You might also like
- Newapproachestopain Management: Orrett E. OgleDocument10 pagesNewapproachestopain Management: Orrett E. OgleNajeeb UllahNo ratings yet
- Jurnal - Relief of PainDocument6 pagesJurnal - Relief of PainChandra NepaNo ratings yet
- Dental Pulp Testing - A ReviewDocument12 pagesDental Pulp Testing - A ReviewSara Loureiro da LuzNo ratings yet
- Odontogenic Pain: Goranka Prpić-Mehičić, Nada GalićDocument12 pagesOdontogenic Pain: Goranka Prpić-Mehičić, Nada Galićsam888xoxoNo ratings yet
- JurnalDocument12 pagesJurnalRestia07RahmaNo ratings yet
- Flare Ups in EndodonticsDocument12 pagesFlare Ups in EndodonticsAnamika Thakur RanaNo ratings yet
- Pain Management in Dentistry: Jeff Burgess, DDS, MSD (Retired) Clinical Assistant Professor, Department ofDocument14 pagesPain Management in Dentistry: Jeff Burgess, DDS, MSD (Retired) Clinical Assistant Professor, Department ofStefanus TabboNo ratings yet
- Vitality TestDocument13 pagesVitality TestSwathyNo ratings yet
- Nerve Injury Following A Mandibular BlockDocument7 pagesNerve Injury Following A Mandibular BlockKranti PrajapatiNo ratings yet
- Phantom Tooth PainDocument31 pagesPhantom Tooth PainMuchlis Fauzi ENo ratings yet
- PDF 20230624 122205 0000Document36 pagesPDF 20230624 122205 0000Maria EvergardenNo ratings yet
- Review Article: The Use of Technology in The Management of Orthodontic Treatment-Related PainDocument5 pagesReview Article: The Use of Technology in The Management of Orthodontic Treatment-Related PainDnys SetiabudiNo ratings yet
- Flare Ups in Endodontics - 1 Etiological FactorsDocument6 pagesFlare Ups in Endodontics - 1 Etiological FactorsdrshravyaNo ratings yet
- The Use of Non-Steroidal Anti-Inflammatory Drugs in Phonophoresis Treatment For Knee Osteoarthritis: A Literature ReviewDocument8 pagesThe Use of Non-Steroidal Anti-Inflammatory Drugs in Phonophoresis Treatment For Knee Osteoarthritis: A Literature Reviewapi-515423744No ratings yet
- Effects of Physical Stimulation in The Field of Oral HealthDocument17 pagesEffects of Physical Stimulation in The Field of Oral HealthsovalaxNo ratings yet
- Wa0007Document17 pagesWa0007Eko WidodoNo ratings yet
- Pain Pathways and Mechanisms of the Pulpodentin ComplexDocument9 pagesPain Pathways and Mechanisms of the Pulpodentin ComplexKyucha ChanNo ratings yet
- Dentin Hypersensitivity: Etiology, Diagnosis and Treatment A Literature ReviewDocument13 pagesDentin Hypersensitivity: Etiology, Diagnosis and Treatment A Literature ReviewViliya QodriyaniNo ratings yet
- Tratamiento TendinopatiaDocument16 pagesTratamiento TendinopatiasputnickNo ratings yet
- Flare Up in Endodontics: A Review: Tharangini Raveenthiraraja, Pradeep SoleteDocument3 pagesFlare Up in Endodontics: A Review: Tharangini Raveenthiraraja, Pradeep SoleteDarshilNo ratings yet
- Hargreaves 1994Document8 pagesHargreaves 1994AbeerNo ratings yet
- Allergic Rhinitis July 2011Document7 pagesAllergic Rhinitis July 2011aswadiibrahimNo ratings yet
- Treatment of Tendinopathy What Works, What Does Not, and What Is On The Horizon PDFDocument16 pagesTreatment of Tendinopathy What Works, What Does Not, and What Is On The Horizon PDFFranciscoJavierRoblesNo ratings yet
