You might also like
- Design and Development of A Hand Exoskeleton Robot For Active and Passive RehabilitationDocument12 pagesDesign and Development of A Hand Exoskeleton Robot For Active and Passive RehabilitationMNo ratings yet
- A Novel Elbow Pneumatic Muscle Actuator For Exoskeleton Arm in Post-Stroke RehabilitationDocument6 pagesA Novel Elbow Pneumatic Muscle Actuator For Exoskeleton Arm in Post-Stroke RehabilitationSathvik BhatNo ratings yet
- A Fairly Simple Mechatronic Device For Training Human Wrist MotionDocument15 pagesA Fairly Simple Mechatronic Device For Training Human Wrist Motionalamin khondakerNo ratings yet
- 15 2021 MDPI Study To Increase The TRL of Exoskeleton ERMIS BasDocument16 pages15 2021 MDPI Study To Increase The TRL of Exoskeleton ERMIS BasUS SILVA (MEX)No ratings yet
- Strokerehabilitationusingexoskeleton-basedroboticexercisersDocument6 pagesStrokerehabilitationusingexoskeleton-basedroboticexercisersAnh HuyNo ratings yet
- Novel Soft Bending Actuator-Based Power Augmentation Hand Exoskeleton Controlled by Human IntentionDocument22 pagesNovel Soft Bending Actuator-Based Power Augmentation Hand Exoskeleton Controlled by Human IntentionAlemeNo ratings yet
- Applsci 11 04145Document17 pagesApplsci 11 04145oreaby05No ratings yet
- Development of Low-Cost Portable Hand Exoskeleton For Assistive and Rehabilitation PurposesDocument14 pagesDevelopment of Low-Cost Portable Hand Exoskeleton For Assistive and Rehabilitation Purposesgil lerNo ratings yet
- Current Hand Exoskeleton Technologies For PDFDocument18 pagesCurrent Hand Exoskeleton Technologies For PDFAlexandra NistorNo ratings yet
- Review Article: Robotic Technologies and Rehabilitation: New Tools For Stroke Patients' TherapyDocument9 pagesReview Article: Robotic Technologies and Rehabilitation: New Tools For Stroke Patients' TherapyyunitadwisNo ratings yet
- Towards Realising Wearable Exoskeletons For Elderly PeopleDocument6 pagesTowards Realising Wearable Exoskeletons For Elderly PeopleRatna SambhavNo ratings yet
- Robotic Orthosis For Upper Limb Rehabilitation: P EedingsDocument13 pagesRobotic Orthosis For Upper Limb Rehabilitation: P EedingsDaniel TamashiroNo ratings yet
- Edo Arte ExoskeletonDocument54 pagesEdo Arte ExoskeletonBlanca RiosNo ratings yet
- Design and Testing of A Soft Parallel Robot Based On Pneumatic Artificial Muscles For Wrist RehabilitationDocument11 pagesDesign and Testing of A Soft Parallel Robot Based On Pneumatic Artificial Muscles For Wrist Rehabilitation王根萌No ratings yet
- Actuators 11 00167 v3Document14 pagesActuators 11 00167 v3carlosNo ratings yet
- Yan 2015Document17 pagesYan 2015Gabriel DelgadoNo ratings yet
- Myoelectric Control Strategies For Rehabilitation RobotsDocument17 pagesMyoelectric Control Strategies For Rehabilitation Robotsmb.farooqui02No ratings yet
- 2018 Article 642Document14 pages2018 Article 642Faqih FathurrozanNo ratings yet
- Exo-Glove: A Soft Wearable Robotic Hand For Stroke SurvivorsDocument7 pagesExo-Glove: A Soft Wearable Robotic Hand For Stroke SurvivorsmaheshNo ratings yet
- AI and Medical RobotsDocument13 pagesAI and Medical RobotsCassandraRhys 0311No ratings yet
- 10 1016@j JHT 2020 03 024Document10 pages10 1016@j JHT 2020 03 024eduar yecid duarte gomezNo ratings yet
