You might also like
- Association Between Intrahepatic Cholestasis in Pregnancy and Gestational Diabetes Mellitus. A Retrospective AnalysisDocument6 pagesAssociation Between Intrahepatic Cholestasis in Pregnancy and Gestational Diabetes Mellitus. A Retrospective AnalysisDr.Karima EldarhobiNo ratings yet
- JurnalDocument32 pagesJurnalVivi Rizki YusufNo ratings yet
- GHTNDocument6 pagesGHTNDelavemia RostianiNo ratings yet
- Nausea and Vomiting in Pregnancy: MedicineDocument8 pagesNausea and Vomiting in Pregnancy: Medicineapi-315854829No ratings yet
- Sirichotiyakul 2016Document5 pagesSirichotiyakul 2016Atul GargNo ratings yet
- Determinants of PreDocument9 pagesDeterminants of PreAr OnaNo ratings yet
- Summary of The NHLBI Working Group On Research On Hypertension During PregnancyDocument9 pagesSummary of The NHLBI Working Group On Research On Hypertension During PregnancycarlosarmijoNo ratings yet
- Uric Acid Is As Important As Proteinuria in Identifying Fetal Risk in Women With Gestational HypertensionDocument8 pagesUric Acid Is As Important As Proteinuria in Identifying Fetal Risk in Women With Gestational HypertensionNurul Rizqan SeptimaNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 9: GynecologyFrom EverandComplementary and Alternative Medical Lab Testing Part 9: GynecologyNo ratings yet
- Paguidian, Griffin John D. Bsn4ADocument10 pagesPaguidian, Griffin John D. Bsn4AGj PaguidianNo ratings yet
- Nidhi Thesis PresentationDocument25 pagesNidhi Thesis Presentationujjwal souravNo ratings yet
- Umanand Prasad School of Medicine and Health ScienceDocument13 pagesUmanand Prasad School of Medicine and Health ScienceShakshi RainaNo ratings yet
- Recurrence of Hyperemesis GravidarumDocument10 pagesRecurrence of Hyperemesis Gravidarumnadyanatasya7No ratings yet
- The Management of Polycystic Ovary Syndrome: Vincenza Bruni, Metella Dei, Valentina Pontello, and Paolo VangelistiDocument15 pagesThe Management of Polycystic Ovary Syndrome: Vincenza Bruni, Metella Dei, Valentina Pontello, and Paolo VangelistiDaniela UrreaNo ratings yet
- Keywords: Pre-Eclampsia, Diagnosis, Risk Factors, Complications, Management, AnesthesiaDocument14 pagesKeywords: Pre-Eclampsia, Diagnosis, Risk Factors, Complications, Management, AnesthesiaAyu W. AnggreniNo ratings yet
- Early - and Late-Onset Preeclampsia A ComprehensiveDocument10 pagesEarly - and Late-Onset Preeclampsia A ComprehensiveEriekafebriayana RNo ratings yet
- Management Emesis GravidarumDocument8 pagesManagement Emesis GravidarumDewi KurniasariNo ratings yet
- Effect of Maternal Anaemia On Birth Weight: Original ArticleDocument3 pagesEffect of Maternal Anaemia On Birth Weight: Original ArticleTsulasatul HafidhohNo ratings yet
- Nausea and Vomiting of Pregnancy - PMCDocument33 pagesNausea and Vomiting of Pregnancy - PMCWidad SalsabilaNo ratings yet
- BJOG - 2020 - Perry - Maternal Haemodynamic Function Differs in Pre Eclampsia When It Is Associated With ADocument9 pagesBJOG - 2020 - Perry - Maternal Haemodynamic Function Differs in Pre Eclampsia When It Is Associated With AHanifa W PNo ratings yet
- Study of Sociodemographic Profile, Maternal, Fetal Outcome in Preeclamptic and Eclamptic Women A Prospective StudyDocument6 pagesStudy of Sociodemographic Profile, Maternal, Fetal Outcome in Preeclamptic and Eclamptic Women A Prospective StudyHarvey MatbaganNo ratings yet
