.
2 of 7 Mastoid obliteration (January 2024)
How successful is this procedure?
About 85 in every 100 patients will have a dry, trouble-free ear after this operation. We also hope
to improve your hearing. The success rate of improving your hearing is in the region of 60 in 100
patients. If your hearing cannot be improved, a safe, dry waterproof ear may allow you to wear a
hearing aid or your surgeon may recommend an alternative hearing solution after healing.
Who will perform my procedure?
An ear nose and throat (ENT) surgeon, with the appropriate experience, will perform your
procedure.
What will happen before my procedure?
• Most patients attend a pre-admission clinic led by a nurse, some days or weeks before their
surgery.
• At this clinic, we will ask you for details of your medical history and carry out any necessary
clinical examinations and investigations such as checking your blood pressure, pulse, and
weight. This is a good opportunity for you to ask us any questions about your procedure, but
please feel free to discuss any concerns at any time.
• You will be asked if you are taking any tablets or other types of medication, these might be
ones prescribed by a doctor or bought over the counter in a pharmacy. It helps us if you bring
with you details of any medications or supplements you are taking.
• Stopping smoking helps you to heal quicker after your surgery, amongst other benefits. The
Stop Smoking Service offers free support, so please ask if you would like a referral.
Will I have an anaesthetic?
Yes. This procedure involves the use of a general anaesthetic, which means you will be asleep for
your procedure.
Will I have to stay in hospital overnight?
Most people who have this type of procedure can go home on the same day as their surgery.
Sometimes we know before your surgery whether you will need to stay for longer than usual; your
doctor will discuss this with you before you decide to have the operation.
Does some of my hair need to be removed before my procedure?
The healthcare team needs to see or reach the skin behind your ear for the operation. So they can
do this, they will probably need to use an electric hair clipper (with a single-use disposable head)
to remove some of your hair on the day of surgery. Please do not shave the hair yourself as this
can increase the risk of skin infection.
You will be advised to shower and wash your hair either the night before or on the morning of your
operation.
3 of 7 Mastoid obliteration (January 2024)
What happens during the operation?
The surgery is performed under general anaesthetic and may take up to five hours.
Once you are asleep, an incision (cut) is made behind your ear and the infected tissues in the
mastoid, along with cholesteatoma (dead skin), are removed to reveal healthy bone. If the surgeon
sees any residual (leftover) infection, the infected bone will be cleared by drilling it away.
At this point synthetic bone substitute, or your own bone dust or chips are used to fill the cavity.
The filling material is then covered with cartilage and local soft tissue flaps to help create a healthy
ear canal.
Your surgeon will often reconstruct your eardrum using cartilage, depending on what structures
are still available and healthy in your ear. If there is a hope that your hearing can be improved,
then the ossicular chain (bones of hearing) may be replaced with a prosthetic (artificial) ossicle
made out of titanium. These prostheses are MRI compatible. This will be discussed with you in
your clinic appointments, however it is often impossible to decide if this is an option until during the
operation itself.
The ear is then packed with ribbon gauze, soaked with antiseptic paste, to keep the graft in place.
The wound is stitched with dissolvable sutures and an adhesive dressing (steristrips) is applied to
protect it. A cushioning bandage is applied and kept on overnight. Your surgeon will usually advise
you to remove this at home.
Are there alternatives to this procedure?
The only way to guarantee that you will not have further problems, arising from your mastoid
cavity, is by removing the cavity (obliteration). In patients who are unfit for this surgery, the only
alternative is to have a specialist regularly clean the ear and for the patient to use antibiotic ear
drops or creams. This, at best, could reduce the discharge.
Are there any significant, unavoidable, or frequently occurring risks of mastoid cavity
obliteration surgery?
There are some risks that you must consider before giving consent to this treatment. You should
speak to your surgeon about the chances of any complications in your case.