- Generation and Control of Adaptive Gaits in Lower-Limb Exoskeletons For Motion AssistanceDocument16 pagesGeneration and Control of Adaptive Gaits in Lower-Limb Exoskeletons For Motion AssistanceShailesh BishnoiNo ratings yet
- Towards The Mechatronic Development of A New Upper-Limb Exoskeleton (SAMA)Document25 pagesTowards The Mechatronic Development of A New Upper-Limb Exoskeleton (SAMA)alamin khondakerNo ratings yet
- Medical Robotics: Virginia Commonwealth University, Richmond, Virginia, U.S.ADocument12 pagesMedical Robotics: Virginia Commonwealth University, Richmond, Virginia, U.S.ARb EyewearNo ratings yet
- An Attention-Controlled Hand Exoskeleton For The Rehabilitation of Finger Extension and Flexion Using A Rigid-Soft Combined MechanismDocument13 pagesAn Attention-Controlled Hand Exoskeleton For The Rehabilitation of Finger Extension and Flexion Using A Rigid-Soft Combined MechanismCarlos Arturo TorresNo ratings yet
- Exoskeleton ArmDocument5 pagesExoskeleton Armc214ocNo ratings yet
- Paper 26-1Document6 pagesPaper 26-1Carlene joy ManaloNo ratings yet
- Torricelli 2016 Bioinspir. Biomim. 11 051002Document21 pagesTorricelli 2016 Bioinspir. Biomim. 11 051002Tình Nguyễn VănNo ratings yet
- Development of An Upper Limb Exoskeleton For Rehabilitation With Feedback From EMG and IMU SensorDocument7 pagesDevelopment of An Upper Limb Exoskeleton For Rehabilitation With Feedback From EMG and IMU SensorkeerthiNo ratings yet
- Ergonomics in The Industry 40 Exoskeletons PDFDocument2 pagesErgonomics in The Industry 40 Exoskeletons PDFAldiko 1No ratings yet
- Hand Extension Robot Orthosis HERO Glove Development and Testing With Stroke Survivors With Severe Hand ImpairmentDocument11 pagesHand Extension Robot Orthosis HERO Glove Development and Testing With Stroke Survivors With Severe Hand ImpairmentMark CagnanNo ratings yet
- Lower Limb Rehabilitation Exoskeleton Robot ReviewDocument17 pagesLower Limb Rehabilitation Exoskeleton Robot Reviewbetelhemterefe wondimagenihuNo ratings yet
- Biomechatronic Design and Control of An Anthropomorphic Artificial Hand For Prosthetic ApplicationsDocument19 pagesBiomechatronic Design and Control of An Anthropomorphic Artificial Hand For Prosthetic ApplicationsGiang TruongNo ratings yet
- Mechanical Design and Trajectory Planning of A Lower Limb Rehabilitation Robot With A Variable WorkspaceDocument13 pagesMechanical Design and Trajectory Planning of A Lower Limb Rehabilitation Robot With A Variable Workspacetanvir anwarNo ratings yet
- A Pneumatic Glove and Immersive Virtual Reality Environment For Hand Rehabilitative Training After StrokeDocument9 pagesA Pneumatic Glove and Immersive Virtual Reality Environment For Hand Rehabilitative Training After StrokeLovin BiancaNo ratings yet
- Proietti 2016 Upper-Limb RoboticDocument13 pagesProietti 2016 Upper-Limb RoboticNeuroNo ratings yet
- 'Robotic Exoskeleton'Document25 pages'Robotic Exoskeleton'Lakshmi Tanmai0% (1)
- Elsevier: Nexos - AN SupportDocument6 pagesElsevier: Nexos - AN SupportGuna SeelanNo ratings yet
- export-pdfDocument2 pagesexport-pdfmiguelvicente150801No ratings yet
- Development of A Flexible Rehabilitation System For Bedridden PatientsDocument19 pagesDevelopment of A Flexible Rehabilitation System For Bedridden Patientsalamin khondakerNo ratings yet