- Impact of Pregnancy-Induced Hypertension On Fetal Growth: Rima Irwinda, Raymond Surya, Lidia F. NemboDocument8 pagesImpact of Pregnancy-Induced Hypertension On Fetal Growth: Rima Irwinda, Raymond Surya, Lidia F. NemboPramatama AndhikaNo ratings yet
- Hyperemesis Gravidarum 2019 NatureDocument17 pagesHyperemesis Gravidarum 2019 NatureResidentes GinecologíaNo ratings yet
- Pattern of Glucose Intolerance Among Pregnant Women With Unexplained IUFDDocument5 pagesPattern of Glucose Intolerance Among Pregnant Women With Unexplained IUFDTri UtomoNo ratings yet
- Research ArticleDocument7 pagesResearch ArticleTieti IsaniniNo ratings yet
- Article PublishedDocument5 pagesArticle PublishedKamran AmeerNo ratings yet
- Does Pre-Pregnancy BMI Determine Blood Pressure During Pregnancy? A Prospective Cohort StudyDocument17 pagesDoes Pre-Pregnancy BMI Determine Blood Pressure During Pregnancy? A Prospective Cohort StudyyundaNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 10: ObstetricsFrom EverandComplementary and Alternative Medical Lab Testing Part 10: ObstetricsNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 15: MusculoskeletalFrom EverandComplementary and Alternative Medical Lab Testing Part 15: MusculoskeletalNo ratings yet
- 4 ArticuloDocument9 pages4 ArticuloIsabella Orozco HdezNo ratings yet
- Acog Nausea Vomiting PregnancyDocument13 pagesAcog Nausea Vomiting PregnancymispNo ratings yet
- Pregnancy Outcomes in Familial Hypercholesterolemia: Epidemiology and PreventionDocument10 pagesPregnancy Outcomes in Familial Hypercholesterolemia: Epidemiology and PreventionsenkonenNo ratings yet
- Clinical Study of Retinal Changes in Pregnancy Induced HypertensionDocument5 pagesClinical Study of Retinal Changes in Pregnancy Induced HypertensionIJAR JOURNALNo ratings yet
- Maternal Serum Triglycerides in Women With Pre-Eclampsia: Original ArticleDocument5 pagesMaternal Serum Triglycerides in Women With Pre-Eclampsia: Original ArticleGladys SusantyNo ratings yet
- Pregnancy Complications in Women With PCOS: A Meta-Analysis: KM Tanvir and Mohammad Lutfor RahmanDocument6 pagesPregnancy Complications in Women With PCOS: A Meta-Analysis: KM Tanvir and Mohammad Lutfor Rahmanmr1998goNo ratings yet
- Chronic Hypertension in Pregnancy: Clinical PracticeDocument8 pagesChronic Hypertension in Pregnancy: Clinical PracticecornelNo ratings yet
- Effects of Blood Pressure Level Management On Maternal and Perinatal Outcomes in Pregnant Women With Mild To Moderate Gestational HypertensionDocument9 pagesEffects of Blood Pressure Level Management On Maternal and Perinatal Outcomes in Pregnant Women With Mild To Moderate Gestational HypertensionSri ayu maryaniNo ratings yet
- Differentiating Between Gestational and Chronic Hyper-Tension An Explorative StudyDocument6 pagesDifferentiating Between Gestational and Chronic Hyper-Tension An Explorative StudyVera Gardasevic MitrovicNo ratings yet
- Jurnal CohortDocument21 pagesJurnal CohortAstri Anindita UtomoNo ratings yet
- Sindrom Hellp PartialDocument5 pagesSindrom Hellp PartialodellistaNo ratings yet
