Professional Documents
Culture Documents
JoWC - 2022 - 31 - 11 - 000 - Da Fonseca Cerqueira 221020 BC
JoWC - 2022 - 31 - 11 - 000 - Da Fonseca Cerqueira 221020 BC
Uploaded by
HelenaOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
JoWC - 2022 - 31 - 11 - 000 - Da Fonseca Cerqueira 221020 BC
JoWC - 2022 - 31 - 11 - 000 - Da Fonseca Cerqueira 221020 BC
Uploaded by
HelenaCopyright:
Available Formats
practice
Complications related to diabetic foot
ulcer and associated social vulnerability
factors at a referral centre in Brazil
Objective: To analyse the prevalence and associated social diabetic foot (PR: 0.79 (0.67–0.92)) and the use of public transport to
vulnerability factors of complications related to diabetic foot ulcer access CEDEBA (PR: 0.82 (0.71–0.96)). On the other hand,
(DFU) among individuals followed up in a public care centre in Brazil. amputations were positively associated with male sex (PR: 1.61
Method: This is a cross-sectional study carried out with individuals (1.23–2.11)) and not working (PR: 3.83 (1.48–9.95)) and negatively
followed up at the diabetic foot service of the State Referral Center associated with age >60 years (PR: 0.57 (0.45–0.74)) and the use of
for Diabetes and Endocrinology Assistance (CEDEBA) between public transport to access CEDEBA (PR: 0.63 (0.49–0.81)).
December 2019 and October 2020, during the COVID-19 pandemic. Conclusion: The prevalence of complications was higher than in
Descriptive analysis and comparison of the prevalence of previous studies, and associated with sociodemographic and clinical
complications related to DFU were carried out. The factors characteristics. Further research should be encouraged to investigate
associated with the outcome variables were verified by hierarchical the role that determinants of health play in the course of the disease,
logistic regression analysis. contributing to the construction of strategies that incorporate
Results: Among the 253 participants in this study, 30.4% had an formulations developed in the social and economic spheres to
active ulcer, 57.1% had a previous ulcer and 45.1% had an broaden the impact of health actions on the prevention of major
Journal of
amputation. Lower limb ulcers were positively associated with male diabetic foot complications.
sex (prevalence ratio (PR): 1.22 (1.04–1.43)) and negatively Declaration of interest: The authors have no conflicts of interest
associated with age >60 years (PR: 0.71 (0.61–0.83)), screening for to declare.
diabetes ● diabetic foot ● epidemiology ● prevention and control ● public health ● ulcer ● vulnerability ● wound ●
wound care ● wound dressing ● wound healing
Wound Care
D
iabetic foot (DF) is a life-threatening, deep tissues associated with neurological abnormalities
chronic complication of diabetes. The and varying degrees of peripheral vascular disease in the
incidence has been increasing due to an lower limb.4
increase in worldwide diabetes prevalence The condition includes changes of different origins,
and prolongation of life expectancy of the common outcome of which is the appearance of
people living with the disease.1,2 The increase in general diabetic foot ulcers (DFU). DFU can favour the invasion
life expectancy increases the likelihood of developing of bacteria due to the loss of skin integrity, facilitating
chronic diseases such as diabetes. The increase in life the development of infections, which are a precipitating
expectancy of people living with diabetes increases the factor for 60–90% of amputations.5–7
probability of developing chronic complications of the The treatment of DFU is challenging due to its
disease. It is caused by lesions in the deep tissues multifactorial aetiology. The risk of recurrence of an
associated with neurological disorders and peripheral ulcer is high even when it is healed, being estimated at
vascular disease in the lower limbs that can generate a 30–40% in the first five years,8 and the associated
spectrum of manifestation, such as foot insensitivity, mortality can reach up to 45% in five years.9 Thus, it is
claudication, deformities and Charcot foot. According understood that the prevention of DFU should be the
to the International Work Group on the Diabetic Foot mainstay of care programmes aimed at reducing
(IWGDF),3 it is a clinical syndrome characterised by the amputation rates among people living with diabetes.10
existence of infection, ulceration and/or destruction of Although efforts to build knowledge about DF have
resulted in the elaboration and wide dissemination of
prevention and treatment protocols, data have shown
Monique Magnavita Borba da Fonseca Cerqueira,1 Master in Public Health*; that the number of amputations continues to increase.10
Helena Maria Silveira Fraga Maia,1 Doctor in Public Health; Magno Conceição das
Mercês,1 Doctor in Health Sciences; Marcio Santos da Natividade,2 Doctor in Public
This may be related to the fact that epidemiology has
Health; Onsli dos Santos Almeida,1 Nurse; Eduardo Fernandes Santana,1 Master in focused on the risk measurement of factors associated
© 2022 MA Healthcare Ltd
Public Health; Beatriz Andrade Mafra Oliveira,1 Medical Student; Marcelo Araújo,3 with individual lifestyle and exposure in an attempt to
Doctor in Medicine explain the aetiology of DF, with little consideration of
*Corresponding author email: mmcerqueira@uneb.br
environmental, behavioural and programmatic
1 Department of Life Sciences, State University of Bahia, Brazil. 2 Collective Health
Institute, Federal University of Bahia, Brazil. 3 Health Department, Santa Cruz State influences on the disease.11,12
University, Brazil. The distribution of risk factors for non-communicable
2 JOURNAL OF WOUND CARE VOL 31, NO 11, NOVEMBER 2022
practice
diseases (NCDs) is socially determined and, although Method
the causal relationship between an individual’s This was a cross-sectional study with individuals
socioeconomic position and diabetes is not yet fully followed up at the DF service of the State Referral Center
understood, the origin of the disease lies in complex for Diabetes and Endocrinology Assistance (CEDEBA),
processes that interact with each other, involving the specialised in multidisciplinary care for people with
lack of access to information about healthy foods, diabetes, including endocrinologists, vascular surgeons,
physical activity, health services, and occupational and physiotherapists, nurses, psychologists and social
economic opportunities.11,13 As reported in India, it has workers. All patients were referred from primary
been observed that DFU is usually a consequence of the healthcare (PHC) and fulfilled the following criteria for
association between inadequate hygiene, use of follow-up:
inappropriate shoes and delay in accessing health ● Diagnosed with diabetes
services.14 ● Showing neuropathic or arterial changes secondary to
In Brazil, there are no records of studies addressing the disease
the association between prevalence and contexts that ● With or without presence of current or past ulcer,
produce vulnerability for the development of DFU and osteoarticular deformities and/or DF-related
amputations. In the northeast region of the country, for amputations.
instance, where social determinants of health play an People diagnosed with type 2 diabetes, >18 years of
important role in the pathophysiology of the disease, age, with or without injuries and/or amputations in the
this suggests a gap in the knowledge about susceptibility lower limbs related to diabetes, living in Salvador,
to this condition. Therefore, this study aims to analyse Bahia, Brazil, and who consented to sign the Free and
the prevalence and associated factors of complications Informed Consent Form (FICF) were consecutively
related to DFU, among individuals followed up in a included in the study. People with cognitive and/or
Journal of
secondary care centre, in the public services of the state language deficits that precluded the interviews, or living
of Bahia, located in northeast of Brazil, in order to outside the state capital, where CEDEBA is located, were
contribute to the debate on the subject. excluded from the study. (The addresses of people living
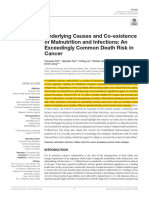
Fig 1. Hierarchical logistic regression model of factors associated with complications related to diabetic foot (DF)
Wound Care
Level 1 Level 2 Level 3 Level 4
Sociodemographic Environmental Clinical Communication Diabetic foot
characteristics characteristics characteristics processes injuries
- Age - Piped water - Diabetes duration - Understands
- Sex - Sanitary/sewage - Therapeutic everything in
- Skin colour/ - Rubbish collection adherence the service
ethnicity - Transport - Consultation at - Understands
- Marital status primary healthcare the terms
- Inhabitants - Health education - Asks when
and home to prevent in doubt
- Schooling diabetic foot - Has already left
- Screening of with doubts about
- Occupation
diabetic foot your disease
- Income
- Has already left
- Religion with doubts about
medications
- Feels well cared for
- Thinks the doctor
has made mistakes
- Feels responsible
for treatment
- Stopped seeking
help for fear
- Stopped seeking
help for not
knowing how to
say what was felt
© 2022 MA Healthcare Ltd
- The doctor
explained diabetes
complications
JOURNAL OF WOUND CARE VOL 31, NO 11, NOVEMBER 2022 3
practice
elsewhere were georeferenced with the intention of according to the four-item Morisky–Green scale,
identifying the distance people walked to the service, namely:
and this variable was part of another study). 1. Do you sometimes have problems remembering to
Primary data were collected with investigation forms take your medication?
and clinical evaluation of the feet, and secondary data 2. Do you sometimes forget to take your medication?
were collected through a search of the patients’ medical 3. When you are feeling better, do you stop taking the
records. Initially, data collection took place from medication?