• Scar
You will have a scar behind your ear. To start with, this will be a red/pink colour but will fade to
a white colour with time and become less noticeable. This scar may be uncomfortable for some
time after your operation, often many months. You may experience some numbness around
the scar, which may or may not improve with time. Sometimes a scar may become larger than
immediately after the operation (hypertrophic or keyloid), which may need a further procedure
at a later date.
• Bleeding
You may experience some bloodstained discharge from your ear in the weeks following your
operation. If the bleeding does not settle, please contact Rotary Ward on the number at the end
of this leaflet and ask to speak to the ENT doctor on-call.
• Loss of hearing
In a small number of patients, the hearing may be made worse due to damage to the inner
ear. It is possible that the hearing in the ear being operated on may be lost completely and
permanently (sometimes called a dead ear).
4 of 7 Mastoid obliteration (January 2024)
• Dizziness
Dizziness is common for a few hours following mastoid cavity obliteration surgery and may
result in nausea (feeling sick) and vomiting. On rare occasions, dizziness can be significant
and persistent, needing a longer stay in hospital and specialist physiotherapy.
• Tinnitus
Sometimes a patient may notice noise in their ear, particularly if their hearing loss gets worse.
This noise is known as tinnitus and can be temporary or permanent.
• Weakness of one side of the face
The nerve that controls movement of the muscles of the face runs inside the ear and may
be damaged during your operation. If this happens, your face may lose its movement on the
side of the operation, but it is usually temporary. A facial nerve monitor is used during your
procedure to help reduce the risk of nerve damage. There is a very small risk of permanent
paralysis of one side of the face.
• Taste disturbance
The taste nerve runs close to the eardrum and may occasionally be damaged. This can
cause an abnormal taste on one side of your tongue. This is usually temporary but it can be
permanent in about one in 10 of patients affected.
• Cerebrospinal fluid leak
The brain lies on top of the mastoid bone, surrounded by a fluid called cerebrospinal fluid or
CSF. On rare occasions, the ear disease may erode into the bone that separates the mastoid
from the brain, or the bone can be breached during surgery. If a CSF leak is seen during
surgery it is repaired at the time. Sometimes the leak appears later on and another operation
will be needed.
• Reaction to ear dressings
Occasionally, your ear may develop an allergic reaction to the dressings we use in your
ear canal. If this happens, the pinna (outer ear) may become swollen, red, and itchy. If this
happens, you should speak to your surgeon so that they can remove the dressing from your
ear. The allergic reaction should settle down after a few days.
• Change in shape of the ear
Cartilage used to obliterate the cavity will be taken from your ear during surgery. This is done
in a way that, in most cases, is not noticeable. There is a small risk however that the shape of
your ear may change slightly as a result of removing some of this cartilage.
• Haematoma formation
A haematoma is a collection of blood under the skin. If this happens on or around your ear,
then it may need removing with a further small procedure to avoid deformity of your ear or
development of an infection.
There are general risks to all major operations, due to having a general anaesthetic. You can
discuss these with your anaesthetist before your surgery.
Developing blood clots in your legs or lung are also general risks when having surgery. As part of
your pre-admission checks you will be risk assessed for developing clots in your legs (deep vein
thrombosis or DVT) or lungs (pulmonary embolism or PE) and options for minimising these risks
will be discussed with you.
5 of 7 Mastoid obliteration (January 2024)
You may change your mind about your operation at any time, and signing a consent form
does not mean that you have to have the operation.
If you would like to have a second opinion about your treatment, you can ask your specialist; they
will not mind arranging this for you. You may wish to ask your own GP to arrange a second opinion
with another specialist.
Will I be in pain after my procedure?
Your surgeon will use an injection around your ear, before your operation begins, to reduce your
pain after surgery. Your ear may ache a little after your procedure, but this can be controlled with
painkillers that we will ask you to buy, such as paracetamol and ibuprofen. More painkillers may be
provided by the hospital before you are discharged.
When can I resume normal activities?
We will help you to move around as soon as possible after your procedure. This helps improve
your recovery and reduces the risk of certain complications.
When can I return to work?
You may need to take two to four weeks off work or school after your operation.