- 82085243 case-study-on-pregnancy-induced-hypertension-eclampsiaDocument13 pages82085243 case-study-on-pregnancy-induced-hypertension-eclampsiashakuntla Devi0% (2)
- Zona Kedokteran - Vol. 11 No. 2 Mei 2021: Correlation Age and Parity With Hiperemesis GravidarumDocument6 pagesZona Kedokteran - Vol. 11 No. 2 Mei 2021: Correlation Age and Parity With Hiperemesis GravidarumTeuku Ilham AkbarNo ratings yet
- Haematocrit Value in Preeclampsia: AbstractDocument6 pagesHaematocrit Value in Preeclampsia: AbstractViraj SenavirathneNo ratings yet
- Pregestational Diabetes and Fetal Heart Rate in The First Trimester of PregnancyDocument4 pagesPregestational Diabetes and Fetal Heart Rate in The First Trimester of PregnancyMifta S P NingrumNo ratings yet
- Hyperemesis GravidarumDocument19 pagesHyperemesis Gravidarumdeneke100% (1)
- Hypertension During PregnancyDocument9 pagesHypertension During PregnancyNera MayaditaNo ratings yet
- Is Fetal Growth Restriction Associated With A More Severe Maternal Phenotype in The Setting of Early Onset Pre-Eclampsia? A Retrospective StudyDocument6 pagesIs Fetal Growth Restriction Associated With A More Severe Maternal Phenotype in The Setting of Early Onset Pre-Eclampsia? A Retrospective StudyYessie ErNo ratings yet
- Pregnancy Complications and Outcomes in Women With Epilepsy: Mirzaei Fatemeh, Ebrahimi B. NazaninDocument5 pagesPregnancy Complications and Outcomes in Women With Epilepsy: Mirzaei Fatemeh, Ebrahimi B. NazaninMentari SetiawatiNo ratings yet
- Literature Review of Hypertension in PregnancyDocument7 pagesLiterature Review of Hypertension in Pregnancyc5jbmre7100% (1)
- Art 1Document17 pagesArt 1Luis GuevaraNo ratings yet
- Perinatal - Outcome - in - Oligohydramnios SynopsisDocument16 pagesPerinatal - Outcome - in - Oligohydramnios SynopsisdhanrajramotraNo ratings yet
- Pregnancy Induced Hypertension Case StudyDocument77 pagesPregnancy Induced Hypertension Case StudyJoe Anne Maniulit, MSN, RN84% (49)
- Pregnancy Outcome in 396 Pregnancies in Patients With SLE in Saudi ArabiaDocument10 pagesPregnancy Outcome in 396 Pregnancies in Patients With SLE in Saudi ArabiaLaura Isabel JaramilloNo ratings yet
- Metanalisis de Los Resultados Del Embarazo en Mujeres Con Nefritis LupicaDocument17 pagesMetanalisis de Los Resultados Del Embarazo en Mujeres Con Nefritis LupicabLANCAFARFANNo ratings yet
- Jurnal 6Document8 pagesJurnal 6Bayek NgekekNo ratings yet
- Internal Medicine Zafar Uric Acid PDFDocument38 pagesInternal Medicine Zafar Uric Acid PDFdwiNo ratings yet
- Pre-Existing Diabetes Mellitus and Adverse PDFDocument5 pagesPre-Existing Diabetes Mellitus and Adverse PDFMetebNo ratings yet
- Changes in Pulmonary Function During Pregnancy: A Longitudinal Cohort StudyDocument8 pagesChanges in Pulmonary Function During Pregnancy: A Longitudinal Cohort StudyFaizah ShabrinaNo ratings yet
- Chronic Hypertension in Pregnancy: Clinical PracticeDocument8 pagesChronic Hypertension in Pregnancy: Clinical PracticeemmoyNo ratings yet
- Original Research PaperDocument4 pagesOriginal Research PaperOviya ChitharthanNo ratings yet
- Ciguatera Fish Poisoning: Symptoms and TreatmentDocument2 pagesCiguatera Fish Poisoning: Symptoms and TreatmentdenardNo ratings yet
- Insurance Proposal GuidelinesDocument6 pagesInsurance Proposal GuidelinesBose GRNo ratings yet