December 2019 to March 2020 by the main author, 4. Sometimes, if you feel worse when taking the
using a structured questionnaire. Face-to-face interviews medication, do you stop taking it?
and care activities carried out by CEDEBA were The individuals were classified as non-adherent if
suspended from April 2020 due to the COVID-19 they answered positively to any of the questions. The
pandemic. Given this context and considering the access to medical consultations at PHC in the last year
existence of secondary data recorded in medical records was judged by the number of times a year, being
by the main investigator, who is the doctor responsible stratified as: not attending or rarely attending; once or
for the clinic where the research population was twice; and three or more times. The last two categories
selected, the interviews were resumed from August 2020 were condensed as regulars and the first defined non-
through telephone contact with individuals who had a regulars for the analysis. Finally, the access to DF
previous appointment for face-to-face consultation and prevention activities at PHC in the last year was
who accepted this type of interview, without prejudice investigated by asking whether there was participation
to the quality of the investigation. The physical of individuals in health education activities and
examination data were collected through the medical screening by examining the feet.
records of the last performed consultation. The following variables were used with regard to
Journal of
Sociodemographic variables consisted of age and sex, adequate health communication: the patient
with age being categorised as <60 years or ≥60 years, the understands what is said in the service; understands the
age which defines people of older age according to the terms used by health professionals; asks when in doubt;
Brazilian Institute of Geography and Statistics.15 Skin has already left with doubts about the health situation;
colour was self-declared and classified according to the has already left with doubts about how to use the
Brazilian Institute of Geography and Statistics (IBGE), medications; feels well cared for by health professionals;
but it was classified into white and non-white for feels responsible for the treatment to be performed;
Wound Care
analysis purposes. Marital status was defined according reported that some medical professional has made
to the existence or absence of partners. The number of mistakes; stopped seeking help from a health professional
residents in the household was categorised between because they do not know how to say what they have
living alone or not living alone. Schooling was defined felt; stopped seeking help from a health professional
according to the number of years of study, categorised because they were afraid of what they felt; and reported
as <8 years and ≥8 years. Occupational activity was that some medical professional has already explained in
classified into salaried work, retirement, unable to work detail the bad consequences of untreated diabetes. All
and without receiving benefits due to illness, or out of these variables were categorised as ‘yes’ or ‘no’.
the workforce, as defined by the IBGE. The categories The dependent variables or outcomes—current ulcer
working and not working were considered for the and/or history of previous ulcer and amputation—were
analysis. Individual income was categorised as ≤1 or >1 determined by the clinical evaluation of the feet and/or
times minimum wage (R$1045.00). Religion was searching the medical records.
determined according to how the faith was processed The collected data were tabulated in Microsoft Excel
by the individual, and categorised between those who for Windows (Microsoft Corp., US) and analyses were
followed a religion and those who did not. The conducted in the statistical package Stata 15 (supplied
questions about access to public services investigated by the Public Health Laboratory of the University of the
the existence of piped water, sanitary sewage and State of Bahia, Brazil), where corrections and
rubbish collection at home, in addition to the use of inconsistencies were eliminated. The descriptive
means of transport to access CEDEBA. All variables analysis identified the general and specific characteristics
related to sanitation were categorised as present or of the studied population, and allowed the comparison
absent, and the transport was classified as public, which of the prevalence of related complications of DF
included the use of buses or the Metro, and private, according to the characteristics found in the
including own or family car, taxi and rides using investigations. Bivariate analyses were performed to
transportation applications. identify the set of variables most associated with the
The clinical data consisted of recording the diabetes outcomes considering the value of Pearson’s Chi‑squared
© 2022 MA Healthcare Ltd
treatment time in years, which was categorised as test (χ2) or Fisher’s exact test. The magnitude of the
≤10 years or >10 years. This cutoff point was defined association under investigation was estimated by
because, according to Riaz et al.,16 most of the patients calculating the prevalence ratios (PR), adopting the 95%
with a DFU had diabetes for >10 years with poor confidence interval (CI). A multivariate analysis was
glycaemic control. Therapeutic adherence was classified performed according to the hierarchical model defined
4 JOURNAL OF WOUND CARE VOL 31, NO 11, NOVEMBER 2022
practice
a priori (Fig 1), using the value of p≤0.20 and the communication. Most of the interviewees (71.2%)
theoretical consistency of association with the outcomes already had some complication related to DF at the time
as screening criteria for inclusion of the independent of the research and, among them, 30.4% had an active
variable. All socioeconomic variables were included in ulcer, 57.1% had had a previous ulcer, and 45.1% had
the first block (level 1), even those not significant in the undergone an amputation. Among amputees, 72.8%
bivariate analysis. The significant variables in this had undergone a minor amputation, defined as those
analysis were conserved in the model and entered into below the ankle, and 27.2% a major amputation,
the adjustment of the next block, that is, the defined as those above the ankle. A higher proportion
environmental variables (level 2), which were of people with DFU was observed among individuals
introduced into the model simultaneously, regardless of with up to 10 years of illness (80.0%) than those with a
changes in the value of the statistical significance of the longer time of diabetes diagnosis (65.0%; p=0.021).
level 1 variables that were already in the model. The Regarding variables related to access to DF prevention
same procedure was used for the following blocks (levels activities in PHC in the last year, a higher prevalence of
3 and 4), i.e., clinical and communication variables, DFUs and amputations was observed among individuals
respectively. The variables associated with the outcome who participated in the screening at PHC in the last
with a level of p≤0.17 were maintained in the partial year (86.3% and 58.8%, respectively) than individuals
hierarchical models, but only those that showed a who did not have their feet examined (69.4% and
significant association with the outcome, with a value 41.6%, respectively; p=0.003 and 0.027, respectively).
of p≤0.05, remained in the final model. The variable communication showed a higher
proportion of patients with DFU among users who said
Ethical approval they had already left a consultation with doubts about
The research project was approved by Committee on their health situation (79.4%) than those who denied it
Journal of
Publication Ethics at Plataforma Brasil under CAAE nº (65.8%; p=0.043) and among those who said they had
23209119.7.0000.0057. All patients invited to stopped seeking help due to fear of what they were
participate in the study signed the FICF. feeling (84.4%) compared with those who opposed this
behaviour (67.0%; p=0.046). A higher proportion of
Results amputations was also identified among individuals who
Of the 285 individuals approached, 259 signed the FICF believed that a doctor had made a mistake with them
(15 refused to participate in the research, seven were (55.4%) than those who do not believe in this possibility
Wound Care
excluded for living in another city and four were (40.8%; p=0.033).