- Guest Editorial An Overview of Biomedical Robotics and Bio-Mechatronics Systems and ApplicationsDocument6 pagesGuest Editorial An Overview of Biomedical Robotics and Bio-Mechatronics Systems and ApplicationsİTYNo ratings yet
- Troncossi-et-al_GEF-2012_v1_UMDocument11 pagesTroncossi-et-al_GEF-2012_v1_UMAnh HuyNo ratings yet
- Training For Users of Myoelectric Multigrip Hand.5Document8 pagesTraining For Users of Myoelectric Multigrip Hand.5Ai Reen ChuNo ratings yet
- Application of Wearable Sensors in Actuation and Control of Powered Ankle Exoskeletons A Comprehensive Review - Sensors-22-02244Document5 pagesApplication of Wearable Sensors in Actuation and Control of Powered Ankle Exoskeletons A Comprehensive Review - Sensors-22-02244Generation GenerationNo ratings yet
- frobt-11-1341580Document19 pagesfrobt-11-1341580SkHasanNo ratings yet
- Module 1 Exam STSDocument4 pagesModule 1 Exam STSAlyssa OrtegaNo ratings yet
- Bionic GloveDocument7 pagesBionic GloveMd ShitolNo ratings yet
- Design and Simulation of Bionic Glove For Rehabilitation of The ParalyticsDocument7 pagesDesign and Simulation of Bionic Glove For Rehabilitation of The ParalyticsAdi CrişanNo ratings yet
- Applied SciencesDocument22 pagesApplied SciencesHamrah SiddiquiNo ratings yet
- Gassert-Dietz2018 Article RehabilitationRobotsForTheTreaDocument15 pagesGassert-Dietz2018 Article RehabilitationRobotsForTheTreaMouyad SrNo ratings yet
- Robot-Assisted Ankle Rehabilitation For The Treatment of Drop Foot: A Case StudyDocument5 pagesRobot-Assisted Ankle Rehabilitation For The Treatment of Drop Foot: A Case StudyIhsanNo ratings yet
- Research On A New Rehabilitation Robot For Balance DisordersDocument10 pagesResearch On A New Rehabilitation Robot For Balance DisordersSyed MoinuddinNo ratings yet
- Design of An Assistive, Glove-Based Exoskeleton: Chad G. Rose and Marcia K. O'MalleyDocument2 pagesDesign of An Assistive, Glove-Based Exoskeleton: Chad G. Rose and Marcia K. O'MalleyYoussef NagatyNo ratings yet
- The Design and Control of A Therapeutic Exercise Robot For Lower Limb Rehabilitation - PhysiotherabotDocument14 pagesThe Design and Control of A Therapeutic Exercise Robot For Lower Limb Rehabilitation - PhysiotherabotIsaac Septimo EscamillaNo ratings yet
- Self Alignment Mechanism - For Upper Arm and LegDocument15 pagesSelf Alignment Mechanism - For Upper Arm and LegMohamed TamerNo ratings yet
- The Development and Testing of A Human Machine Interface For A Mobile Medical ExoskeletonDocument6 pagesThe Development and Testing of A Human Machine Interface For A Mobile Medical ExoskeletonArsyad Zanadin RamadhanNo ratings yet
- Developing a user-friendly telerehabilitation system for stroke patientsDocument7 pagesDeveloping a user-friendly telerehabilitation system for stroke patientsMuhammad ImronNo ratings yet
- Biomechatronics Design of A Novel Artificial Arm: A. Malik Mohd Ali M. Mahadi - Abdul JamilDocument5 pagesBiomechatronics Design of A Novel Artificial Arm: A. Malik Mohd Ali M. Mahadi - Abdul JamilİTYNo ratings yet
- (2020) Inflatable Soft Wearable Robot For Reducing Therapist Fatigue During Upper Extremity RehabilitationDocument9 pages(2020) Inflatable Soft Wearable Robot For Reducing Therapist Fatigue During Upper Extremity Rehabilitationjhonrt06mxNo ratings yet
- CompositeDocument32 pagesCompositeSandeep KumarNo ratings yet