When can I leave hospital?
You will usually go home the same day. You will have a head bandage that you can remove the
next day, but you must leave the packing inside your ear. You should speak to your surgeon if
you suddenly experience deafness, dizziness, or severe pain after you are sent home from the
hospital.
How do I look after my wound following my procedure?
• There are usually no stitches to be removed. The stitches we use are beneath your skin and
dissolve on their own over time.
• You may have some sticky strips over your wound that you can remove around seven days
after your operation. If they peel off before this then this is nothing to worry about and they do
not need replacing.
• There may be a small amount of discharge from your ear canal. This usually comes from the
dressings and settles in three to four days. If the discharge continues, there is a lot of it, and it
is smelly or you have any pain or itching, you should contact the hospital.
• Your ear canal will be full of dressing/packing that will be removed at your first follow-up
appointment; usually four weeks after your operation. Because of this packing your hearing
may well seem worse than before your operation. We will not be able to assess your hearing
until this packing is removed from your ear. The final result regarding your hearing is only
known three months after surgery, after all the healing has taken place.
• If some of the packing falls out, it is sensible to trim the loose end of packing with scissors and
leave the rest in place.
6 of 7 Mastoid obliteration (January 2024)
• You should keep your ear dry for the first few weeks after surgey. Plug it with a cotton wool ball
coated with Vaseline when you are having a shower. We recommend that you do not wash
your hair until the ear packing is removed in clinic. Dry shampoo can be used instead.
• Avoid straining/lifting anything heavy for the first few weeks after surgery.
• Only blow your nose gently.
• Avoid air travel for two months.
• You are advised to avoid diving or flying when you have a cold, if possible.
Will I have a follow-up appointment?
You will receive an appointment to return to the clinic four weeks following your operation. This is
mainly to remove the packing and check your ear.
We will see you again three months after your surgery, where we will check your ear and perform
an audiogram; any further treatments you may need will be discussed then.
You will need to come to the ENT Department for your follow-up, for a minimum of five years after
your operation. The appointments are usually every year and your surgeon may also order an MRI
scan to check your ear, usually one year after your operation. Further MRI scans may be needed.
What if I have any problems or concerns?
Call the ENT team on-call at William Harvey Hospital via the hospital switchboard on 01233 63 33
31 or Rotary Ward on 01233 61 62 34. Ask to speak to either the on call ENT registrar or nurse
practitioner for advice.
This leaflet has been produced with and for patients
If you would like this information in another language, audio, Braille, Easy
Read, or large print please ask a member of staff. You can ask someone to
contact us on your behalf.
Any complaints, comments, concerns, or compliments please speak to your doctor or
nurse, or contact the Patient Advice and Liaison Service (PALS) on 01227 78 31 45, or email
ekh-tr.pals@nhs.net
Patients should not bring in large sums of money or valuables into hospital. Please note
that East Kent Hospitals accepts no responsibility for the loss or damage to personal property,
unless the property had been handed in to Trust staff for safe-keeping.