excluded for being patients with type 1 diabetes). Tables 3 and 4 show the bivariate and multiple
Among the questionnaires, six were excluded by analyses of the four variable levels regarding the
duplicate collection. Thus, 253 individuals living with associations between complications of DF, and
diabetes took part in this study. Sociodemographic and sociodemographic and clinical characteristics, as well as
environmental characteristics are described in Table 1. those related to access to public services and DF
Statistically significant differences in the proportion prevention activities at PHC and communication of the
of DFUs and amputations were observed between the studied population. The multiple regression model
age groups, with the youngest individuals presenting adjusted for the characteristics included in level 1
with a higher prevalence (85.9% and 58.7%, revealed that the variables age and sex remained
respectively) when compared with older individuals associated with DFU (prevalence ratio (PR): 0.69, 95% CI:
(59.6% and 37.3%, respectively; p<0.001 and p=0.001, 0.60–0.81; PR: 1.29, 95% CI: 1.09–1.52, respectively)
respectively). Regarding sex, men had a higher while following a religion lost its strength of association
occurrence of DFU (78.3%) and amputations (56.7%) with DFU after the adjustment (PR: 1.20, 95% CI: 0.95–
than women (60.9 and 34.6%, respectively; p=0.003 1.51). With regard to amputation, age, sex and
and p<0.0019, respectively). A higher proportion of occupation maintained the strength of association after
people with DFUs was also found among individuals the adjustment (PR: 0.63, 95% CI: 0.49–0.83; PR: 1.64,
without religion (88.0%) compared with those who had 95% CI: 1.24–2.17; PR: 3.32, 95% CI: 1.30–8.44,
religion (67.4%; p=0.034). Regarding the means of respectively). No variable was associated with the
transport used to access CEDEBA, users of private outcomes at level 2. The block of variables at level 3
transport had a higher prevalence of DFUs and showed an association between DFU and diabetes
amputations (75.9% and 53.7%, respectively) than duration (PR: 0.81, 95% CI: 0.69–0.95). Screening for DF
users of public transport (64.1% and 38.6%, respectively; (PR: 0.75, 95% CI: 0.65–0.87; PR: 0.71, 95% CI: 0.53–
p=0.045 and p=0.017, respectively). No differences in 0.94, respectively) is associated with both outcomes after
proportion were observed between DFUs and multiple regression. On the other hand, ‘access to health
© 2022 MA Healthcare Ltd
amputations, and other sociodemographic variables or education practices’ lost strength of association with
related to access to public services. DFU after adjustment (PR: 1.09, 95% CI 0.85–1.40). The
Table 2 shows data on the prevalence of injuries block of variables at level 4 showed an association
related to DF according to clinical characteristics relative between DFU and the variables ‘leaving with doubts
to diabetes care activities, prevention of DF and about the health situation’ and ‘not seeking help for fear
JOURNAL OF WOUND CARE VOL 31, NO 11, NOVEMBER 2022 5
practice
Table 1. Sociodemographic characteristics and those related to access to public services of individuals
living with type 2 diabetes followed up at the CEDEBA diabetic foot clinic, Salvador, Bahia, Brazil,
2019–2020 (n=253)
Variable n (%) Prevalence of p-value Prevalence of p-value
DFU, n (%) amputation, n (%)
Sociodemographic
Age, years
<60 92 (36.4) 79 (85.9) 54 (58.7)
≥60 161 (63.6) 96 (59.6) <0.001 60 (37.3) 0.001
Sex
Female 133 (52.6) 81 (60.9) 46 (34.6)
Male 120 (47.4) 94 (78.3) 0.003 68 (56.7) <0.001
Skin colour/ethnicity*
White 19 (7.5) 12 (63.2) 9 (47.4)
Non-white 233 (92.5) 163 (69.9) 0.536 105 (45.1) 0.846
Marital status*
With partner 131 (52.0) 90 (68.7) 62 (47.3)
Journal of
Without partner 121 (48.0) 85 (70.2) 0.790 52 (43.0) 0.488
Lives alone*
No 216 (85.7) 149 (69.0) 97 (44.9)
Yes 36 (14.3) 26 (72.2) 0.696 17 (47.2) 0.796
Schooling*, years
Wound Care
<8 127 (50.4) 87 (68.5) 0.744 51 (40.2) 0.102
≥8 125 (49.6) 88 (70.4) 63 (50.4)
Occupation*
Salaried 18 (7.1) 12 (66.7) 4 (22.2)
No work due to illness 32 (12.7) 29 (90.6) 0.087† 22 (68.8) 0.001
Retired 169 (67.1) 117 (69.2) 0.823 79 (46.7) 0.046
Out of the workforce 33 (13.1) 17 (51.5) 0.298 9 (27.3) 0.966†
Income (compared to minimum wage)*
≤1× 148 (58.7) 107 (72.3) 0.241 64 (43.2) 0.448
>1× 104 (41.3) 68 (65.4) 50 (48.1)
Religion
Catholic/Protestant/other 227 (90.1) 153 (67.4) 101 (44.5)
No religion 25 (9.9) 22 (88.0) 0.034 13 (52.0) 0.474
Access to public services
Piped water*
Yes 247 (98.0) 171 (69.2) 113 (45.7)
No 5 (2.0) 4 (80.0) >0.999† 1 (20.0) 0.501†
© 2022 MA Healthcare Ltd
Sanitary sewage*
Yes 236 (93.6) 165 (69.9) 107 (45.3)
No 16 (6.4) 10 (62.5) 0.712† 7 (43.7) 0.902
6 JOURNAL OF WOUND CARE VOL 31, NO 11, NOVEMBER 2022
practice
Table 1. Sociodemographic characteristics and those related to access to public services of individuals
living with type 2 diabetes followed up at the CEDEBA diabetic foot clinic, Salvador, Bahia, Brazil,
2019–2020 (n=253) (continued)
Variable n (%) Prevalence of p-value Prevalence of p-value
DFU, n (%) amputation, n (%)
Access to public services (continued)
Garbage collection*
Yes 108 (42.9) 72 (66.7) 46 (42.6)
No 144 (57.1) 103 (71.5) 0.407 68 (47.2) 0.465
Means of transport (to access CEDEBA)
Private 108 (42.7) 82 (75.9) 58 (53.7)
Public 145 (57.3) 93 (64.1) 0.045 56 (38.6) 0.017
DFU—diabetic foot ulcer; *252 observations; †Fisher’s exact test
of asking’ (PR: 1.21, 95% CI: 1.03–1.42; PR: 1.26, 95% CI: around 6%, with the main risk factors being older age,
1.06–1.50, respectively). Moreover, thinking that a longer diabetes duration, hypertension, diabetic
doctor was wrong was associated with the outcome of retinopathy, smoking, chronic kidney disease and
Journal of
amputation (PR: 1.36, 95% CI: 1.04–1.78). The variable peripheral arterial disease.2,18 Although Zhang et al.1
‘leaving with doubts about the health situation’ lost corroborate the information that older individuals are
strength of association with DFU after regression. more likely to develop a DFU, a negative association was
Table 5 shows the final hierarchical multivariate identified in the present study between being >60 years
logistic regression model. The variables considered old and developing complications related to DF. It
associated with the occurrence of DFU, adjusted for shows a trend of higher involvement of complications
diabetes duration and therapeutic adherence (and that generate functional limitation in a young and
Wound Care
although not statistically significant in our study, economically active population. In this sense, Coffey et
having a strong association with the outcome according al.19 suggest that most individuals with a DFU do not
to the literature), showed higher exposure among men have information or have limited knowledge about the
(PR: 1.22; 95% CI: 1.04–1.43) and lower exposure mechanisms by which diabetes acts in the
among individuals aged 60 years or over (PR: 0.71; pathophysiology of injuries. Even among those who
95% CI: 0.61–0.83), those who have access to public have an adequate level of knowledge, there are barriers
transport to CEDEBA (PR: 0.82; 95% CI: 0.71–0.96) and to the implementation of a self-care routine related to
those who underwent screening tests (PR: 0.79; 95% CI: the difficulties of a busy daily life, especially among the
0.67–0.92). The variables considered associated with youngest patients, which impacts on the adherence to
amputation outcome, adjusted for diabetes duration prevention and treatment practices. It is important to
and therapeutic adherence, showed higher exposure highlight that foot self-care was particularly impactful
among men (PR: 1.61; 95% CI: 1.23–2.11) and not during the COVID-19 pandemic, when access to health
working (PR: 3.83; 95% CI: 1.48–9.95) and lower infrastructure may have been limited.20,21
exposure among individuals aged 60 years and over (PR: Santos et al.22 observed the occurrence of a high
0.56; 95% CI: 0.44–0.73) and who have access to public number of amputation surgeries in young people living
transport for CEDEBA (PR: 0.65; 95% CI: 0.50–0.83). with diabetes, estimating that, in addition to potential
years of life lost, amputation in this population
Discussion determined years lived with disability. It suggests that
In the present study, a high prevalence of complications the limitations imposed by the ageing process will be
related to DF was found among the interviewees. Parisi added to an irreversible physical disability, which
et al.17 worked with 1055 participants selected in generates a high disease burden. Moreover, Hanashiro
Brazilian diabetes treatment centres and observed a et al.23 demonstrated that people with amputation are
prevalence of 18.6% of active ulcer, 25.3% of history of impacted from a socioeconomic perspective after the
previous ulcer and 13.7% of amputation, which are occurrence of the disability due to being unable to work
values much lower than those found in this study. This and falling income, requiring social security and
© 2022 MA Healthcare Ltd
high prevalence may be related to the fact that the assistance protection, as return-to-work activities are
participants were selected at a referral centre to which infrequent, despite rehabilitation.
