You might also like
- Nakamura 2017Document7 pagesNakamura 2017shobhana20No ratings yet
- An Optimization Method For EquDocument22 pagesAn Optimization Method For EquValentina Castaneda TorresNo ratings yet
- Accessibility and Site Suitability For Healthcare Services Using GIS Based Hybrid Decision-Making Approach A Study in Murshidabad, IndiaDocument18 pagesAccessibility and Site Suitability For Healthcare Services Using GIS Based Hybrid Decision-Making Approach A Study in Murshidabad, IndiaASHUTOSH OJHANo ratings yet
- The Canadian Geographer - 2019 - Shah - Geographic Accessibility To Primary Care Providers Comparing Rural and Urban AreasDocument14 pagesThe Canadian Geographer - 2019 - Shah - Geographic Accessibility To Primary Care Providers Comparing Rural and Urban Areasshobhana20No ratings yet
- ARTICLE In-DhakaDocument21 pagesARTICLE In-DhakaEdwin Rafael Patino CortesNo ratings yet
- ARM 421: Research Methods FOR Architecture: ResearchersDocument19 pagesARM 421: Research Methods FOR Architecture: ResearchersKristle MacapagaoNo ratings yet
- Urban and Regional PlanningDocument36 pagesUrban and Regional PlanningGilsonNo ratings yet
- Ijgi 11 00516Document13 pagesIjgi 11 00516Cherry KimNo ratings yet
- GWR and HealthDocument12 pagesGWR and HealthRimjhim BajpaiNo ratings yet
- Spatial Vertical Equity in PubDocument16 pagesSpatial Vertical Equity in PubValentina Castaneda TorresNo ratings yet
- Measuring Accessibility To Public Services and Infrastructure Criticality For Disasters Risk ManagemenDocument16 pagesMeasuring Accessibility To Public Services and Infrastructure Criticality For Disasters Risk ManagemencherrielNo ratings yet
- An Assessment of The Distribution of Health Care Facilities in Bogorolocal Government Area of Bauchi StateDocument10 pagesAn Assessment of The Distribution of Health Care Facilities in Bogorolocal Government Area of Bauchi StateEditor IJTSRDNo ratings yet
- UEE J: Hospital Site Selection Using Two-Stage Fuzzy Multi-Criteria Decision Making ProcessDocument12 pagesUEE J: Hospital Site Selection Using Two-Stage Fuzzy Multi-Criteria Decision Making ProcessAbinaya KalyanasundaramNo ratings yet
- 1 s2.0 S0143622822000157 MainDocument10 pages1 s2.0 S0143622822000157 Mainphyq1435034345No ratings yet
- 1 s2.0 S0143622814001787 MainDocument7 pages1 s2.0 S0143622814001787 MainSantiago Díaz RuizNo ratings yet
- Hospital Site Selection AnalysisDocument16 pagesHospital Site Selection AnalysisMarlo Anthony BurgosNo ratings yet
- Geostatistical Linkage of National Demographic and Health Survey Data: A Case Study of TanzaniaDocument14 pagesGeostatistical Linkage of National Demographic and Health Survey Data: A Case Study of Tanzaniaobaidur.slghnNo ratings yet
- Art 3A10.1186 2F1476 072X 13 36Document14 pagesArt 3A10.1186 2F1476 072X 13 36Y YNo ratings yet
- RRL 02Document2 pagesRRL 02Zet MiguelNo ratings yet
- Comparative Analysis of Public Transport Accessibility To Hospitals in Cordoba 20192023 Where Are We NowDocument22 pagesComparative Analysis of Public Transport Accessibility To Hospitals in Cordoba 20192023 Where Are We Nowmaezison83No ratings yet
- Distribution and Accessibility of Road Networks To Educational Facilities in Delta State: Transport Geographical AppraisalDocument19 pagesDistribution and Accessibility of Road Networks To Educational Facilities in Delta State: Transport Geographical AppraisalEditor IjrssNo ratings yet