Further patient leaflets are available via the East Kent Hospitals web site www.ekhuft.nhs.uk/
patientinformation
Information produced by the Otology Department
Date: January 2021 Review date: May 2024 Web 503
7 of 7 Mastoid obliteration (January 2024)
You might also like
- GOV Salary ScaleDocument23 pagesGOV Salary ScaleChadwick BarclayNo ratings yet
- MLTC Champion Show Shedule 2021 October 2ndDocument6 pagesMLTC Champion Show Shedule 2021 October 2ndapi-198076804No ratings yet
- Coalition's $10b BlackholeDocument10 pagesCoalition's $10b BlackholePolitical AlertNo ratings yet
- Formulation and Evaluation of Topical Dosage Form Containing Microspheres For Model Anti Inflammatory DrugDocument15 pagesFormulation and Evaluation of Topical Dosage Form Containing Microspheres For Model Anti Inflammatory DrugCandriya LaelNo ratings yet
- American National Standard For Financial PDFDocument19 pagesAmerican National Standard For Financial PDFaakbaralNo ratings yet
- Healthy Start, Grow Smart Series - 06 - Six MonthDocument15 pagesHealthy Start, Grow Smart Series - 06 - Six MonthMihaelaPantaNo ratings yet
- Usnea - ApotheciumDocument7 pagesUsnea - ApotheciumVarada K DasNo ratings yet
- Digested Journal#7Document4 pagesDigested Journal#7Jay Raymond DelfinNo ratings yet
- G20 Quiz Competition BrochureDocument5 pagesG20 Quiz Competition BrochureRahul jhaNo ratings yet
- CDS Rev14 - 1 2022-02-09Document34 pagesCDS Rev14 - 1 2022-02-09dennys sofia rozo medinaNo ratings yet
- Kidder S. Q. & Haar T. H. - Satellite Meteorology - Index (1995)Document7 pagesKidder S. Q. & Haar T. H. - Satellite Meteorology - Index (1995)celso QueteNo ratings yet
- India Is A Socialist Republic According To The Preamble of The Constitution of IndiaDocument6 pagesIndia Is A Socialist Republic According To The Preamble of The Constitution of IndiaSHASHI BHUSHANNo ratings yet
- El I Gi Bi L I T Y: - : Tat Aai Amaharakshasupr EmeDocument5 pagesEl I Gi Bi L I T Y: - : Tat Aai Amaharakshasupr EmePradeep NadarNo ratings yet
- Iks/S, Oa Tarqvksa DK Laj (K.KDocument13 pagesIks/S, Oa Tarqvksa DK Laj (K.KAshutosh KaushikNo ratings yet
- Data Norek DPLK AmpenanDocument20 pagesData Norek DPLK AmpenanY & HNo ratings yet
- Tensile Properties and Viscoelastic Model of A Polyimide FilmDocument10 pagesTensile Properties and Viscoelastic Model of A Polyimide FilmShengde ZhangNo ratings yet
- Nature Unbound - Conservation Capitalism and The Future of Protected AreasDocument265 pagesNature Unbound - Conservation Capitalism and The Future of Protected AreasernestofluNo ratings yet
- Newton's Laws Escape Room Key Section 1Document2 pagesNewton's Laws Escape Room Key Section 1cybersnake72No ratings yet
- Lecture 1 - IntroductionDocument29 pagesLecture 1 - IntroductionSiti Nurhaslinda Bt ZakariaNo ratings yet
- Nps PFM SchemeInfoDocument4 pagesNps PFM SchemeInfoEr. Nidhi ShahNo ratings yet
- Fast Food Competition-3-29Document27 pagesFast Food Competition-3-29Thanh Hà TrầnNo ratings yet
- Development and Validation of A LC/MS/MS Method For The Determination of Duloxetine in Human Plasma and Its Application To Pharmacokinetic StudyDocument14 pagesDevelopment and Validation of A LC/MS/MS Method For The Determination of Duloxetine in Human Plasma and Its Application To Pharmacokinetic StudyMohamed Medhat AliNo ratings yet