- The Painful Tooth - Mechanisms, Presentation and Differential Diagnosis of Odontogenic PainDocument19 pagesThe Painful Tooth - Mechanisms, Presentation and Differential Diagnosis of Odontogenic Painbyun sugaNo ratings yet
- Current Advances in Orthodontic Pain: ReviewDocument9 pagesCurrent Advances in Orthodontic Pain: ReviewCamila Alvarez GaravitoNo ratings yet
- Children: Acupuncture For Pediatric PainDocument15 pagesChildren: Acupuncture For Pediatric PainRachel GreeneNo ratings yet
- Completed Research PaperDocument14 pagesCompleted Research Paperapi-545708059No ratings yet
- Hot Tooth - A Challenge To EndodontistsDocument5 pagesHot Tooth - A Challenge To EndodontistsShameena KnNo ratings yet
- The Effects of Commonly Used Drugs On Orthodontic Tooth Movement: A Systematic ReviewDocument5 pagesThe Effects of Commonly Used Drugs On Orthodontic Tooth Movement: A Systematic ReviewvprakshaindiaNo ratings yet
- 6 A-Hot ToothDocument14 pages6 A-Hot ToothYadnesh DondulkarNo ratings yet
- Medip, IJCMPH-9190 RDocument5 pagesMedip, IJCMPH-9190 RSimona BudauNo ratings yet
- Analgesia y Anestesia Oral en Perro y Gato VCSADocument18 pagesAnalgesia y Anestesia Oral en Perro y Gato VCSAValentina AmayaNo ratings yet
- Hot Tooth - A Challenge To EndodontistsDocument5 pagesHot Tooth - A Challenge To EndodontistsSomansh GoyalNo ratings yet
- Pain ControlDocument33 pagesPain ControlOussama BenaliNo ratings yet
- Hot Tooth - A Challenge To EndodontistsDocument5 pagesHot Tooth - A Challenge To EndodontistsKalpanaNo ratings yet
- Treatment of Tic EmergenciesDocument7 pagesTreatment of Tic Emergenciesinalcp290891No ratings yet
- 10 1179@0886963413z 0000000002Document7 pages10 1179@0886963413z 0000000002hilderhNo ratings yet
- 3 - Pulpal and Periradicular PathosisDocument10 pages3 - Pulpal and Periradicular PathosisZaid AKNo ratings yet
- Journal Pre-ProofDocument26 pagesJournal Pre-ProofcatalinaNo ratings yet
- Chronic Facial Pain Guide: Causes, Symptoms & TreatmentsDocument5 pagesChronic Facial Pain Guide: Causes, Symptoms & TreatmentsdamarstationNo ratings yet
- AnalgesikDocument25 pagesAnalgesikernha watiNo ratings yet
- Pain AssessmentDocument11 pagesPain AssessmentSuvadip MaityNo ratings yet
- DikonversiDocument17 pagesDikonversiAkbar FitryansyahNo ratings yet
- OPERATORIA. Henry A. Gremillion Multidisciplinary Diagnosis and Management of Orofacial PainDocument13 pagesOPERATORIA. Henry A. Gremillion Multidisciplinary Diagnosis and Management of Orofacial PainKenigal14No ratings yet
- Halpern 2016Document25 pagesHalpern 2016SAYDE ILEANA NAJERA DOMINGUEZNo ratings yet
- Clinical Classification of The Status of The Pulp and Dental HealthDocument15 pagesClinical Classification of The Status of The Pulp and Dental HealthrahaazadNo ratings yet
- Effect of Desensitizing Patch For Dentin Hypersensitivity: Su-Yeon Park, Mi-Ra Lee, Jin-Hee WonDocument7 pagesEffect of Desensitizing Patch For Dentin Hypersensitivity: Su-Yeon Park, Mi-Ra Lee, Jin-Hee WonIndah LestariNo ratings yet
- Management of Mid-Treatment Endodontics Flare-UpsDocument33 pagesManagement of Mid-Treatment Endodontics Flare-UpsWreq SurrenNo ratings yet
- Intratympanic Bupivacaine Instillation For Tinnitus Treatment?Document4 pagesIntratympanic Bupivacaine Instillation For Tinnitus Treatment?Novita WulandariNo ratings yet