- System Approaches To Water, Sanitation, and Hygiene A Systematic Literature ReviewDocument18 pagesSystem Approaches To Water, Sanitation, and Hygiene A Systematic Literature ReviewDicky Estosius TariganNo ratings yet
- Scaling Laws Between Population and Facility DensitiesDocument5 pagesScaling Laws Between Population and Facility DensitiesKiet HoangNo ratings yet
- Sensors 17 01104Document25 pagesSensors 17 01104sheikhali9180No ratings yet
- Assessing The Spatial AccessibDocument20 pagesAssessing The Spatial AccessibValentina Castaneda TorresNo ratings yet
- Ijerph 17 04528Document17 pagesIjerph 17 04528Abdul HadiNo ratings yet
- Water: A Perception Study of An Integrated Water System Project in A Water Scarce Community in The PhilippinesDocument23 pagesWater: A Perception Study of An Integrated Water System Project in A Water Scarce Community in The PhilippinesMada Pasalli SaludungNo ratings yet
- Sustainability 15 11985Document25 pagesSustainability 15 11985Shahriar RahmanNo ratings yet
- 5-323-Keterjangkauan Spasial PuskesmasDocument14 pages5-323-Keterjangkauan Spasial PuskesmasFIQIH NURMANSYAHNo ratings yet
- Geospatial Mapping and Analysis of The Distribution of Public Primary Healthcare Centers in Kaduna State, Nigeria.Document15 pagesGeospatial Mapping and Analysis of The Distribution of Public Primary Healthcare Centers in Kaduna State, Nigeria.Editor IJTSRDNo ratings yet
- Sustainability 11 05492 v2Document16 pagesSustainability 11 05492 v2Sheraz UllahNo ratings yet
- Green InfrasDocument6 pagesGreen InfrasbregasNo ratings yet
- Remotesensing 11 02801Document26 pagesRemotesensing 11 02801umisaaadahNo ratings yet
- Capturing Patients Needs in CaDocument18 pagesCapturing Patients Needs in CaAnissa ResianaNo ratings yet
- A Literature Review of The Use of GIS-Based Measures of Access To Health Care ServicesDocument21 pagesA Literature Review of The Use of GIS-Based Measures of Access To Health Care ServicesApocryphus ErasmusNo ratings yet
- Evaluación y Gestión de Servicios Recreativos de Espacios Verdes UrbanosDocument10 pagesEvaluación y Gestión de Servicios Recreativos de Espacios Verdes UrbanosKenneth Ayala CastroNo ratings yet
- Estimating Need, Demand and Supply in Primary Health Care Services: A Local Application in ArgentinaDocument9 pagesEstimating Need, Demand and Supply in Primary Health Care Services: A Local Application in ArgentinaprincesaleemNo ratings yet
- Tessa Ecosystem Services PDFDocument7 pagesTessa Ecosystem Services PDFinscNo ratings yet
- Sustainability 12 09839 v2Document12 pagesSustainability 12 09839 v2prajakta vaidyaNo ratings yet
- Urban Accessibility Index Literature ReviewDocument4 pagesUrban Accessibility Index Literature Reviewafdtvztyf100% (1)
- Icao Aerodrome Design Manual Part 1 RunwaysDocument15 pagesIcao Aerodrome Design Manual Part 1 RunwaysNafila El HafizahNo ratings yet
- Analysis of Care-Seeking Behaviour and Referral Mechanism Modelling in Public Healthcare FacilitiesDocument34 pagesAnalysis of Care-Seeking Behaviour and Referral Mechanism Modelling in Public Healthcare FacilitiesPratish DesignNo ratings yet
- Remotesensing 02 02274 v2 PDFDocument31 pagesRemotesensing 02 02274 v2 PDFBtph MoiNo ratings yet
