You might also like
- Hotel Incident ReportDocument2 pagesHotel Incident ReportApirinmu100% (7)
- Incident Report - IOSHDocument4 pagesIncident Report - IOSHSarwo Edy PurnomoNo ratings yet
- Dobbs Issues COVID Isolation Order For Positive Cases in MississippiDocument3 pagesDobbs Issues COVID Isolation Order For Positive Cases in MississippiRuss Latino100% (1)
- Incident Report FormDocument2 pagesIncident Report FormAnku Kingsley Etornam100% (1)
- NHCA Health Club Incident RPT FormDocument2 pagesNHCA Health Club Incident RPT Formcrossfitvelocity982No ratings yet
- Hazard Identification-Incident Reporting FormDocument3 pagesHazard Identification-Incident Reporting FormgeoanburajaNo ratings yet
- Critical Incident Reporting Guideline and FormDocument8 pagesCritical Incident Reporting Guideline and FormkinyzoNo ratings yet
- Hazard Incident Report FormDocument2 pagesHazard Incident Report FormRamanaMurthy KotiNo ratings yet
- Near Miss or Incident InvestigationDocument4 pagesNear Miss or Incident InvestigationFahad AhmedNo ratings yet
- Sample Incident Investigation FormsDocument5 pagesSample Incident Investigation FormsshahbazchafekarNo ratings yet
- Incident ReportDocument2 pagesIncident ReportZyra AndoyNo ratings yet
- Employee Incident Report FormDocument2 pagesEmployee Incident Report FormDS SystemsNo ratings yet
- Incident/Near Miss Investigation FormDocument2 pagesIncident/Near Miss Investigation FormIrinel ApostuNo ratings yet
- Incident / Hazard Report Form: 1. Person Involved Details - Forward To Your Team Leader / Manager Within 24 HoursDocument3 pagesIncident / Hazard Report Form: 1. Person Involved Details - Forward To Your Team Leader / Manager Within 24 HourstitaandientiNo ratings yet
- Incident Report and Investigation FormDocument1 pageIncident Report and Investigation FormChristine KhoNo ratings yet
- First Aid Accident Form WPADocument2 pagesFirst Aid Accident Form WPAshaibaz chafekarNo ratings yet
- Accident Investigation Report: Adamson University College of Engineering Chemical Engineering DepartmentDocument7 pagesAccident Investigation Report: Adamson University College of Engineering Chemical Engineering DepartmentdhesNo ratings yet
- Workplace Violence Incident Report FormDocument3 pagesWorkplace Violence Incident Report Formamrpoiu2016No ratings yet
- FMT - 13.incident ReportDocument2 pagesFMT - 13.incident ReportDinesh BNo ratings yet
- Incident & Accident ReportDocument7 pagesIncident & Accident ReportleganzaNo ratings yet
- Sample Safety InspectionDocument3 pagesSample Safety InspectionEka FarmaNo ratings yet
- Incident / Hazard Report Form: 1. Person Involved Details - Forward To Your Team Leader / Manager Within 24 HoursDocument3 pagesIncident / Hazard Report Form: 1. Person Involved Details - Forward To Your Team Leader / Manager Within 24 HourstitaandientiNo ratings yet
- Making 3 Party Report Revised Event Summary: Street City State ZipDocument4 pagesMaking 3 Party Report Revised Event Summary: Street City State ZipCherylNo ratings yet
- Accident Reporting, Investigation & Analysis (CIF&B)Document47 pagesAccident Reporting, Investigation & Analysis (CIF&B)saraswatvoNo ratings yet
- Incident Intimation Cum Investigation ReportDocument1 pageIncident Intimation Cum Investigation ReportDenstun DSouzaNo ratings yet
- Accident and IncidentDocument1 pageAccident and Incidentkkhan.yasim75No ratings yet
- Pharmacy Level Iii: Learning Guide - 26Document21 pagesPharmacy Level Iii: Learning Guide - 26Belay KassahunNo ratings yet
- Incident and Accident Form: UI-61917-PGCC-HSSE-IAF 3.1Document4 pagesIncident and Accident Form: UI-61917-PGCC-HSSE-IAF 3.1benNo ratings yet
- GIL-ORGN-MGM-G-111-01 Action & Response Plan For Fatal AccidentsDocument7 pagesGIL-ORGN-MGM-G-111-01 Action & Response Plan For Fatal AccidentsRajarathinam1235463No ratings yet
- 1.SeriousAccidentGuestEmployee en May 2021Document3 pages1.SeriousAccidentGuestEmployee en May 2021mohammedboushib1965No ratings yet
