You might also like
- Hypertension For StudentsDocument64 pagesHypertension For StudentsNajib Al FatinNo ratings yet
- Ground Power Unit: GA ModelDocument17 pagesGround Power Unit: GA ModelAngelica Nava0% (1)
- National Leaflet About CKD and eGFR For GPs Updated September 2007 PDFDocument2 pagesNational Leaflet About CKD and eGFR For GPs Updated September 2007 PDFRifky Octavio PNo ratings yet
- Blood Physiology 2022Document116 pagesBlood Physiology 2022Gurmessa FekaduNo ratings yet
- Toxicological Stability of Drugs: de Jesus, Adia Cavrinni G. Manalo, Alyssa ADocument42 pagesToxicological Stability of Drugs: de Jesus, Adia Cavrinni G. Manalo, Alyssa AAlyssa ManaloNo ratings yet
- PAMDocument14 pagesPAMRashed IslamNo ratings yet
- HbA1c Test 1Document11 pagesHbA1c Test 1Mohammed R.HusseinNo ratings yet
- Guidelines For The Management of Alcohol Dependendence and Acute Withdrawal On General Psychiatry Wards May 2017Document10 pagesGuidelines For The Management of Alcohol Dependendence and Acute Withdrawal On General Psychiatry Wards May 2017renzo85rhNo ratings yet
- Items of Work For RoadsDocument6 pagesItems of Work For Roadsjhc1123No ratings yet
- Quiz 2 Principles of DesignDocument4 pagesQuiz 2 Principles of DesignJovito Reyes0% (1)
- Addresses Contact Details of InstitutesDocument16 pagesAddresses Contact Details of Institutesanon_961232893No ratings yet
- Phytotherapy in the Management of Diabetes and Hypertension: Volume 2From EverandPhytotherapy in the Management of Diabetes and Hypertension: Volume 2Rating: 5 out of 5 stars5/5 (1)
- Test Engleza Clasa A5a Modul 3Document3 pagesTest Engleza Clasa A5a Modul 3Adelina HasasNo ratings yet
- CarbamazepinaDocument15 pagesCarbamazepinaNataliaPalacínBernalNo ratings yet
- CKD CmeDocument45 pagesCKD Cmeizatul farhanahNo ratings yet
- HPN in CKDDocument27 pagesHPN in CKDLeigh Picardal Caragos-MerinNo ratings yet
- ChlordiazepoxideDocument9 pagesChlordiazepoxideMister CaballeroNo ratings yet
- FAQ - DOAC in CKD Update - FinalDocument4 pagesFAQ - DOAC in CKD Update - Finalraea.dobsonNo ratings yet
- CARVEDILOL Nursing ImplicationsDocument2 pagesCARVEDILOL Nursing Implicationsshiraz.aNo ratings yet
- Leung 2018Document26 pagesLeung 2018Dewi MNo ratings yet
- Medicines For CKD A Practical-Guide PrintVersionDocument14 pagesMedicines For CKD A Practical-Guide PrintVersionKalashini SenadheeraNo ratings yet
- Cards JC - Association of Rivaroxaban Vs Apixaban With Major Ischemic or Hemorrhagic Events in Patients With Atrial FibrillationDocument18 pagesCards JC - Association of Rivaroxaban Vs Apixaban With Major Ischemic or Hemorrhagic Events in Patients With Atrial Fibrillationapi-602288180No ratings yet
- AssignmentDocument1 pageAssignmentAllysa MendozaNo ratings yet
- Antihyperlipidemic AgentsDocument71 pagesAntihyperlipidemic AgentsFirda100% (1)
- How To Achieve Target BP in CKD DR Paramita AyuDocument53 pagesHow To Achieve Target BP in CKD DR Paramita Ayuxiongmao2389No ratings yet
- Dyslipidaemia GuidelinesDocument28 pagesDyslipidaemia GuidelinesEllieNo ratings yet
- Arterial Blood Gas (Abg)Document10 pagesArterial Blood Gas (Abg)Kita kitaNo ratings yet
- COVID19 - DexamethasoneDocument2 pagesCOVID19 - DexamethasoneLe Hoang TuanNo ratings yet
- Abvd Hem HLDocument6 pagesAbvd Hem HLTowhidulIslamNo ratings yet
- Tatalaksana Kad 1Document7 pagesTatalaksana Kad 1Nurul Kamilah SadliNo ratings yet
- Alogaritma CKDDocument2 pagesAlogaritma CKDChairunnisa SiamNo ratings yet
- Abvd Hem HLDocument10 pagesAbvd Hem HLMohammed HaiderNo ratings yet
- Diabetic Care in Acute Febrile IllnessDocument27 pagesDiabetic Care in Acute Febrile IllnessDr-Ajay TripathiNo ratings yet
- DOAC VTE Treatment April2020Document4 pagesDOAC VTE Treatment April2020Ahmed MohammedNo ratings yet
- Cholesterol GuidelinesDocument2 pagesCholesterol GuidelinesJuan Miguel PangilinanNo ratings yet