- Atypical OdontalgiaDocument5 pagesAtypical OdontalgiaMaria Putri NasutionNo ratings yet
- Thesis On Facial PalsyDocument8 pagesThesis On Facial Palsymelissalongmanchester100% (2)
- A Future Without Chronic Pain: Neuroscience and Clinical Research by David Borsook, M.D., PH.DDocument16 pagesA Future Without Chronic Pain: Neuroscience and Clinical Research by David Borsook, M.D., PH.DZmajNo ratings yet
- PainDocument13 pagesPainGhufran KhalilNo ratings yet
- Painful NeuropathiesDocument6 pagesPainful NeuropathiesAgusBhaktiNo ratings yet
- SWD For SinusesDocument9 pagesSWD For SinusesFaisal QureshiNo ratings yet
- Diagnosis and Treatment of Chronic CoughFrom EverandDiagnosis and Treatment of Chronic CoughSang Heon ChoNo ratings yet
- Ccide 6 045Document12 pagesCcide 6 045Karissa NavitaNo ratings yet
- Physiotherapy Management of SciaticaDocument6 pagesPhysiotherapy Management of SciaticaMuly Arafah ZakariaNo ratings yet
- Trauma Medular Cervical en Pacientes Con OsificaciDocument11 pagesTrauma Medular Cervical en Pacientes Con OsificaciLeticia RiveraNo ratings yet
- Electroestimulacion Funcional INGLESDocument9 pagesElectroestimulacion Funcional INGLESLeticia RiveraNo ratings yet
- Malformations of The Tooth Root in Humans PDFDocument16 pagesMalformations of The Tooth Root in Humans PDFLeticia RiveraNo ratings yet
- Art2 Para+publicarDocument9 pagesArt2 Para+publicarLeticia RiveraNo ratings yet
- Three-Rooted Maxillary PremolarsDocument2 pagesThree-Rooted Maxillary PremolarsLeticia RiveraNo ratings yet
- Endodontic Treatment of A Mandibular Second Premolar With Three Roots and Three CanalsDocument3 pagesEndodontic Treatment of A Mandibular Second Premolar With Three Roots and Three CanalsLeticia RiveraNo ratings yet
- Incidence and Factors Associated With Flare-Ups in A Post Graduate Programme in The Indian PopulationDocument6 pagesIncidence and Factors Associated With Flare-Ups in A Post Graduate Programme in The Indian PopulationLeticia RiveraNo ratings yet
- Digital vs. conventional radiography for root canal lengthDocument4 pagesDigital vs. conventional radiography for root canal lengthNitesh SanghviNo ratings yet
- Endodontic Flare-Ups Comparison of Incidence Between Single and Multiple Visit Procedures in Patients Attending A Nigerian Teaching HospitalDocument6 pagesEndodontic Flare-Ups Comparison of Incidence Between Single and Multiple Visit Procedures in Patients Attending A Nigerian Teaching HospitalLeticia RiveraNo ratings yet
- Digital vs. conventional radiography for root canal lengthDocument4 pagesDigital vs. conventional radiography for root canal lengthNitesh SanghviNo ratings yet
- Comparison of Radiographic Measurements Obtained With Conventional and Indirect Digital Imaging During Endodontic TreatmentDocument4 pagesComparison of Radiographic Measurements Obtained With Conventional and Indirect Digital Imaging During Endodontic TreatmentLeticia RiveraNo ratings yet
- Efficacy of Articaine vs Lidocaine for Treating Pulpitis: RCTDocument6 pagesEfficacy of Articaine vs Lidocaine for Treating Pulpitis: RCTLeticia RiveraNo ratings yet