cases with advanced neuropathic and circulatory According to Silva et al.,24 Brazil has a shortage of
changes are referred, requiring a specialised evaluation. specific measures aimed at preventing and controlling
Globally, it is estimated that the prevalence of DFU is diabetes and, more specifically, DF, suggesting that PHC
JOURNAL OF WOUND CARE VOL 31, NO 11, NOVEMBER 2022 7
practice
Table 2. Clinical characteristics related to access to public services and diabetic foot (DF) prevention
activities at primary healthcare (PHC) and communication with individuals living with type 2 diabetes
followed up at the CEDEBA diabetic foot clinic, Salvador, Bahia, Brazil 2019–2020 (n=253)
Variable n (%) Prevalence of p-value Prevalence of p-value
DFU, n (%) amputation, n (%)
Clinic
Diabetes duration (in years)*
≤10 70 (27.7) 56 (80.0) 36 (51.4)
>10 183 (72.3) 119 (65.0) 0.021 78 (42.6) 0.208
Therapeutic adherence by the Morisky–Green test
Yes 86 (34.0) 56 (65.1) 41 (47.7)
No 167 (66.0) 119 (71.3) 0.316 73 (43.7) 0.549
Access to primary health care (PHC) in number of times a year
Rarely or not attending 150 (59.3) 102 (68.0) 0.627 65 (43.3) 0.505
≥1 103 (40.7) 73 (70.9) 49 (45.6)
Access to diabetic foot prevention activities at PHC in the last year
Journal of
Health education
Yes 75 (29.6) 57 (76.0) 36 (48.0)
No 178 (70.4) 118 (66.3) 0.127 78 (43.8) 0.542
Screening
Yes 51 (20.2) 44 (86.3) 30 (58.8)
Wound Care
No 202 (79.8) 131 (64.9) 0.003 84 (41.6) 0.027
Adequate health communication
Understands everything in the service
Yes 202 (79.8) 142 (70.3) 96 (47.5)
No 51 (20.2) 33 (64.7) 0.439 18 (35.3) 0.117
Understands the terms
Yes 160 (63.2) 108 (67.5) 70 (43.7)
No 93 (36.8) 67 (72.0) 0.451 44 (47.3) 0.583
Asks when in doubt
Yes 215(85.0) 145 (67.4) 94 (43.7)
No 38 (15.0) 30 (78.9) 0.157 20 (52.6) 0.309
Has already left with doubts about your disease
No 190 (75.1) 125 (65.8) 84 (44.2)
Yes 63 (24.9) 50 (79.4) 0.043 30 (47.6) 0.637
Has already left with doubts about medications
No 203 (80.2) 139 (68.5) 88 (43.3)
Yes 50 (19.8) 36 (72.0) 0.628 26 (52.0) 0.271
© 2022 MA Healthcare Ltd
Feels well cared for by health professionals
Yes 200 (79.1) 134 (67.0) 85 (42.5)
No 53 (20.9) 41 (77.4) 0.146 29 (54.7) 0.112
8 JOURNAL OF WOUND CARE VOL 31, NO 11, NOVEMBER 2022
practice
Table 2. Clinical characteristics related to access to public services and diabetic foot (DF) prevention
activities at primary healthcare (PHC) and communication with individuals living with type 2 diabetes
followed up at the CEDEBA diabetic foot clinic, Salvador, Bahia, Brazil 2019–2020 (n=253) (continued)
Variable n (%) Prevalence of p-value Prevalence of p-value
DFU, n (%) amputation, n (%)
Adequate health communication (continued)
Thinks that the doctor has made mistakes
No 179 (70.7) 118 (65.9) 73 (40.8)
Yes 74 (29.3) 57 (77.03) 0.082 41 (55.4) 0.033
Feels responsible for the treatment
Yes 235 (92.9) 162 (68.9) 104 (44.3)
No 18 (7.1) 13 (72.2) 0.771 10 (55.6) 0.353
Stopped seeking help for fear
No 221 (87.3) 148 (67.0) 97 (43.9)
Yes 32 (12.7) 27 (84.4) 0.046 17 (53.1) 0.326
Stopped seeking help for not knowing how to say what has felt
Journal of
No 225 (88.9) 154 (68.4) 98 (43.6)
Yes 28 (11.1) 21 (75.0) 0.479 16 (57.1) 0.173
The doctor explained about diabetes complicationsn
Yes 224 (88.9) 154 (68.8) 102 (45.5)
No 28 (11.1) 20 (71.4) 0.772 12 (42.9) 0.788
Wound Care
DFU—diabetic foot ulcer; *252 observations
should be the setting for these actions, with the lack of primary prevention practices. There is no doubt
implementation of strategies based on the best scientific that DFU and DF-related amputations are conditions
evidence. Considering that screening, stratification and which can be treated in PHC, given that the main
regular clinical follow-up of people at risk have been protocols for disease management place the population
measures with a stronger level of evidence in the screening of individuals together with education
prevention and control of complications related to DF, programmes for self-care and strict metabolic control as
it is indisputable that health surveillance actions priority recommendations.5,6
implemented at the most basic healthcare level have Regarding sex, being a man was strongly associated
the potential to control the epidemiological situation, with the development of ulcers and amputations. This
and may directly impact the human, social and financial information is in line with most studies previously
costs of the disease. published worldwide and can be explained by several
The large percentage of people who do not use PHC social and behavioural factors.27 It is assumed that male
as a gateway to the health system was notable in this individuals have a higher level of activity, and are often
study, although no statistically significant associations home providers, which imposes a higher burden on the
were found. From the user’s perspective, part of this feet. This fact, associated with a lower trend for
behaviour can be explained by the perception of therapeutic adherence, contributes to the increased
excessive bureaucratisation of actions in primary care, chance of developing foot injuries.17 A study conducted
which makes them seek, as a priority, solutions to their with 1515 people living with diabetes in the south of
health problems in the emergency units or at the Brazil showed that the prevalence of self-care deficit
secondary level.25 However, it is possible that, under the with the feet was significantly higher among men, as
influence of the medical hegemonic model, users have well as a less healthy behaviour in relation to diet.28 It
a culture of seeking specialised services and procedures.26 can be partially explained by the idea that men are
© 2022 MA Healthcare Ltd
Additionally, there was a low level of access of the socialised to be strong and independent, making the act
interviewed individuals to health education and of seeking care something that threatens their virility.29
screening actions aimed at DF prevention, and those The fact is that, regardless of the origin of these
who had access to these activities already had behaviours, it is necessary to reposition prevention
complications such as DFU or amputation, showing the strategies and health promotion, as well as forms of
JOURNAL OF WOUND CARE VOL 31, NO 11, NOVEMBER 2022 9
practice
Table 3. Association between diabetic foot ulcer (DFU) and amputation, and sociodemographic and clinical
characteristics, as well as those related to access to public services and diabetic foot (DF) prevention activities at
primary healthcare (PHC) and communication of individuals living with type 2 diabetes followed up at the CEDEBA