- Civil EngineeringDocument72 pagesCivil EngineeringSri Rama ChandNo ratings yet
- Hendy2012 Article AnOrganisationalAnalysisOfTheIDocument10 pagesHendy2012 Article AnOrganisationalAnalysisOfTheIAlejandro CardonaNo ratings yet
- Research Paper Two-ColumnDocument22 pagesResearch Paper Two-ColumnJoseph TsoNo ratings yet
- Sustainability 12 03923 v2Document17 pagesSustainability 12 03923 v2Tuệ TuệNo ratings yet
- Literature Review On Peri Urban Natural Resource Conceptualisation and Management ApproachesDocument12 pagesLiterature Review On Peri Urban Natural Resource Conceptualisation and Management Approachesea813c29No ratings yet
- Commentary: The Applications of Implementation Science in Water, Sanitation, and Hygiene (WASH) Research and PracticeDocument10 pagesCommentary: The Applications of Implementation Science in Water, Sanitation, and Hygiene (WASH) Research and PracticeNisa AzrinNo ratings yet
- Land Use Change DissertationDocument5 pagesLand Use Change DissertationNeedHelpWithPaperSingapore100% (1)
- Impact of Urbanization On Ecosystem Health A CaseDocument17 pagesImpact of Urbanization On Ecosystem Health A CaseNouhaïla RejimNo ratings yet
- Telemedicine StudyDocument7 pagesTelemedicine Studyvijju006No ratings yet
- Capturing Spatial Analysis of Slums PDFDocument19 pagesCapturing Spatial Analysis of Slums PDFAbhishek DeshmukhNo ratings yet
- Jana+¡na Ferreira Guidolini-Publicacao-Internacional-Ijerph-15-02582Document15 pagesJana+¡na Ferreira Guidolini-Publicacao-Internacional-Ijerph-15-02582jackNo ratings yet
- 2022 - A Multi Objective Distributionally Robust Model For Sustainable Last MileDocument42 pages2022 - A Multi Objective Distributionally Robust Model For Sustainable Last MileleoNo ratings yet
- Jurnal KetigaDocument12 pagesJurnal KetigagalihNo ratings yet
- Human Health and Climate Change: Leverage Points For Adaptation in Urban EnvironmentsDocument25 pagesHuman Health and Climate Change: Leverage Points For Adaptation in Urban EnvironmentsfaithnicNo ratings yet
- Real-Time Transit, Rider'S Transit Perceptions and Travel BehaviorsDocument20 pagesReal-Time Transit, Rider'S Transit Perceptions and Travel Behaviorsapi-529360970No ratings yet
- Sewerage Infrastructure Asset Management Based On A Consumer Centric ApproachDocument13 pagesSewerage Infrastructure Asset Management Based On A Consumer Centric ApproachRamdinNo ratings yet
- New sanitation techniques in the development cooperation: An economical reflectionFrom EverandNew sanitation techniques in the development cooperation: An economical reflectionNo ratings yet
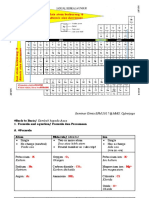
- Seminar Kimia SPM Mmu 2017 CG Adura Jawapan Kertas 2 PDFDocument48 pagesSeminar Kimia SPM Mmu 2017 CG Adura Jawapan Kertas 2 PDFNoorleha Mohd YusoffNo ratings yet
- Causes of Status EpilepticusDocument12 pagesCauses of Status EpilepticusSergio MouraNo ratings yet
- Food Science and Technology Research Volume 8 Issue 1 2002 (Doi 10.3136/fstr.8.80) ANDO, Hitomi CHEN, Yi-Chun TANG, Hanjun SHIMIZU, MayumiDocument5 pagesFood Science and Technology Research Volume 8 Issue 1 2002 (Doi 10.3136/fstr.8.80) ANDO, Hitomi CHEN, Yi-Chun TANG, Hanjun SHIMIZU, Mayumiyamid pismagNo ratings yet
- Malaria and Climate Change1248scribdDocument3 pagesMalaria and Climate Change1248scribdGuadalupe JamesNo ratings yet