- Efficacy of Prophylactic Use of Antibiotics To Avoid Flare Up During Root Canal Treatment of Nonvital Teeth A Randomized Clinical TrialDocument4 pagesEfficacy of Prophylactic Use of Antibiotics To Avoid Flare Up During Root Canal Treatment of Nonvital Teeth A Randomized Clinical TrialLeticia RiveraNo ratings yet
- X-Tip Intraosseous Injection System As A Primary Anesthesia For Irreversible Pulpitis of Posterior Mandibular Teeth A Randomized Clinical TrailDocument8 pagesX-Tip Intraosseous Injection System As A Primary Anesthesia For Irreversible Pulpitis of Posterior Mandibular Teeth A Randomized Clinical TrailLeticia RiveraNo ratings yet
- An in Vitro Comparison of Bond Strength of Different SealersObturation Systems To Root Dentin Using The Push-Out Test at 2 Weeks and 3 MonthsDocument6 pagesAn in Vitro Comparison of Bond Strength of Different SealersObturation Systems To Root Dentin Using The Push-Out Test at 2 Weeks and 3 MonthsLeticia RiveraNo ratings yet
- Comparison of Obturation Quality in Modified Continuous Wave Compaction, Continuous Wave Compaction, Lateral Compaction and Warm Vertical Compaction TechniquesDocument10 pagesComparison of Obturation Quality in Modified Continuous Wave Compaction, Continuous Wave Compaction, Lateral Compaction and Warm Vertical Compaction TechniquesHachko GiragosyanNo ratings yet
- Endodontic Treatment of A Maxillary First Premolar With Type IV Buccal Root Canal A Case ReportDocument2 pagesEndodontic Treatment of A Maxillary First Premolar With Type IV Buccal Root Canal A Case ReportLeticia RiveraNo ratings yet
- CBCT Joint Position StatementDocument6 pagesCBCT Joint Position StatementPaweł SieradzkiNo ratings yet
- Ultrasonic Cavity Preparation Using CVD Coated Diamond Bur A Case ReportDocument6 pagesUltrasonic Cavity Preparation Using CVD Coated Diamond Bur A Case ReportLeticia RiveraNo ratings yet
- A Comparative Clinical Evaluation of Accuracy of Six Apex Locators With Intraoral Periapical Radiograph in Multirooted Teeth An in Vivo StudyDocument10 pagesA Comparative Clinical Evaluation of Accuracy of Six Apex Locators With Intraoral Periapical Radiograph in Multirooted Teeth An in Vivo StudyLeticia RiveraNo ratings yet
- Working Length Determination Using Cone-Beam Computed Tomography, Periapical Radiography and Electronic Apex Locator in Teeth With Apical PeriodontitisDocument5 pagesWorking Length Determination Using Cone-Beam Computed Tomography, Periapical Radiography and Electronic Apex Locator in Teeth With Apical PeriodontitisLeticia RiveraNo ratings yet
- Comparing Root Canal Filling Techniques in Anterior TeethDocument5 pagesComparing Root Canal Filling Techniques in Anterior TeethLeticia RiveraNo ratings yet
- Cerebral VasculitisDocument46 pagesCerebral VasculitisMatteo PaolucciNo ratings yet
- Temperature Regulation and Monitoring-Samar TahaDocument57 pagesTemperature Regulation and Monitoring-Samar TahapaulaNo ratings yet
- Assignment #1Document6 pagesAssignment #1Leylu RepatoNo ratings yet
- Paracetamol Drug StudyDocument1 pageParacetamol Drug Studyrain peregrinoNo ratings yet
- Bioengineering Approaches To Controlled Protein DeliveryDocument7 pagesBioengineering Approaches To Controlled Protein DeliveryarisNo ratings yet
- ????? ?????????Document2 pages????? ?????????KIANA LOUISE ROMANONo ratings yet