- Presentasi Hipertensi BPJS 20518Document109 pagesPresentasi Hipertensi BPJS 20518Dody TamaraNo ratings yet
- Anaemia Management in People With Chronic Kidney Disease Anaemia Management in People With Chronic Kidney Disease OverviewDocument9 pagesAnaemia Management in People With Chronic Kidney Disease Anaemia Management in People With Chronic Kidney Disease Overviewraheemrahi089No ratings yet
- Class 2: ECE-Rft Part 2, VitaminsDocument85 pagesClass 2: ECE-Rft Part 2, VitaminsammuNo ratings yet
- An Overview of Hyperinsulinemic-Euglycemic Therapy in Calcium Channel Blocker and β-blocker OverdoseDocument30 pagesAn Overview of Hyperinsulinemic-Euglycemic Therapy in Calcium Channel Blocker and β-blocker OverdoseFitra AlfaniNo ratings yet
- COVID-19 PKPD Treatment VietnamDocument27 pagesCOVID-19 PKPD Treatment VietnamNhanLiNo ratings yet
- Pin Sky PresentationDocument9 pagesPin Sky Presentationapi-3851462No ratings yet
- Hypertension in Dialysis PatientsDocument16 pagesHypertension in Dialysis PatientsSaad Anwar GujjarNo ratings yet
- PharmacologyDocument22 pagesPharmacologytayyaba riazNo ratings yet
- CPG Diabetic NephropathyDocument23 pagesCPG Diabetic NephropathyapalaginihNo ratings yet
- Algoritmo. ADA Management Patients DKA UpToDateDocument1 pageAlgoritmo. ADA Management Patients DKA UpToDateEMELYN YASMIN FIGUEROA HUANCANo ratings yet
- First-Line Anti-Ischaemic Agents Use and Long-Term Clinical Outcomes in Stable Coronary Artery Disease. Insights From The CLARIFY RegistryDocument18 pagesFirst-Line Anti-Ischaemic Agents Use and Long-Term Clinical Outcomes in Stable Coronary Artery Disease. Insights From The CLARIFY RegistryDenisseRangelNo ratings yet
- KDIGO 2024 ANCA Vasculitis Guideline Executive Sum - 240226 - 085441Document3 pagesKDIGO 2024 ANCA Vasculitis Guideline Executive Sum - 240226 - 085441Rossio Ortuño LoboNo ratings yet
- SFMH Mental Health AssessmentDocument24 pagesSFMH Mental Health AssessmentKholiwe Cassie MasekwaneNo ratings yet
- Updates in The Management of Diabetic Ketoacidosis: Kathryn Evans Kreider, DNP, FNP-BCDocument7 pagesUpdates in The Management of Diabetic Ketoacidosis: Kathryn Evans Kreider, DNP, FNP-BCLenin Zavaleta RodriguezNo ratings yet
- Cannabis For The Treatment of Attention Deficit Hyperactivity Disorder: A Report of 3 CasesDocument6 pagesCannabis For The Treatment of Attention Deficit Hyperactivity Disorder: A Report of 3 CasesGiulia PierroNo ratings yet
- Pathophysiology & Therapeutics IDocument454 pagesPathophysiology & Therapeutics IMuhammad AbdullahiNo ratings yet
- Drug Study SodiumbicarbonateDocument3 pagesDrug Study SodiumbicarbonatePao LaurenteNo ratings yet
- Apixaban Eliquis MonographDocument14 pagesApixaban Eliquis MonographTran Minh NgocNo ratings yet
- July Aug 2009Document7 pagesJuly Aug 2009sourabh koseyNo ratings yet
- AKI Vs CKD Lecture Latest 3rd Dec 2018Document51 pagesAKI Vs CKD Lecture Latest 3rd Dec 2018mugilessNo ratings yet
- Chronic Kidney Disease Bhakti MuliaDocument24 pagesChronic Kidney Disease Bhakti MuliaCOVID RSHJNo ratings yet
- Dasatinib Monograph 1mar2017Document8 pagesDasatinib Monograph 1mar2017Fandi HarmikiNo ratings yet
- 6.Z8sNyP 6 GHafez HT and Antihypertensive DrugsDocument81 pages6.Z8sNyP 6 GHafez HT and Antihypertensive Drugsyasmin.rahmany03No ratings yet
- Diabetes Mellitus: Geriatrics Evaluation & ManagementDocument4 pagesDiabetes Mellitus: Geriatrics Evaluation & ManagementAngeles SlzrNo ratings yet
- TM CKD2 - Case Discussion 2Document27 pagesTM CKD2 - Case Discussion 2KKNo ratings yet
- Alcoholic Liver DiseaseDocument60 pagesAlcoholic Liver Diseasegarychia100% (1)
- Nonalcoholic Fatty Liver DiseaseDocument4 pagesNonalcoholic Fatty Liver DiseaseAshvanee sharmaNo ratings yet
- Cost-Effectiveness of Alcohol Use Treatments in Patients With Alcohol-Related CirrhosisDocument9 pagesCost-Effectiveness of Alcohol Use Treatments in Patients With Alcohol-Related CirrhosisTIARA AMELIANo ratings yet