- StrengthDocument78 pagesStrengthJoseph Mbsui Andrew AP21110040013No ratings yet
- By Night Abyss RitualsDocument3 pagesBy Night Abyss RitualsalexisgroovyNo ratings yet
- JMD 19083Document3 pagesJMD 19083anton MDNo ratings yet
- PowerSchool SIS Start of Year GuideDocument30 pagesPowerSchool SIS Start of Year GuideSandi HodgsonNo ratings yet
- The Main Effects of Global WarmingDocument3 pagesThe Main Effects of Global WarmingAna MladinNo ratings yet
- The University of Dschang and Her National and International Cooperation From 1972 To 2016Document20 pagesThe University of Dschang and Her National and International Cooperation From 1972 To 2016IJAERS JOURNALNo ratings yet
- S-3109 FinalDocument60 pagesS-3109 FinalRaúl Oscar LedesmaNo ratings yet
- Trane Equipment and Services OverviewDocument28 pagesTrane Equipment and Services OverviewZvonimir PerasovićNo ratings yet
- Iridian 3Q10 LetterDocument15 pagesIridian 3Q10 LetterHariharan SundaresanNo ratings yet
- Wellness Policy 2015Document2 pagesWellness Policy 2015api-301953890No ratings yet
- 63 BD 111532 Ee 3113 RD Bo AAgenda SEZwDocument39 pages63 BD 111532 Ee 3113 RD Bo AAgenda SEZwGIFT CityNo ratings yet
- Nanoparticle-Based Therapeutic Approaches For Wound Healing - A Review of The State-Of-The-ArtDocument34 pagesNanoparticle-Based Therapeutic Approaches For Wound Healing - A Review of The State-Of-The-ArtMilan JovicNo ratings yet
- UntitledDocument11 pagesUntitledSonia KousarNo ratings yet
- Application of Numerical Models To Evaluate Oil SPDocument9 pagesApplication of Numerical Models To Evaluate Oil SPLeidy CastroNo ratings yet
- PE 10 Q2 M7-ModifiedDocument14 pagesPE 10 Q2 M7-ModifiedJubilo , Daniella Mae S.No ratings yet
- Open Bionics LTD Ob Valuation Exit Opportunities 2022Document4 pagesOpen Bionics LTD Ob Valuation Exit Opportunities 2022Dragan SaldzievNo ratings yet
- Corporate Valuation: Tata Motors LTDDocument10 pagesCorporate Valuation: Tata Motors LTDUTKARSH PABALENo ratings yet
- Cortnée N. Love Department of Education, Drexel University EDUC 540: Field Placement Professor Meagan RodriguezDocument5 pagesCortnée N. Love Department of Education, Drexel University EDUC 540: Field Placement Professor Meagan Rodriguezapi-521599993No ratings yet
- TC200 - Om 2Document192 pagesTC200 - Om 2DmitryNo ratings yet
- Part+1+of+20+ +Applications+for+a+Plasmoids+Form+and+Functions+ +Draft+518,400+b+Kmv+ +August+Monday+29th+2022Document72 pagesPart+1+of+20+ +Applications+for+a+Plasmoids+Form+and+Functions+ +Draft+518,400+b+Kmv+ +August+Monday+29th+2022totoNo ratings yet
- Block 6 SEQsDocument49 pagesBlock 6 SEQsBosco785No ratings yet
- English7 Q1 M1 W1Document22 pagesEnglish7 Q1 M1 W1donabelle mianoNo ratings yet
- VN CapticalDocument90 pagesVN CapticalPhuongNo ratings yet
- Music1-Second QuarterDocument42 pagesMusic1-Second QuarterZairah Lyn SaysonNo ratings yet
- Insurer Market PowerDocument7 pagesInsurer Market PowerTom BiusoNo ratings yet
- Imperative For Ag-Food Innovation: Biostl Approach: Revitalizing Rural Communities Bridging The Urban-Rural DivideDocument56 pagesImperative For Ag-Food Innovation: Biostl Approach: Revitalizing Rural Communities Bridging The Urban-Rural DivideNational Press FoundationNo ratings yet
- Annual Report 21-22-1Document116 pagesAnnual Report 21-22-1ranjitrajivNo ratings yet
- TDS Sipernat 50S OriginalDocument2 pagesTDS Sipernat 50S OriginalFabio Arboleda TorresNo ratings yet