- Antibiotic TableDocument5 pagesAntibiotic TableLiana Et Murat KalabalikNo ratings yet
- Precision Medicine in Lung CancerDocument12 pagesPrecision Medicine in Lung Cancerswastik panditaNo ratings yet
- Spinal and Epidural Anesthesia: Department of AnesthesiologyDocument42 pagesSpinal and Epidural Anesthesia: Department of AnesthesiologyCharisse Ann GasatayaNo ratings yet
- SOAP Note - Peter The DeanDocument5 pagesSOAP Note - Peter The DeanWu TracyNo ratings yet
- Essential List On 5th November 2022Document9 pagesEssential List On 5th November 2022AFI FARMANo ratings yet
- Medicines Management: To Be Viewed in Conjunction With NMC Standards For Medicines ManagementDocument20 pagesMedicines Management: To Be Viewed in Conjunction With NMC Standards For Medicines ManagementPranavjeet KaldateNo ratings yet
- Cell-Based Model of CoagulationDocument8 pagesCell-Based Model of CoagulationIULIU-CONSTANTIN MOCANUNo ratings yet
- JAAPA Article - Staying Up To Date With JNC 8 HTN Guideline - H FeldmanDocument7 pagesJAAPA Article - Staying Up To Date With JNC 8 HTN Guideline - H FeldmanNomar NonatoNo ratings yet
- GIT - Dr. Allam 2021 PDFDocument47 pagesGIT - Dr. Allam 2021 PDFMohammedNo ratings yet
- Ethinylestradiol 0.03mg + Drospirenone 3mg (Yasmin)Document18 pagesEthinylestradiol 0.03mg + Drospirenone 3mg (Yasmin)asdwasdNo ratings yet
- Neuropsychological Effects of Caffeine Is Caffeine Addictive 2161 0487 1000295 PDFDocument12 pagesNeuropsychological Effects of Caffeine Is Caffeine Addictive 2161 0487 1000295 PDFAli ShahNo ratings yet
- Diabetes Algorithm Executive SummaryDocument30 pagesDiabetes Algorithm Executive SummaryLuis Alberto Alvarez AnkassNo ratings yet
- Assignment 1: Renal Treatment: InstructionsDocument16 pagesAssignment 1: Renal Treatment: InstructionsAJ BayNo ratings yet
- Nursing Management of Breast CancerDocument12 pagesNursing Management of Breast CancerJanelle Cabida SupnadNo ratings yet
- Management of Cyanide PoisoningDocument3 pagesManagement of Cyanide PoisoningnadiaramadaniNo ratings yet
- Psychotherapeutic Drugs: Pam Pam LamDocument7 pagesPsychotherapeutic Drugs: Pam Pam Lamchubbygunny_29776413No ratings yet
- MED SURG Final CoachingDocument12 pagesMED SURG Final Coachingkim torino100% (1)
- 1 Acute Renal FailureDocument65 pages1 Acute Renal FailureDammaqsaa W BiyyanaaNo ratings yet
- Top 10 Most Anticipated Drug Launches of 2023Document14 pagesTop 10 Most Anticipated Drug Launches of 2023Radha RaniNo ratings yet
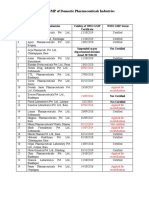
- Status of Nepali Pharma GMP CertificationDocument2 pagesStatus of Nepali Pharma GMP CertificationDapper Yourself100% (1)
- Legalization of Marijuana in The PhilippinesDocument12 pagesLegalization of Marijuana in The PhilippinesJenny ChavezNo ratings yet
- NAG Skin and Soft Tissue Infections AdultsDocument21 pagesNAG Skin and Soft Tissue Infections AdultsJun JimenezNo ratings yet
- Kerry Layne Author Albert Ferro Author 100 Cases in Clinical PharmacologyDocument249 pagesKerry Layne Author Albert Ferro Author 100 Cases in Clinical Pharmacologyteju100% (3)
- Drug Induced Movement DisordersDocument65 pagesDrug Induced Movement DisordersShaunak PatilNo ratings yet