- On Agents of MutationDocument22 pagesOn Agents of Mutationmine_ne361No ratings yet
- API STD 2510Document27 pagesAPI STD 2510Rafnun100% (1)
- Carrot Cake Cupcakes - Sugar Spun RunDocument2 pagesCarrot Cake Cupcakes - Sugar Spun RunSean BermejoNo ratings yet
- The Challenges of Achieving Equity Within Public School Gifted and Talented ProgramsDocument13 pagesThe Challenges of Achieving Equity Within Public School Gifted and Talented Programsapi-623888875No ratings yet
- 2020 Guidelines WebDocument249 pages2020 Guidelines WebDaryl Barrios LamedaNo ratings yet
- BC-8000 Ops ManualDocument21 pagesBC-8000 Ops ManualNIXON BENITEZNo ratings yet
- Transportation - Life Processes Class 10 Notes: Transportation in Human Beings: The Circulatory System Is Responsible ForDocument4 pagesTransportation - Life Processes Class 10 Notes: Transportation in Human Beings: The Circulatory System Is Responsible ForGeetanjali jadhavNo ratings yet
- ISSF The Ferritic Solution EnglishDocument68 pagesISSF The Ferritic Solution EnglishdhurushaNo ratings yet
- Preparation of Standard Solutions and Acid-Base TitrationDocument4 pagesPreparation of Standard Solutions and Acid-Base TitrationJhon Jasper ApanNo ratings yet
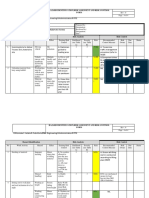
- Roof Work HIRARCDocument4 pagesRoof Work HIRARCSarah Liyana86% (7)
- n thi tuyển sinh lớp 10 môn tiếng AnhDocument29 pagesn thi tuyển sinh lớp 10 môn tiếng AnhnguyenanhmaiNo ratings yet
- Sweet Poison - David Gillespie PDFDocument214 pagesSweet Poison - David Gillespie PDFvalterbrigo100% (10)
- THERMOFLUX PEELING 25 KWDocument48 pagesTHERMOFLUX PEELING 25 KWsorin.agapeNo ratings yet
- SONY CASE - Strategic ManagementDocument7 pagesSONY CASE - Strategic ManagementMirza Trilaksono0% (1)
- Laporan Case Mix Gabungantgl 27-12-2023Document191 pagesLaporan Case Mix Gabungantgl 27-12-2023Adhita Septianty ningrumNo ratings yet
- 2009 Annual Flood Report of FFCDocument44 pages2009 Annual Flood Report of FFCshadi khanNo ratings yet
- RM AOSASw GBHWK7 RW 7 MP 99 QDocument38 pagesRM AOSASw GBHWK7 RW 7 MP 99 QfernanroldanNo ratings yet
- Operational Procedure On Illegal Drugs and Vice ControlDocument18 pagesOperational Procedure On Illegal Drugs and Vice ControlJohn Lester PanaliganNo ratings yet
- Completion Equipment ChecklistDocument3 pagesCompletion Equipment ChecklistYougchu LuanNo ratings yet
- Natural Gas Filters PDFDocument10 pagesNatural Gas Filters PDFKirthiga RamaswamyNo ratings yet
- Over View: of Panchayati Raj DepartmentDocument48 pagesOver View: of Panchayati Raj DepartmentGomathiRachakondaNo ratings yet
- DLL Mapeh-4 Q1 W3Document8 pagesDLL Mapeh-4 Q1 W3dianne grace incognitoNo ratings yet
- Fluorometric Determination of ChlorophyllDocument13 pagesFluorometric Determination of Chlorophyllstar warsNo ratings yet
- Nutrition Practice Test QuestionsDocument8 pagesNutrition Practice Test QuestionsDianna Marrie M. NayreNo ratings yet
- Ảnh hưởng của hệ thống sưởi Ohmic đến sự phân hủy của các thành phần hoạt tính sinh học trong thực phẩm 2020 PDFDocument18 pagesẢnh hưởng của hệ thống sưởi Ohmic đến sự phân hủy của các thành phần hoạt tính sinh học trong thực phẩm 2020 PDFĐoanNo ratings yet
- Biyani's Think Tank: Cell Biology & GeneticsDocument81 pagesBiyani's Think Tank: Cell Biology & GeneticsAkshay chandrakarNo ratings yet