- Robotics-Notes From MuDocument113 pagesRobotics-Notes From MuGet OutNo ratings yet
- 10158676953506001Document2 pages10158676953506001LTHCB ITNo ratings yet
- Draw An Assembly Drawing of The Clamp As Shown in Figure 1. Draw Detailed Drawings of The Individual Parts. Create A Standard Parts SheetDocument1 pageDraw An Assembly Drawing of The Clamp As Shown in Figure 1. Draw Detailed Drawings of The Individual Parts. Create A Standard Parts SheetSandeep KumarNo ratings yet
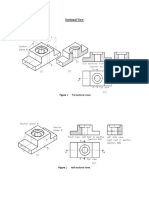
- Sectional DrawingsDocument4 pagesSectional DrawingsSandeep KumarNo ratings yet
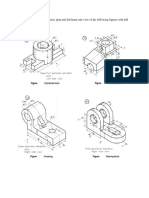
- Section.: Question 5. Draw The Elevation, Plan and Left Hand Side View of The Following Figures With FullDocument1 pageSection.: Question 5. Draw The Elevation, Plan and Left Hand Side View of The Following Figures With FullSandeep KumarNo ratings yet
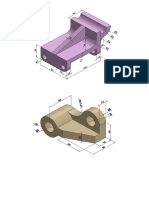
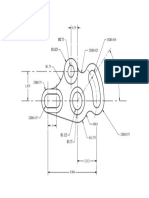
- 2D and 3D Drawings For PracticeDocument7 pages2D and 3D Drawings For PracticeSandeep KumarNo ratings yet
- GT CELLS GROUP SIMILAR PARTS FOR EFFICIENT PRODUCTIONDocument15 pagesGT CELLS GROUP SIMILAR PARTS FOR EFFICIENT PRODUCTIONSandeep KumarNo ratings yet
- 2D Practice DrawingsDocument1 page2D Practice DrawingsSandeep KumarNo ratings yet
- 2DDrawing 3 ModelDocument1 page2DDrawing 3 ModelSandeep KumarNo ratings yet
- Programming For Turning CycleDocument1 pageProgramming For Turning CycleSandeep KumarNo ratings yet
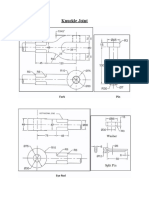
- Knuckle JointDocument1 pageKnuckle JointSandeep KumarNo ratings yet
- Development of Surfaces-ModelDocument1 pageDevelopment of Surfaces-ModelSandeep KumarNo ratings yet
- IIT Hyderabad Workshop Practice ME 101 GuideDocument51 pagesIIT Hyderabad Workshop Practice ME 101 GuideHittendra Singh100% (3)
- Roller AssemblyDocument1 pageRoller AssemblySandeep KumarNo ratings yet
- G7 Spa Obusan Grade - Section - Nutri Status - 2023 2024Document4 pagesG7 Spa Obusan Grade - Section - Nutri Status - 2023 2024Nelson Jeff Jr. MagpaliNo ratings yet
- TX Hosp Based Prac List 120120Document975 pagesTX Hosp Based Prac List 120120David SantosNo ratings yet
- The Dumbo Guide To Diffusion-Weighted Imaging (DWI) : C Ackermann, S AndronikouDocument2 pagesThe Dumbo Guide To Diffusion-Weighted Imaging (DWI) : C Ackermann, S AndronikouCatalina VenegasNo ratings yet
- Waist Circumference Percentiles of Black South African Children Aged 10 - 14 Years From Different Study SitesDocument9 pagesWaist Circumference Percentiles of Black South African Children Aged 10 - 14 Years From Different Study SitesyutefupNo ratings yet
- DesignDocument14 pagesDesignLorena DazaNo ratings yet
- Simera, Bea Michaela C. - Arch 101 - Arints - Case StudyDocument23 pagesSimera, Bea Michaela C. - Arch 101 - Arints - Case StudyBea MichaelaNo ratings yet
- CPT Code Guidelines For Nuclear Medicine and PETDocument2 pagesCPT Code Guidelines For Nuclear Medicine and PETsujithasNo ratings yet
- BMI FormulaDocument21 pagesBMI FormulaNatalio AguadoNo ratings yet
- Women's Clothing Size Conversion: A Comprehensive GuideDocument1 pageWomen's Clothing Size Conversion: A Comprehensive GuideAlain CheryNo ratings yet
- Freestyle swimming speeds and strokesDocument10 pagesFreestyle swimming speeds and strokesAndica DiamantaNo ratings yet