diabetic foot clinic, Salvador, Bahia, Brazil 2019–2020 (n=253)
DFU Amputation
Variable Crude PR Adjusted PR* p-value Crude PR Adjusted PR* p-value
(95% CI) (95% CI) (95% CI) (95% CI)
Level 1: Sociodemographic characteristcs
Age
<60 1.00 1.00 1.00 1.00
≥60 0.69 (0.60–0.81) 0.72 (0.62–0.84) <0.001 0.63 (0.49–0.83) 0.63 (0.48–0.81) 0.001
Sex
Female 1.00 1.00 1.00 1.00
Male 1.29 (1.09–1.52) 1.22 (1.04–1.43) 0.013 1.64 (1.24–2.17) 1.60 (1.22–2.09) <0.001
Skin colour/ethnicity
White 1.00 1.00
Non-white 1.11 (0.78–1.58) – 0.95 (0.58–1.56) –
Marital status
With partner 1.00 1.00
Without partner 1.02 (0.87–1.20) – 0.91 (0.69–1.19) –
Journal of
Lives alone
No 1.00 1.00
Yes 1.05 (0.84–1.31) – 1.05 (0.72–1.53) –
Schooling
<8 years 0.97 (0.83–1.15) – 0.80 (0.61–1.05) 0.86 (0.66–1.13) 0.279
≥8 years 1.00 1.00 1.00
Wound Care
Occupation
Working 1.00 1.00 1.00
Not working 1.05 (0.75–1.46) – 2.12 (0.88–5.07) 3.32 (1.30–8.44) <0.001
Income (minimum wages)
≤1 1.11 (0.93–1.31) – 0.90 (0.69–1.18) –
>1 1.00 1.00
Religion
Catholic/Protestant/other 1.00 1.00
No religion 1.31 (1.10–1.55) 1.20 (0.95–1.51) 0.152 1.17 (0.78–1.75) –
Level 2: Environmental characteristics: Access to public services
Piped water
Yes 1.00 1.00
No 1.16 (0.74–1.81) – 0.44 (0.08–2.54) –
Sanitary/sewage
Yes 1.00 1.00
No 0.89 (0.61–1.32) – 0.96 (0.54–1.71) –
Rubbish collection
Yes 1.00 1.00
No 1.07 (0.91–1.27) – 1.11 (0.84–1.46) –
Transport (to access CEDEBA)
Private (car or taxi) 1.00 1.00 1.00 1.00
© 2022 MA Healthcare Ltd
Public (bus and/or Metro) 0.84 (0.72–0.99) 0.84 (0.72–0.99) 0.045 0.72 (0.55–0.94) 0.72 (0.55–0.94) 0.017
Level 3: Clinical characteristics: diabetes duration (in years)
≤10 1.00 1.00 1.00 1.00
≤10 0.81 (0.69–0.95) 0.84 (0.71–0.98) 0.032 0.83 (0.62–1.10) 0.85 (0.64–1.13) 0.279
10 JOURNAL OF WOUND CARE VOL 31, NO 11, NOVEMBER 2022
practice
Table 3. Association between diabetic foot ulcer (DFU) and amputation, and sociodemographic and clinical
characteristics, as well as those related to access to public services and diabetic foot (DF) prevention activities at
primary healthcare (PHC) and communication of individuals living with type 2 diabetes followed up at the CEDEBA
diabetic foot clinic, Salvador, Bahia, Brazil 2019–2020 (n=253) (continued)
DFU Amputation
Variable Crude PR Adjusted PR* p-value Crude PR Adjusted PR* p-value
(95% CI) (95% CI) (95% CI) (95% CI)
Therapeutic adherence by the Morisky–Green test
Yes 1.00
No 1.09 (0.91–1.31) 1.08 (0.90–1.28) 0.403 0.92 (0.69–1.21) 0.91 (0.69–1.19) 0.485
Access to primary health care (PHC) in number of times a year
Rarely or not attending 0.96 (0.81–1.13) – 0.91 (0.69–1.20) –
≥1 1.00 1.0
Health education to prevent DF
Yes 1.00
No 0.87 (0.74–1.03) 1.09 (0.85–1.40) 0.481 0.91 (0.68–1.22) –
Screening of DF
Yes 1.00
No 0.75 (0.65–0.87) 0.73 (0.62–0.87) 0.001 0.71 (0.53–0.94) 0.72 (0.54–0.96) 0.035
Level 4: Communication
Understands everything in the service
Journal of
Yes 1.00
No 0.92 (0.74–1.15) – 0.74 (0.50–1.11) 0.70 (0.46–1.05) 0.049
Understands the terms
Yes 1.00
No 1.07 (0.90–1.26) – 1.08 (0.82–1.43) –
Asks when in doubt
Wound Care
Yes 1.00
No 1.17 (0.97–1.41) 1.19 (0.99–1.42) 0.080 1.20 (0.86–1.69) –
Has already left with doubts about the health situation
No 1.00
Yes 1.21 (1.03–1.42) 1.13 (0.94–1.35) 0.218 1.08 (0.79–1.46) –
Has already left with doubts about medications
No 1.00
Yes 1.05 (0.86-1.28) – 1.20 (0.88–1.63) –
Feels well cared for by health professionals
Yes 1.00
No 1.15 (0.97–1.38) 1.07 (0.87–1.32) 0.509 1.29 (0.96–1.73) –
Thinks that the doctor has made mistakes
No 1.00
Yes 1.17 (0.99–1.38) 1.12 (0.94–1.33) 0.222 1.36 (1.04–1.78) 1.41 (1.08–1.84) 0.017
Feels responsible for the treatment
Yes 1.00
No 1.05 (0.78–1.41) – 1.25 (0.81–1.94) –
Stopped seeking help for fear
No 1.00
Yes 1.26 (1.06–1.50) 1.22 (1.01–1.48) 0.057 1.21 (0.85–1.73) –
Stopped seeking help for not knowing how to say what has felt
No 1.00
Yes 1.10 (0.87–1.38) – 1.31 (0.92–1.87) –
© 2022 MA Healthcare Ltd
The doctor explained about diabetes complications
Yes 1.00
No 1.04 (0.81–1.33) – 0.94 (0.60–1.48) –
*Logistic regression with correction for PR was used separately and processed hierarchically with each outcome; CI—confidence interval; PR—prevalence ratio
JOURNAL OF WOUND CARE VOL 31, NO 11, NOVEMBER 2022 11
practice
Table 4. Multivariate regression model of factors associated with the development of diabetic foot ulcer (DFU)
among individuals living with type 2 diabetes followed up at the CEDEBA diabetic foot clinic, Salvador, Bahia, Brazil
2019–2020 (n=253)
Variable Model A Model B Model C Model D Final model**
(Block 1) (Blocks 1 and 2) (Blocks 1, 2 and 3) (Blocks 1, 2, p-value <0.05
PR (95% CI) PR (95% CI) PR (95% CI) 3 and 4)
PR (95% CI)
Level 1: Sociodemographic characteristcs
Age*
<60 1.00 1.00 1.00 1.00 1.00
≥60 0.72 (0.62–0.84) 0.71 (0.61–0.82) 0.73 (0.63–0.85) 0.73 (0.63–0.85) 0.71 (0.61–0.83)
Sex*
Female 1.00 1.00 1.00 1.00 1.00
Male 1.22 (1.04–1.43) 1.23 (1.05–1.43) 1.19 (1.02–1.39) 1.21 (1.03–1.41) 1.22 (1.04–1.43)
Religion*
Catholic/Protestant/others 1.00 1.00 1.00 1.00
No religion 1.20 (0.95–1.51) 1.20 (0.95–1.50) 1.22 (0.98–1.51) 1.23 (0.99–1.51) –
Journal of
Level 2: Environmental characteristics
Transport (to access CEDEBA)*
Private 1.00 1.00 1.00 1.00
Public 0.81 (0.70–0.95) 0.83 (0.71–0.96) 0.84 (0.72–0.98) 0.82 (0.71–0.96)
Level 3: Clinical characteristics
Wound Care
Diabetes duration (years)
≤10
>10 1.00 1.00
Therapeutic adherence by the Morisky–Green test
Yes 0.93 (0.78–1.10) 0.96 (0.80–1.16) Adjustment
No 1.00 1.00
Screening* 1.09 (0.92–1.29) 1.07 (0.91–1.26) Adjustment
Yes 1.00 1.00 1.00
No 0.79 (0.68–0.92) 0.79 (0.68–0.92) 0.79 (0.67–0.92)
Level 4: Communication
Asks when in doubt*
Yes 1.00
No 1.16 (0.98–1.39) –
Stopped seeking help for fear
No 1.00
Yes 1.16 (0.94–1.43) –
Model adjustment analyses
AIC 289.4264 284.4282 281.5009 281.7031 282.8243
© 2022 MA Healthcare Ltd
ROC curve 0.69 0.73 0.76 0.76 0.75
VIF 2.68
*252 observations; **Permanence of variables statistically associated with outcomes at a significance level of 5% (p-value ≤0.05), evaluated from the AIC, ROC curve and VIF;
AIC—Akaike Information Criterion; CI—confidence interval; PR—prevalence ratio; ROC—receiver operating characteristic; VIF—variance inflation factor
12 JOURNAL OF WOUND CARE VOL 31, NO 11, NOVEMBER 2022
practice
Table 5. Multivariate regression model of factors associated with the development of amputation among individuals
living with type 2 diabetes followed up at the CEDEBA diabetic foot clinic, Salvador, Bahia, Brazil 2019–2020 (n=253)
Variable Model E (Block 1) Model F Model G Model H Final Model 1