- M3A79-T DeluxeDocument164 pagesM3A79-T Deluxepeeg2ochNo ratings yet
- STS Chapter 3Document5 pagesSTS Chapter 3krung krung biNo ratings yet
- 1 s2.0 S2666833521000381 MainDocument11 pages1 s2.0 S2666833521000381 Mainiñaki zamora sevillaNo ratings yet
- Pompeo Unit 3 Networking PlanDocument17 pagesPompeo Unit 3 Networking Planapi-654903205No ratings yet
- REGISTER DBD KOTA BONTANG 2023 21 MeiDocument46 pagesREGISTER DBD KOTA BONTANG 2023 21 Meiyusuf lensa hamdanNo ratings yet
- Profil Fermentasi Sukrosa Menjadi SORBITOL OLEH Zymomonas Mobilis DENGAN Penambahan Kation Logam Divalen ZNDocument122 pagesProfil Fermentasi Sukrosa Menjadi SORBITOL OLEH Zymomonas Mobilis DENGAN Penambahan Kation Logam Divalen ZNValerie hongNo ratings yet
- Movement Disorders of The Mouth Review of The Common Phenomenologies 2022Document19 pagesMovement Disorders of The Mouth Review of The Common Phenomenologies 2022Gonçalo CabralNo ratings yet
- A BERT Encoding With Recurrent Neural Network and Long-Short Term Memory For Breast Cancer Image Classification - 1-s2.0-S2772662223000176-MainDocument15 pagesA BERT Encoding With Recurrent Neural Network and Long-Short Term Memory For Breast Cancer Image Classification - 1-s2.0-S2772662223000176-MainSrinitish SrinivasanNo ratings yet
- Horizon LawsuitDocument15 pagesHorizon LawsuitRobert GarciaNo ratings yet
- Myringoplasty and TympanoplastyDocument4 pagesMyringoplasty and TympanoplastyK.charitha ChowdaryNo ratings yet
- dp1812 Microfinancial Linkages Shallow MarketsDocument53 pagesdp1812 Microfinancial Linkages Shallow MarketsLovesickbut PrettysavageNo ratings yet
- Andrei Enterpri - 3Document1 pageAndrei Enterpri - 3Lovesickbut PrettysavageNo ratings yet
- Activity 1.Document2 pagesActivity 1.Lovesickbut PrettysavageNo ratings yet
- UntitledDocument1 pageUntitledLovesickbut PrettysavageNo ratings yet
- Enriching OutputDocument1 pageEnriching OutputLovesickbut PrettysavageNo ratings yet
- ActivityDocument1 pageActivityLovesickbut PrettysavageNo ratings yet
- ABM 12 B - Activity 2Document1 pageABM 12 B - Activity 2Lovesickbut PrettysavageNo ratings yet
- Activity 1.Document2 pagesActivity 1.Lovesickbut PrettysavageNo ratings yet
- Activity 1Document6 pagesActivity 1Lovesickbut PrettysavageNo ratings yet
- UntitledDocument1 pageUntitledLovesickbut PrettysavageNo ratings yet
- Estimating The Effect of Government Programs On Youth Entrepreneurship in The PhilippinesDocument9 pagesEstimating The Effect of Government Programs On Youth Entrepreneurship in The PhilippinesLovesickbut PrettysavageNo ratings yet
- Partnership Terms ReviewerDocument5 pagesPartnership Terms ReviewerLovesickbut PrettysavageNo ratings yet
- Econ Finals ReviewDocument10 pagesEcon Finals ReviewLovesickbut PrettysavageNo ratings yet
- Global Fund To Fight AIDS, Tuberculosis, and MalariaDocument12 pagesGlobal Fund To Fight AIDS, Tuberculosis, and MalariaLovesickbut PrettysavageNo ratings yet
- Surname, First Name Middle Name: Residential Address E-Mail Address Mobile No.Document1 pageSurname, First Name Middle Name: Residential Address E-Mail Address Mobile No.Lovesickbut PrettysavageNo ratings yet
- Sample ResumeDocument1 pageSample ResumeLovesickbut PrettysavageNo ratings yet
- Wounds and BleedingDocument57 pagesWounds and BleedingAnn Merlin JobinNo ratings yet