- Image Registration in RadiotherapyDocument27 pagesImage Registration in Radiotherapynilesh kumarNo ratings yet
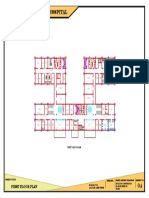
- 100 Bedded General Hospital: First Floor PlanDocument1 page100 Bedded General Hospital: First Floor PlanAshish chauhanNo ratings yet
- MX9C Color Doppler SystemDocument4 pagesMX9C Color Doppler Systemสุมิตตา อ่อนมั่งคงNo ratings yet
- The Modern Technology of Radiation Oncology VolumeDocument2 pagesThe Modern Technology of Radiation Oncology VolumeSebastian GarciaNo ratings yet
- Anthropometry ReflectionDocument2 pagesAnthropometry ReflectionTessNo ratings yet
- Calculate BMI, Ideal Body WeightDocument22 pagesCalculate BMI, Ideal Body WeightCathy Dao-ayenNo ratings yet
- Elastografía Tiroides: Gustavo Arturo C., LLANOVARCED DAMIÁNDocument26 pagesElastografía Tiroides: Gustavo Arturo C., LLANOVARCED DAMIÁNmariaNo ratings yet
- Teaching P.E. and Health in The Elementary GradesDocument20 pagesTeaching P.E. and Health in The Elementary GradesTech VlogsNo ratings yet
- Resume MedisDocument6 pagesResume MedisRina ekaNo ratings yet
- 191 - XBOE4103 - Occupational Ergonomics Lab ManualDocument16 pages191 - XBOE4103 - Occupational Ergonomics Lab ManualHuda Hafiz100% (1)
- Preview of "MyDietAnalysis - Report"Document2 pagesPreview of "MyDietAnalysis - Report"LeovergeldediosNo ratings yet
- WP ErgoStandards PDFDocument5 pagesWP ErgoStandards PDFJohn JustinusNo ratings yet
- Andreas: Focused Assessment With Sonography in TraumaDocument13 pagesAndreas: Focused Assessment With Sonography in Traumarina paramitaNo ratings yet
- Grade 6 Nutritional RecordsDocument41 pagesGrade 6 Nutritional RecordsPrincess TeodoroNo ratings yet
- Pet CTDocument4 pagesPet CTKanishk R.SinghNo ratings yet
- BMI Calculator JavaDocument2 pagesBMI Calculator JavaeyaknaraNo ratings yet
- Nutritional Status of Children UnderDocument8 pagesNutritional Status of Children UnderInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Merck & Company Product - Decision TreeDocument11 pagesMerck & Company Product - Decision TreeIgor SoaresNo ratings yet
- BMI Grade 9 Sapphire EditedDocument43 pagesBMI Grade 9 Sapphire EditedMargie Valero PascualNo ratings yet
- CCPS (2022) - Human Factors Handbook For Process Plant Operations - Improving Process Safety and System PerformanceDocument440 pagesCCPS (2022) - Human Factors Handbook For Process Plant Operations - Improving Process Safety and System PerformanceDiego Serrão100% (1)
- Artificial Intelligence: From Medieval Robots to Neural NetworksFrom EverandArtificial Intelligence: From Medieval Robots to Neural NetworksRating: 4 out of 5 stars4/5 (3)
- PLC Programming & Implementation: An Introduction to PLC Programming Methods and ApplicationsFrom EverandPLC Programming & Implementation: An Introduction to PLC Programming Methods and ApplicationsNo ratings yet
- Artificial Intelligence Revolution: How AI Will Change our Society, Economy, and CultureFrom EverandArtificial Intelligence Revolution: How AI Will Change our Society, Economy, and CultureRating: 4.5 out of 5 stars4.5/5 (2)