PR (95% CI) (Blocks 1 and 2) (Blocks 1, 2 and 3) (Blocks 1, 2, 3 & 4) PR (95% CI)
PR (95% CI) PR (95% CI) PR (95% CI)
Level 1: Sociodemographic characteristcs
Age*
<60 1.00 1.00 1.00 1.00 1.00
≥60 0.61 (0.47–0.78) 0.57 (0.45–0.73) 0.57 (0.44–0.73) 0.59 (0.46–0.77) 0.57 (0.45–0.74)
Sex*
Female 1.00 1.00 1.00 1.00 1.00
Male 1.60 (1.22–2.10) 1.62 (1.24–2.11) 1.58 (1.20–2.07) 1.59 (1.21–2.08) 1.61 (1.23–2.11)
Occupation*
Working 1.00 1.00 1.00 1.00 1.00
Not working 3.19 (1.27–8.04) 3.83 (1.48–9.90) 3.62 (1.41–9.30) 4.02 (1.56–10.36) 4.11 (1.57–10.75)
Level 2: Environmental characteristics
Journal of
Transport (to acess CEDEBA)*
Private 1.00 1.00 1.00 1.00
Public 0.65 (0.50–0.83) 0.66 (0.51–0.85) 0.63 (0.49–0.82) 0.63 (0.49–0.81)
Level 3: Clinical characteristics
Diabetes duration (years)
Wound Care
≤10 1.00 1.00 1.00
>10 1.04 (0.78–1.40) 1.03 (0.77–1.37) 1.03 (0.77–1.37)
Therapeutic adherence by the Morisky–Green test
Yes 1.00 1.00 1.00
No 0.93 (0.72–1.22) 0.97 (0.74–1.28) 0.99 (0.75–1.30)
Screening
Yes 1.00
No 0.81 (0.61–1.08) – –
Level 4: Communication
Understands everything in the service*
Yes 1.00 1.00
No 0.70 (0.47–1.03) 0.72 (0.49–1.06)
Thinks that the doctor has made mistakes
No 1.00
Yes 1.19 (0.91–1.56)
Model adjustment analyses
AIC 323.1903 313.8631 317.7495 316.7376 316.28
© 2022 MA Healthcare Ltd
ROC curve 0.70 0.72 0.73 0.74 0.73
VIF
AIC—Akaike Information Criterion; CI—confidence interval; PR—prevalence ratio; ROC—receiver operating characteristic; VIF—variance inflation factor
JOURNAL OF WOUND CARE VOL 31, NO 11, NOVEMBER 2022 13
practice
intervention by health professionals, to consider the social spheres to broaden understanding about the
cultural specificities and attitudes conditioned by sex. health needs of the target population.
Although the use of public transport has shown a
negative association with the development of the Conclusions
outcomes under study, the degree of functional The results of this investigation suggest that the
limitation determined by DF complications likely prevalence of DFUs and lower limb amputations in the
influences the choice of the type of transport used by studied population is high, and that these complications
people, considering the low accessibility of public are associated with: sociodemographic characteristics
transport. Therefore, the use of private transport to such as age, sex and occupation; environmental
access CEDEBA is probably a consequence of the characteristics such as the use of public transport to
existence of injuries that reduce the functional capacity access the CEDEBA; and characteristics related to access
of individuals. to DF screening programmes. However, the impact of
these factors on the causality network of DF can be
Limitations minimised through the development of health
The use of different approaches to obtain data, in promotion, prevention and assistance activities that
person and by telephone, can be considered a limitation consider, in addition to the clinical characteristics of
of the study. However, the objective data of the foot individuals, conditions that produce vulnerability.
evaluation were collected from medical records prepared The analysis of the factors associated with DFU from
by the main researcher, who used the same methodology this perspective has the potential to contribute to the
already used in the clinical evaluations of individuals. construction of strategies that incorporate, in addition
Moreover, the study involved a limited and to biomedical and epidemiological knowledge,
homogeneous number of participants, which limited formulations developed in the social and human
Journal of
the drawing of conclusions with strong evidence spheres to broaden the understanding about the health
capable of confirming the existence of an association needs of the target population. In this sense, new
between certain demographic, socioeconomic and studies with greater analytical power should be
programmatic characteristics, and the development of encouraged to investigate the role that
complications related to DF. However, the results sociodemographic, economic, environmental and
presented so far are promising, as they have the programmatic characteristics have on the development
potential to contribute to the identification of of DF injuries to increase understanding of interference,
Wound Care
conditions of vulnerability of the population under entanglement and significance of these factors on the
study. The analysis of the factors associated with DF course of the disease. JWC
from the point of view of vulnerability has the potential
to offer subsidies for the construction of health practices
Acknowledgements
that incorporate, in addition to biomedical and The authors would like to thank the CEDEBA patients for their contribution
epidemiological knowledge, formulations developed in to this research.
References
1 Zhang P, Lu J, Jing Y et al. Global epidemiology of diabetic foot 9 Armstrong DG, Wrobel J, Robbins JM. Guest editorial: are diabetes-
ulceration: a systematic review and meta-analysis. Ann Med 2017; related wounds and amputations worse than cancer? Int Wound J 2007;
49(2):106–116. https://doi.org/10.1080/07853890.2016.1231932 4(4):286–287. https://doi.org/10.1111/j.1742-481X.2007.00392.x
2 Rastogi A, Goyal G, Kesavan R et al. Long term outcomes after incident 10 Hingorani A, LaMuraglia GM, Henke P et al. The management of
diabetic foot ulcer: multicenter large cohort prospective study (EDI-FOCUS diabetic foot: a clinical practice guideline by the Society for Vascular
investigators) epidemiology of diabetic foot complications study. Diabetes Surgery in collaboration with the American Podiatric Medical Association
Res Clin Pract 2020; 162:108113. https://doi.org/10.1016/j. and the Society for Vascular Medicine. J Vasc Surg 2016; 63(2 Suppl):3S–
diabres.2020.108113 21S. https://doi.org/10.1016/j.jvs.2015.10.003
3 International Diabetes Federation. IDF Diabetes Atlas, 9th edition. 2019. 11 Duncan BB, Chor D, Aquino EML et al. [Chronic non-communicable
https://diabetesatlas.org/atlas/ninth-edition (accessed 4 October 2022) diseases in Brazil: priorities for disease management and research] [In
4 Schaper NC, Apelqvist J, Bakker K. The international consensus and Portuguese]. Rev Saúde Pública 2012; 46(suppl 1):126–134. https://doi.
practical guidelines on the management and prevention of the diabetic org/10.1590/S0034-89102012000700017
foot. Curr Diab Rep 2003; 3(6):475–479. https://doi.org/10.1007/ 12 do Carmo ME, Guizardi FL. [The concept of vulnerability and its
s11892-003-0010-4 meanings for public policies in health and social welfare] [In Portuguese].