- Basal Cell Carsinoma: Novita Hianto 07120020021 BedahDocument9 pagesBasal Cell Carsinoma: Novita Hianto 07120020021 BedahFerdy ErawanNo ratings yet
- Bioethics Quiz (Oct. 14)Document7 pagesBioethics Quiz (Oct. 14)RM DemetilloNo ratings yet
- WHLP Music 10 1Document15 pagesWHLP Music 10 1Rommel LagaticNo ratings yet
- What Is A Bone Marrow Transplant?Document4 pagesWhat Is A Bone Marrow Transplant?Krisna AgustiniNo ratings yet
- Dr. Nagula Praveen, MD, DMDocument79 pagesDr. Nagula Praveen, MD, DMDr. RajibNo ratings yet
- Fixed Prosthodontic Designs: Dr. Mohammed Yousef Miqdad Ass. Professor, Faculty of Dentistry, Al-Azhar University-GazaDocument37 pagesFixed Prosthodontic Designs: Dr. Mohammed Yousef Miqdad Ass. Professor, Faculty of Dentistry, Al-Azhar University-Gazaعبد الرحمن خالد الزميليNo ratings yet
- BladderDocument107 pagesBladderRocci Jack ParseNo ratings yet
- Veterinary Medicine 7th EditionDocument2 pagesVeterinary Medicine 7th EditionpintuNo ratings yet
- MalariaDocument6 pagesMalariaShadab Ahmad KhanNo ratings yet
- VertebrobasilarDocument35 pagesVertebrobasilarBen Asiel PadangNo ratings yet
- Chapter 2Document24 pagesChapter 2Eden Marie FranciscoNo ratings yet
- AmebiasisDocument32 pagesAmebiasisRizty Mayang FachleviNo ratings yet
- 17 6 14 VeR Korban Hidup KupangDocument44 pages17 6 14 VeR Korban Hidup Kupangrara prameiNo ratings yet
- Development of The Infant and Young ChildDocument406 pagesDevelopment of The Infant and Young Childdarkorx100% (1)
- Acclarent Aera Fact SheetDocument2 pagesAcclarent Aera Fact SheetalexharripersadNo ratings yet
- Exploring Lifespan Development 4th Edition Berk Solutions ManualDocument13 pagesExploring Lifespan Development 4th Edition Berk Solutions ManualAngieFisherxirmc100% (12)
- Medicine: Sudden Seizure During Cesarean SectionDocument2 pagesMedicine: Sudden Seizure During Cesarean SectionDavid RefuncionNo ratings yet
- Ati Codes Cont'Document1 pageAti Codes Cont'm1k0eNo ratings yet
- 2020 06 18 Coronavirus Covid 19 Infection in PregnancyDocument61 pages2020 06 18 Coronavirus Covid 19 Infection in PregnancyIndah AulliaNo ratings yet
- Principles of Cavity Preparation LECDocument2 pagesPrinciples of Cavity Preparation LECKen HoiNo ratings yet
- EngDocument76 pagesEngMaimunah Novita SariNo ratings yet
- DISEASES - Immune SystemsDocument3 pagesDISEASES - Immune SystemsMolan JenaNo ratings yet
- AORN 2020: Guidelines For Perioperative Practice: Patient Skin AntisepsisDocument30 pagesAORN 2020: Guidelines For Perioperative Practice: Patient Skin AntisepsisAldy Mulia Hati SetyaNo ratings yet
- Pakistan Health SolutionsDocument43 pagesPakistan Health SolutionsShayan Abbas100% (1)
- Ahc Chapter 22 Infection ControlDocument20 pagesAhc Chapter 22 Infection Controlapi-209542414No ratings yet
- Maternal and Perinatal Death Surveillance and Response:: Materials To Support ImplementationDocument140 pagesMaternal and Perinatal Death Surveillance and Response:: Materials To Support ImplementationBianca Maria PricopNo ratings yet
- Hunter Crane Job Shadow ReflectionDocument3 pagesHunter Crane Job Shadow Reflectionapi-304880833No ratings yet
- 1003 MedtechWire TriVascularDocument1 page1003 MedtechWire TriVascularClyve ParkerNo ratings yet
- Ethical Dilemmas in Pandemics - Lessons From COVIDDocument8 pagesEthical Dilemmas in Pandemics - Lessons From COVIDSurya MahardikaNo ratings yet