- ChatGPT Money Machine 2024 - The Ultimate Chatbot Cheat Sheet to Go From Clueless Noob to Prompt Prodigy Fast! Complete AI Beginner’s Course to Catch the GPT Gold Rush Before It Leaves You BehindFrom EverandChatGPT Money Machine 2024 - The Ultimate Chatbot Cheat Sheet to Go From Clueless Noob to Prompt Prodigy Fast! Complete AI Beginner’s Course to Catch the GPT Gold Rush Before It Leaves You BehindNo ratings yet
- Artificial You: AI and the Future of Your MindFrom EverandArtificial You: AI and the Future of Your MindRating: 4 out of 5 stars4/5 (3)
- Dark Aeon: Transhumanism and the War Against HumanityFrom EverandDark Aeon: Transhumanism and the War Against HumanityRating: 5 out of 5 stars5/5 (1)
- Mastering Drones - A Beginner's Guide To Start Making Money With DronesFrom EverandMastering Drones - A Beginner's Guide To Start Making Money With DronesRating: 2.5 out of 5 stars2.5/5 (3)
- Atlas of AI: Power, Politics, and the Planetary Costs of Artificial IntelligenceFrom EverandAtlas of AI: Power, Politics, and the Planetary Costs of Artificial IntelligenceRating: 5 out of 5 stars5/5 (9)
- In the Age of AI: How AI and Emerging Technologies Are Disrupting Industries, Lives, and the Future of WorkFrom EverandIn the Age of AI: How AI and Emerging Technologies Are Disrupting Industries, Lives, and the Future of WorkRating: 5 out of 5 stars5/5 (1)
- Robotics: Designing the Mechanisms for Automated MachineryFrom EverandRobotics: Designing the Mechanisms for Automated MachineryRating: 4.5 out of 5 stars4.5/5 (8)
- Comprehensive Guide to Robotic Process Automation (RPA): Tips, Recommendations, and Strategies for SuccessFrom EverandComprehensive Guide to Robotic Process Automation (RPA): Tips, Recommendations, and Strategies for SuccessNo ratings yet
- Collection of Raspberry Pi ProjectsFrom EverandCollection of Raspberry Pi ProjectsRating: 5 out of 5 stars5/5 (1)
- Projects With Microcontrollers And PICCFrom EverandProjects With Microcontrollers And PICCRating: 5 out of 5 stars5/5 (1)
- Artificial Intelligence: The Complete Beginner’s Guide to the Future of A.I.From EverandArtificial Intelligence: The Complete Beginner’s Guide to the Future of A.I.Rating: 4 out of 5 stars4/5 (5)
- Modeling, Dynamics, and Control of Electrified VehiclesFrom EverandModeling, Dynamics, and Control of Electrified VehiclesRating: 5 out of 5 stars5/5 (1)
- What to Expect When You're Expecting Robots: The Future of Human-Robot CollaborationFrom EverandWhat to Expect When You're Expecting Robots: The Future of Human-Robot CollaborationRating: 4.5 out of 5 stars4.5/5 (2)
- Learning Robotics, with Robotics, by Robotics: Educational RoboticsFrom EverandLearning Robotics, with Robotics, by Robotics: Educational RoboticsNo ratings yet
- Arduino: The complete guide to Arduino for beginners, including projects, tips, tricks, and programming!From EverandArduino: The complete guide to Arduino for beginners, including projects, tips, tricks, and programming!Rating: 4 out of 5 stars4/5 (3)
- Create Profitable Side Hustles with Artificial IntelligenceFrom EverandCreate Profitable Side Hustles with Artificial IntelligenceNo ratings yet
- Design and Operation of Human Locomotion SystemsFrom EverandDesign and Operation of Human Locomotion SystemsMarco CecarelliNo ratings yet
- RoboNexus: Bridging Realms: The Confluence of Mechanics, Electronics, and ProgrammingFrom EverandRoboNexus: Bridging Realms: The Confluence of Mechanics, Electronics, and ProgrammingNo ratings yet