5 Armstrong DG, Lavery LA, Harkless LB. Treatment-based classification Cad Saúde Pública 2018; 34(3). https://doi.
system for assessment and care of diabetic feet. J Am Podiatr Med Assoc org/10.1590/0102-311X00101417
1996; 86(7):311–316. https://doi.org/10.7547/87507315-86-7-311 13 Agardh E, Allebeck P, Hallqvist J et al. Type 2 diabetes incidence and
6 Lavery LA, Armstrong DG, Vela SA et al. Practical criteria for screening socio-economic position: a systematic review and meta-analysis. Int J
patients at high risk for diabetic foot ulceration. Arch Intern Med 1998; Epidemiol 2011; 40(3):804–818. https://doi.org/10.1093/ije/dyr029
© 2022 MA Healthcare Ltd
158(2):157–162. https://doi.org/10.1001/archinte.158.2.157 14 Rastogi A, Bhansali A. Diabetic foot infection: an indian scenario.
7 Bowling FL, Rashid ST, Boulton AJM. Preventing and treating foot J Foot Ankle Surg (Asia-Pacific) 2016; 3(2):71–79. https://doi.org/10.5005/
complications associated with diabetes mellitus. Nat Rev Endocrinol 2015; jp-journals-10040-1052
11(10):606–616. https://doi.org/10.1038/nrendo.2015.130 15 Instituto Brasileiro de Geografia e Estatística. [Sociodemographic and
8 van Netten JJ, Price PE, Lavery LA et al. Prevention of foot ulcers in the Health Indicators in Brazil] [In Portuguese]. 2009. https://tinyurl.com/
at-risk patient with diabetes: a systematic review. Diabetes Metab Res Rev mryz374d (accessed 4 October 2022)
2016; 32(Suppl 1):84–98. https://doi.org/10.1002/dmrr.2701 16 Riaz M, Miyan Z, Zaidi SI et al. Characteristics of a large cohort of
14 JOURNAL OF WOUND CARE VOL 31, NO 11, NOVEMBER 2022
practice
patients with diabetes having at-risk feet and outcomes in patients with
foot ulceration referred to a tertiary care diabetes unit. Int Wound J 2016; Reflective questions
13(5):594–599. https://doi.org/10.1111/iwj.12289 ● What paths should knowledge production take to contribute
17 Parisi MCR, Moura Neto A, Menezes FH et al. Baseline characteristics
to a reduction in the number of amputations related to
and risk factors for ulcer, amputation and severe neuropathy in diabetic
diabetic foot (DF)?
foot at risk: the BRAZUPA study. Diabetol Metab Syndr 2016; 8(1):25.
● How can health professionals act at the level of micropolicy
https://doi.org/10.1186/s13098-016-0126-8
18 Chaudhary S, Bhansali A, Rastogi A. Mortality in Asian Indians with to minimise the vulnerability of these patients?
Charcot’s neuroarthropathy: a nested cohort prospective study. ● How should healthcare systems be organised to mitigate
Acta Diabetol 2019; 56(12):1259–1264. https://doi.org/10.1007/ age- and gender-related risk in the case of DF?
s00592-019-01376-9
19 Coffey L, Mahon C, Gallagher P. Perceptions and experiences of
diabetic foot ulceration and foot care in people with diabetes: a qualitative
meta-synthesis. Int Wound J 2019; 16(1):183–210. https://doi.org/10.1111/
iwj.13010 v20.34481
20 Gupta SK, Lakshmi PV, Kaur M, Rastogi A. Role of self-care in 25 Campos RT, Ferrer AL, da Gama CA et al. [Assesment of quality of
COVID-19 pandemic for people living with comorbidities of diabetes and access in primary care in a large Brazilian city in the perspective of user]
hypertension. J Family Med Prim Care 2020; 9(11):5495–5501. https://doi. [In Portuguese]. Saúde Em Debate 2014; 38(special). https://doi.
org/10.4103/jfmpc.jfmpc_1684_20 org/10.5935/0103-1104.2014S019
21 Jude E, Rastogi A. COVID-19 pandemic and life style modification for 26 Spedo SM, da Silva Pinto, Tanaka OY. [The difficult access to
people with diabetes. Open Diabetes J 2021. https://tinyurl.com/42ftzkb8 secondary health care services: São Paulo city case study, Brazil] [In
(accessed 17 October 2022) Portuguese]. Physis 2010; 20(3). https://doi.org/10.1590/
22 dos Santos KP, da Luz SC, Mochizuki L, d’Orsi E. [Burden of disease S0103-73312010000300014
from lower limb amputations attributable to diabetes mellitus in Santa 27 Harding JL, Pavkov ME, Magliano DJ et al. Global trends in diabetes
Catarina State, Brazil, 2008–2013] [In Portuguese]. Cad Saúde Pública complications: a review of current evidence. Diabetologia 2019;
2018; 34(1). https://tinyurl.com/yc8dntpf (accessed 4 October 2022) 62(1):3–16. https://doi.org/10.1007/s00125-018-4711-2
23 Hanashiro R, Correia VD, Sugawara AT. [Social inclusion in the labour 28 Rossaneis MA, Haddad M do CFL, Mathias TA de F, Marcon SS.
market of amputees in the process of rehabilitation] [In Portuguese]. Differences in foot self-care and lifestyle between men and women with
Acta Fisiátrica 2018; 25(3). https://tinyurl.com/fshtw2ub (accessed 4 diabetes mellitus. Rev Lat Am Enfermagem 2016; 24:e2761. https://doi.
October 2022) org/10.1590/1518-8345.1203.2761
Journal of
24 Silva FM, Viana MCA, Barreto JOM et al. [Evidence brief for health 29 Botton A, Cúnico SD, Strey MN. [Gender differences in the access to
policy-making: prevention and control of diabetic foot in primary health health services: necesssary problematization] [In Portuguese]. Mudanças
care] [In Portuguese]. BIS 2019; 20(2). https://doi.org/10.52753/bis.2019. 2017; 25(1):67–72
Wound Care
© 2022 MA Healthcare Ltd
JOURNAL OF WOUND CARE VOL 31, NO 11, NOVEMBER 2022 15
You might also like
- Chung2020 Article PrecisionMedicineInDiabetesACoDocument23 pagesChung2020 Article PrecisionMedicineInDiabetesACoFilipa Figueiredo100% (1)
- Deleterious Dozen DMT2Document18 pagesDeleterious Dozen DMT2cecilia zavala100% (1)
- Metode Kualitatif DiabeticDocument8 pagesMetode Kualitatif DiabeticIyanNo ratings yet
- Pie Diabetico - Equipo MultidisciplinarioDocument7 pagesPie Diabetico - Equipo MultidisciplinarioMartina HuamánNo ratings yet
- Walsh2015association of Diabetic Foot Ulcer and Death in A Population-Based Cohort From The United KingdomDocument6 pagesWalsh2015association of Diabetic Foot Ulcer and Death in A Population-Based Cohort From The United KingdomAnonymous SMLzNANo ratings yet
- Ciencias Del Comportamiento en La Optimización de La Terapia Farmacológica y No Farmacológica para La Diabetes Tipo 2 (2021)Document19 pagesCiencias Del Comportamiento en La Optimización de La Terapia Farmacológica y No Farmacológica para La Diabetes Tipo 2 (2021)7 MNTNo ratings yet
- Diabetes and PeriodontitisDocument10 pagesDiabetes and PeriodontitisRobins DhakalNo ratings yet
- Diabetes and Mental HealthDocument3 pagesDiabetes and Mental HealthVENNA FADILLAHNo ratings yet
- DPN - Iberoamericanjm-3-1-18Document8 pagesDPN - Iberoamericanjm-3-1-18ganesh raoNo ratings yet
- Prevalence and Risk Factors For ChronicDocument10 pagesPrevalence and Risk Factors For ChronicKhoirul AnamNo ratings yet
- Review Article Stem Cell Therapy For Diabetic Foot Ulcers: Theory and PracticeDocument12 pagesReview Article Stem Cell Therapy For Diabetic Foot Ulcers: Theory and PracticeNenen DestianiNo ratings yet