- MCQ Final 1984Document19 pagesMCQ Final 1984JohnSonNo ratings yet
- Prepositions-Of-Time-Grammar-Guides - Sin RespuestaDocument1 pagePrepositions-Of-Time-Grammar-Guides - Sin RespuestaCarla BonanoNo ratings yet
- Table of Genetic DisordersDocument3 pagesTable of Genetic DisordersEliNo ratings yet
- Askep Bahasa Inggris SaneDocument12 pagesAskep Bahasa Inggris SaneRio FernandoNo ratings yet
- 2 ApendixDocument8 pages2 Apendixمحمد عماد عليNo ratings yet
- Aa by AbdifatahDocument57 pagesAa by AbdifatahAbdifatah AhmedNo ratings yet
- Human Sciences ToK - PsychologyDocument9 pagesHuman Sciences ToK - PsychologyOliver Emmet  THOMPSONNo ratings yet
- NLE 08 Test IDocument7 pagesNLE 08 Test IBrenlei Alexis NazarroNo ratings yet
- End of Life CareDocument18 pagesEnd of Life CareselvarajNo ratings yet
- Lecture 5.3 Metabolic Errors of Carbohydrates PART 3Document8 pagesLecture 5.3 Metabolic Errors of Carbohydrates PART 3Huzaifa MehmoodNo ratings yet
- Monkey Pox Fact SheetDocument3 pagesMonkey Pox Fact SheetMalcolm M. LeeNo ratings yet
- Taylor GLN CH 31Document4 pagesTaylor GLN CH 31Karen Mae AlcantaraNo ratings yet
- Personal LetterDocument7 pagesPersonal LetterSMK MutiaraNo ratings yet
- CardiologíaDocument3 pagesCardiologíajakpowerNo ratings yet
- Hookworm Infection - UpToDateDocument12 pagesHookworm Infection - UpToDatedesilasarybasriNo ratings yet
- Diabetic Ketoacidosis Care Guideline EdDocument2 pagesDiabetic Ketoacidosis Care Guideline EdSeno Adi WicaksonoNo ratings yet
- Medical Certificate for Cough, Sore Throat, HeadacheDocument1 pageMedical Certificate for Cough, Sore Throat, HeadacheJareena SamsonNo ratings yet
- HOMEOPATHIC CASE FORMATDocument21 pagesHOMEOPATHIC CASE FORMATSatyendra Rawat43% (7)
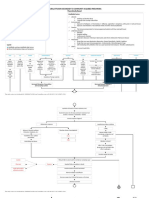
- Acute Renal Failure: Presented by Peter Fumo, MD, FACPDocument20 pagesAcute Renal Failure: Presented by Peter Fumo, MD, FACPlagathurcNo ratings yet
- WS BG3 M01 L17 Grammar ROOM2Document2 pagesWS BG3 M01 L17 Grammar ROOM2Paola MartínezNo ratings yet
- India Pharmaceutical Market Growth to Accelerate by 2030Document14 pagesIndia Pharmaceutical Market Growth to Accelerate by 2030Naveena ShreeNo ratings yet
- Case 14-2020: A 37-Year-Old Man With Joint Pain and Eye RednessDocument9 pagesCase 14-2020: A 37-Year-Old Man With Joint Pain and Eye RednessGénesis LeónNo ratings yet
- Pleural Effusion Secondary To Community Acquired Pneumonia PathophysiologyDocument5 pagesPleural Effusion Secondary To Community Acquired Pneumonia PathophysiologySteffiNo ratings yet
- Comcogtable 3 Summary All TestsDocument17 pagesComcogtable 3 Summary All TestsanamariapobleteNo ratings yet
- Nisa's eye exam diagnosesDocument4 pagesNisa's eye exam diagnosesNisaadivaNo ratings yet
- Stanley T. Agor, MD, DPPS, MSPH Department of Pediatrics Cagayan Valley Medical CenterDocument35 pagesStanley T. Agor, MD, DPPS, MSPH Department of Pediatrics Cagayan Valley Medical CenterLuis PadillaNo ratings yet
- Rumination Disorder Research and Case StudiesDocument19 pagesRumination Disorder Research and Case StudiesJaya TevesNo ratings yet
- Homelessness and Burns - Joan ChenDocument16 pagesHomelessness and Burns - Joan ChenJjoan ChchenNo ratings yet