- Jurnal CaseDocument4 pagesJurnal CaseVivi DeviyanaNo ratings yet
- Bempedoic AcidDocument16 pagesBempedoic AcidSanjiv KlerNo ratings yet
- Lower Is Better - FinalDocument91 pagesLower Is Better - FinalJamsidul Hassan RajibNo ratings yet
- Study Some Important Biomarkers in Patients With Chronic Kidney DiseaseDocument7 pagesStudy Some Important Biomarkers in Patients With Chronic Kidney DiseaseCentral Asian StudiesNo ratings yet
- Iptec Taching Portfolio Midpoint ReviewDocument2 pagesIptec Taching Portfolio Midpoint Reviewapi-648401824No ratings yet
- Abx DeescalationDocument44 pagesAbx Deescalationapi-648401824No ratings yet
- Teaching Evaluation Feedback - Antibiotic DeescalationDocument9 pagesTeaching Evaluation Feedback - Antibiotic Deescalationapi-648401824No ratings yet
- Phenobarbital Nursing EducationDocument2 pagesPhenobarbital Nursing Educationapi-648401824No ratings yet
- Medication BasicsDocument2 pagesMedication Basicsapi-648401824No ratings yet
- Student Evals EtohDocument3 pagesStudent Evals Etohapi-648401824No ratings yet
- Spring Appe Preceptor FeedbackDocument4 pagesSpring Appe Preceptor Feedbackapi-648401824No ratings yet
- Cirrhosis With SBPDocument22 pagesCirrhosis With SBPapi-648401824No ratings yet
- Cardiac ArrestDocument4 pagesCardiac Arrestapi-648401824No ratings yet
- Diabetes Management in The Inpt SettingDocument3 pagesDiabetes Management in The Inpt Settingapi-648401824No ratings yet
- Student Feedback Fall 2022Document4 pagesStudent Feedback Fall 2022api-648401824No ratings yet
- Roberto Del RosarioDocument19 pagesRoberto Del RosarioCarl llamasNo ratings yet
- Georgia Habitats Lesson PlansDocument5 pagesGeorgia Habitats Lesson PlansBecky BrownNo ratings yet
- 7th Chemistry DLP Study Package FinalDocument101 pages7th Chemistry DLP Study Package FinalAdityaNo ratings yet
- GFRC Floating Concrete Hearth For Concrete Wood FiDocument11 pagesGFRC Floating Concrete Hearth For Concrete Wood FiJuliano. PQMNo ratings yet
- E TIMA News Letter November 2016 2 Min - CompressedDocument39 pagesE TIMA News Letter November 2016 2 Min - Compressedasidique5_292665351No ratings yet
- NUMBERS 2 Percentage ChangeDocument2 pagesNUMBERS 2 Percentage ChangeDinangaNo ratings yet
- Animal 1414Document6 pagesAnimal 1414trialink minsanNo ratings yet
- S800 SCL SR - 2CCC413009B0201 PDFDocument16 pagesS800 SCL SR - 2CCC413009B0201 PDFBalan PalaniappanNo ratings yet
- Construction and Building Materials: Paolo ForaboschiDocument21 pagesConstruction and Building Materials: Paolo ForaboschiMarco CamposNo ratings yet
- BotanyDocument11 pagesBotanyGirish GuptaNo ratings yet
- RS68-120 MLN ManuelDocument28 pagesRS68-120 MLN ManuelUmar MajeedNo ratings yet
- Vandex Plug: Rapid-Setting, Crystalline Hydraulic CementDocument2 pagesVandex Plug: Rapid-Setting, Crystalline Hydraulic CementQuerubin EboliNo ratings yet
- Recognizing and Classifying Daily Human Activities: Group-22Document23 pagesRecognizing and Classifying Daily Human Activities: Group-22Divyam GuptaNo ratings yet
- 22.anaerobes (Part II)Document91 pages22.anaerobes (Part II)sigrid jaramilloNo ratings yet
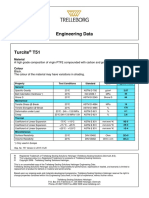
- Turcite T51 Engineering DataDocument1 pageTurcite T51 Engineering DataAntonio Rivera VillavicencioNo ratings yet
- EngineeringDocument107 pagesEngineeringSuezakumeNo ratings yet
- January 2005 6677 Mechanics M1: Mark SchemeDocument7 pagesJanuary 2005 6677 Mechanics M1: Mark SchemeWael TareqNo ratings yet
- Stationery Stock CardDocument100 pagesStationery Stock CardHuny BunyNo ratings yet
- The National TerritoryDocument39 pagesThe National TerritoryRan RanNo ratings yet
- Dr. M. Syed Jamil Asghar: Paper Published: 80Document6 pagesDr. M. Syed Jamil Asghar: Paper Published: 80Awaiz NoorNo ratings yet
- Car Frontal ImpactDocument25 pagesCar Frontal Impactapi-3762972100% (1)
- Manual HB ISM112 EDocument106 pagesManual HB ISM112 EALFAKNo ratings yet