- NCD View Point 3Document3 pagesNCD View Point 3upashana medhiNo ratings yet
- HHS Public Access: Update On Management of Diabetic Foot UlcersDocument19 pagesHHS Public Access: Update On Management of Diabetic Foot UlcersPUSKESMAS KECAMATAN KEPULAUAN SERIBU UTARANo ratings yet
- Perspectives of Nursing in The Care of The Patient With Diabetes MellitusDocument7 pagesPerspectives of Nursing in The Care of The Patient With Diabetes MellitusSammy OhNo ratings yet
- 620-Article Text-1231-1-10-20220127Document8 pages620-Article Text-1231-1-10-20220127Yusnita OktaviaNo ratings yet
- Article 3Document17 pagesArticle 3Um ShooqNo ratings yet
- ITC Type 2 Diabetes 2019Document16 pagesITC Type 2 Diabetes 2019ALEJANDRO DUEÑAS GUTIERREZNo ratings yet
- Relationshipbetween Knowledgeand Attitudeabout Preventionof Diabetes Mellitus Complicationsin Diabetes Mellitus PatientsDocument8 pagesRelationshipbetween Knowledgeand Attitudeabout Preventionof Diabetes Mellitus Complicationsin Diabetes Mellitus Patientscheatingw995No ratings yet
- Dmso 13 3703Document9 pagesDmso 13 3703Eva Cica SusantiNo ratings yet
- Depression and TB Outcomes 1Document13 pagesDepression and TB Outcomes 1Roger CNo ratings yet
- The Emergence of Non-Communicable Disease in Indonesia: Dyah PurnamasariDocument2 pagesThe Emergence of Non-Communicable Disease in Indonesia: Dyah Purnamasarinene_luciaNo ratings yet
- Type 2 Diabetes The Lancet 2022Document18 pagesType 2 Diabetes The Lancet 2022Valentina Kerguelen HernándezNo ratings yet
- Neuropatia DiabéticaDocument18 pagesNeuropatia DiabéticaGustavo PestanaNo ratings yet
- Div Class Title An Insight Into The Public Acceptance of Nutrigenomic Based Personalised Nutrition DivDocument10 pagesDiv Class Title An Insight Into The Public Acceptance of Nutrigenomic Based Personalised Nutrition DivLaila FauzaNo ratings yet
- Clinical and Behavioral Factors Associated With Management Outcome in Hospitalized Patients With Diabetic Foot UlcerDocument5 pagesClinical and Behavioral Factors Associated With Management Outcome in Hospitalized Patients With Diabetic Foot UlcerIndah Nevhita LNo ratings yet
- Liu 2019Document8 pagesLiu 2019Andi sutandiNo ratings yet
- 2018 A Global Overview of Precision Medicine in Type 2 DiabetesDocument12 pages2018 A Global Overview of Precision Medicine in Type 2 Diabetesguanyulin01No ratings yet
- Assesing The ProblemDocument9 pagesAssesing The Problemakko aliNo ratings yet
- JCM 10 00797Document11 pagesJCM 10 00797alazarNo ratings yet
- Diabetes and Back Pain: Markers of Diabetes Disease Progression Are Associated With Chronic Back PainDocument6 pagesDiabetes and Back Pain: Markers of Diabetes Disease Progression Are Associated With Chronic Back PainabdulfatahalhemeryNo ratings yet
- Lep266 282Document17 pagesLep266 282Hasana NurNo ratings yet
- Nutrigenetics-Personalized Nutrition in The Genetic Age: Review ArticleDocument8 pagesNutrigenetics-Personalized Nutrition in The Genetic Age: Review Articleravenwatch1No ratings yet
- Article 1567163840Document4 pagesArticle 1567163840lailatul husnaNo ratings yet
- Jurnal ASKEP KOMUNITASDocument8 pagesJurnal ASKEP KOMUNITASSitiraihanNo ratings yet
- Gambaran Tingkat Health Literacy Pasien Ulkus Kaki Diabetik Ferlan Ansye PondaagDocument6 pagesGambaran Tingkat Health Literacy Pasien Ulkus Kaki Diabetik Ferlan Ansye PondaagFairudzal DianaNo ratings yet
- Healthframework PaperDocument9 pagesHealthframework Paperapi-449184986No ratings yet
- Anderson e Durstine (2019) Physical Activity, Exercise, and Chronic DiseasesDocument8 pagesAnderson e Durstine (2019) Physical Activity, Exercise, and Chronic DiseasesAna Flávia SordiNo ratings yet
- Direct Medical Cost of Type 2 Diabetes in SingaporeDocument11 pagesDirect Medical Cost of Type 2 Diabetes in SingaporeElla FaotNo ratings yet
- JDM 2017110814284359Document8 pagesJDM 2017110814284359Mochamad BilalNo ratings yet
- 10 1111@odi 13236Document10 pages10 1111@odi 13236vero alvarezNo ratings yet
- Bidirectional AssociationDocument10 pagesBidirectional AssociationAndrea MorenoNo ratings yet
- Genetics of Type 2 Diabetes Past Present and FuturDocument12 pagesGenetics of Type 2 Diabetes Past Present and FuturChengwustZhangNo ratings yet
- Jurnal 7 PDFDocument10 pagesJurnal 7 PDFAdi SuciptoNo ratings yet
- JCM 10 05383Document24 pagesJCM 10 05383bere laraNo ratings yet
- TCC 5Document8 pagesTCC 5rafacosta3679No ratings yet
- Periodontal Complications With ObesityDocument31 pagesPeriodontal Complications With ObesityMaria pérezNo ratings yet
- Seminar: Epidemiology and Global Trends in Type 2 DiabetesDocument18 pagesSeminar: Epidemiology and Global Trends in Type 2 DiabetesRoopaNo ratings yet
- Elementsprinciplesofartdesig 120213105802 Phpapp01Document284 pagesElementsprinciplesofartdesig 120213105802 Phpapp01Analyn QueroNo ratings yet
- Chronic Non Communicable DiseaseDocument13 pagesChronic Non Communicable DiseaseGabryelNo ratings yet
- 2017 Subinical DiabetesDocument24 pages2017 Subinical DiabetesLuís Mauricio LimaNo ratings yet
- Journal Homepage: - : IntroductionDocument8 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Journal of Diabetes and Its Complications: Yiqun Chen, Frank A. Sloan, Arseniy P. YashkinDocument6 pagesJournal of Diabetes and Its Complications: Yiqun Chen, Frank A. Sloan, Arseniy P. YashkinrodrigoNo ratings yet
- Health Beliefs, Self-Care Behaviors and Quality of Life in Adults With Type 2 DiabetesDocument9 pagesHealth Beliefs, Self-Care Behaviors and Quality of Life in Adults With Type 2 DiabetesgamzeNo ratings yet
- Adiposity Measurements and Non-Surgical Periodontal Therapy Outcomes.Document8 pagesAdiposity Measurements and Non-Surgical Periodontal Therapy Outcomes.yomiboyNo ratings yet
- Articolo Originale. Documento Di Consenso Tra European Federation of Periodontology e International Diabetes FederationDocument12 pagesArticolo Originale. Documento Di Consenso Tra European Federation of Periodontology e International Diabetes Federationnensy121No ratings yet
- Underlying Causes and Co-Existence of Malnutrition and Infections: An Exceedingly Common Death Risk in CancerDocument11 pagesUnderlying Causes and Co-Existence of Malnutrition and Infections: An Exceedingly Common Death Risk in CancerBBD BBDNo ratings yet
- Diabetic Foot Full ThesisDocument5 pagesDiabetic Foot Full Thesishcivczwff100% (1)
- Physical Exercise and Major Depressive Disorder in Adults Systematic Review and Meta AnalysisDocument17 pagesPhysical Exercise and Major Depressive Disorder in Adults Systematic Review and Meta AnalysisErick NunesNo ratings yet
- Painful Diabetic Polyneuropathy: A Comprehensive Guide for CliniciansFrom EverandPainful Diabetic Polyneuropathy: A Comprehensive Guide for CliniciansNo ratings yet
- Tropical NephrologyFrom EverandTropical NephrologyGeraldo Bezerra da Silva JuniorNo ratings yet