- Incident ReportDocument3 pagesIncident Reportyakeshk5No ratings yet
- Incident Report InjuryDocument2 pagesIncident Report InjuryJovy Ann EsquilonaNo ratings yet
- Form G: Part A - Incident NotificationDocument7 pagesForm G: Part A - Incident NotificationFNo ratings yet
- Accident Form Template: Developed byDocument5 pagesAccident Form Template: Developed byEcinaj CabahugNo ratings yet
- Accident Form Template: Developed byDocument5 pagesAccident Form Template: Developed byj.andry. dprNo ratings yet
- 3CMA Crisis Handouts PacketDocument19 pages3CMA Crisis Handouts PacketTriton007No ratings yet
- Form Latihan HiraDocument20 pagesForm Latihan HiraFines AdemukhlisNo ratings yet
- 52 Near Miss Report Form 1903Document3 pages52 Near Miss Report Form 1903SamuelNo ratings yet
- Incident FormDocument2 pagesIncident FormdranilshindeNo ratings yet
- Template - Initial Notification Form 2018Document1 pageTemplate - Initial Notification Form 2018nagul kmtcNo ratings yet
- Incident Alert 001 - Incidente Operacional - Mina Islay - Ecosem HuaychaoDocument3 pagesIncident Alert 001 - Incidente Operacional - Mina Islay - Ecosem HuaychaoSEGURIDAD ECOSEM HNo ratings yet
- Hazard Report Form SampleDocument2 pagesHazard Report Form Samplewelly1980okNo ratings yet
- Borang Incident FinalDocument3 pagesBorang Incident FinalSarah EddiahNo ratings yet
- Incident Report FormDocument2 pagesIncident Report FormMuhammad Ibad AlamNo ratings yet
- Proposed Investigation FormDocument9 pagesProposed Investigation FormLawrence EnehNo ratings yet
- 4.AttemptedSuicideGuestEmployee - EN - May 2021Document3 pages4.AttemptedSuicideGuestEmployee - EN - May 2021mohammedboushib1965No ratings yet
- Incident Report Form: RPSG-IMS-F-24 Accident and Investigation Form 5ADocument2 pagesIncident Report Form: RPSG-IMS-F-24 Accident and Investigation Form 5ARocky BisNo ratings yet
- Dhs Ied Search ProceduresDocument72 pagesDhs Ied Search ProceduresRJay JacabanNo ratings yet
- Incident Report KosongDocument1 pageIncident Report KosongNada SantikaNo ratings yet
- ESR Form GrezDocument2 pagesESR Form Grezlizabernard.hernandezNo ratings yet
- Snap ReportDocument2 pagesSnap ReportJoseNo ratings yet
- Accident/Incident Report Section 1: Details of Person Making This ReportDocument2 pagesAccident/Incident Report Section 1: Details of Person Making This ReportAbdul RafeequeNo ratings yet
- QR-ADM-1010 Incident Report TPSMIDocument17 pagesQR-ADM-1010 Incident Report TPSMIHR SundiaNo ratings yet
- PCD-QSC-FMT-13 Accident-Incident Investigation ReportDocument2 pagesPCD-QSC-FMT-13 Accident-Incident Investigation ReportRami KhedroNo ratings yet
- Preca Solutions India PVT LTD: Accident / Incident Investigation ReportDocument8 pagesPreca Solutions India PVT LTD: Accident / Incident Investigation ReportMURTHYNo ratings yet
- Ovr New MohDocument2 pagesOvr New MohhyNo ratings yet
- Incident and Accident Report TemplateDocument4 pagesIncident and Accident Report TemplateKashifPervez1No ratings yet
- Inccident Investigation Form v5.0Document4 pagesInccident Investigation Form v5.0ahmedNo ratings yet
- The Manager’s Guide to Quick Crisis Response: Effective Action in an EmergencyFrom EverandThe Manager’s Guide to Quick Crisis Response: Effective Action in an EmergencyNo ratings yet
- Crisis Intervention Training for Disaster Workers: An IntroductionFrom EverandCrisis Intervention Training for Disaster Workers: An IntroductionRating: 4.5 out of 5 stars4.5/5 (3)
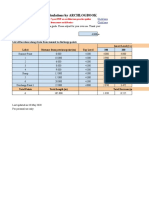
- Drainage Invert Level Calculation (Download & Use)Document2 pagesDrainage Invert Level Calculation (Download & Use)Waheed Ur RehmanNo ratings yet
- TSU 23.april 2021 Eye On H&S - AllOne Advisory ServiceDocument1 pageTSU 23.april 2021 Eye On H&S - AllOne Advisory ServiceWaheed Ur RehmanNo ratings yet
- LOTOInspection FormDocument1 pageLOTOInspection FormWaheed Ur RehmanNo ratings yet
- PPE Request FormDocument1 pagePPE Request FormWaheed Ur RehmanNo ratings yet