You might also like
- SARS-CoV-2 Viral Outbreak Investigation: Laboratory Perspective: Clinical Updates in COVID-19From EverandSARS-CoV-2 Viral Outbreak Investigation: Laboratory Perspective: Clinical Updates in COVID-19Rating: 3 out of 5 stars3/5 (1)
- SARS-CoV-2 Viral Outbreak Investigation: Laboratory PerspectiveFrom EverandSARS-CoV-2 Viral Outbreak Investigation: Laboratory PerspectiveNo ratings yet
- COVISHIELD TAG REPORT EULvaccineDocument24 pagesCOVISHIELD TAG REPORT EULvaccineMrinal SivadasanNo ratings yet
- Recommendation For An Emergency Use Listing of Covid-19 Vaccine (Vero Cell), Inactivated Submitted by SinovacDocument36 pagesRecommendation For An Emergency Use Listing of Covid-19 Vaccine (Vero Cell), Inactivated Submitted by Sinovacindra sanjayaNo ratings yet
- TRS 910 Annex2-WHO Revision of The WHO Recommendations For The Production and Control of IPVDocument28 pagesTRS 910 Annex2-WHO Revision of The WHO Recommendations For The Production and Control of IPVaprilmm419No ratings yet
- KN TamDocument2 pagesKN TamHữu Phương ĐinhNo ratings yet
- WHO 2019 nCoV Vaccines SAGE Recommendation Sinovac CoronaVac Background 2021.1 EngDocument30 pagesWHO 2019 nCoV Vaccines SAGE Recommendation Sinovac CoronaVac Background 2021.1 EngJet HernandezNo ratings yet
- WHO OperationalTool EfficientLotRelease V20jan2021Document3 pagesWHO OperationalTool EfficientLotRelease V20jan2021annas rizky bramokoNo ratings yet
- WHO IVB 12.10 EngDocument36 pagesWHO IVB 12.10 EngJjNo ratings yet
- The Covid-19 Pandemic and Haemoglobin Disorders: Vaccinations & Therapeutic DrugsDocument53 pagesThe Covid-19 Pandemic and Haemoglobin Disorders: Vaccinations & Therapeutic DrugsJuanGabrielVillamizarNo ratings yet
- Ipv Operational Manual PDFDocument36 pagesIpv Operational Manual PDFrajendra gajulaNo ratings yet
- WHO 2019 nCoV Vaccines SAGE - Recommendation BNT162b2 2021.1 EngDocument7 pagesWHO 2019 nCoV Vaccines SAGE - Recommendation BNT162b2 2021.1 EngFernando PerezNo ratings yet
- US State Pilot Program Nov162020LDocument4 pagesUS State Pilot Program Nov162020LWJHL News Channel ElevenNo ratings yet
- Who Covid 2019 Solidarityvaccinetrial Expandedoutline 28mayDocument17 pagesWho Covid 2019 Solidarityvaccinetrial Expandedoutline 28mayBasra AhmadNo ratings yet
- Foot-And-: Vaccination Sample Testing of FMD Disease Within PakistanDocument14 pagesFoot-And-: Vaccination Sample Testing of FMD Disease Within PakistanQuratulainNo ratings yet
- Information and Criteria For Prioritizing Diagnostic TestsDocument5 pagesInformation and Criteria For Prioritizing Diagnostic TestsLenin CarrilloNo ratings yet
- Smallpox Eradication: Destruction of Variola Virus Stocks: Report by The Director-GeneralDocument5 pagesSmallpox Eradication: Destruction of Variola Virus Stocks: Report by The Director-GeneralPutri Nur IrsyadiyahNo ratings yet
- Smallpox Eradication: Destruction of Variola Virus Stocks: Report by The Director-GeneralDocument5 pagesSmallpox Eradication: Destruction of Variola Virus Stocks: Report by The Director-GeneralPutri Nur IrsyadiyahNo ratings yet
- WHO 2019 nCoV Vaccines SAGE Prioritization 2020.1 EngDocument31 pagesWHO 2019 nCoV Vaccines SAGE Prioritization 2020.1 EngJosh San PedroNo ratings yet
- 4.08 WHO - Cholera - Vaccines - Emergencies - 2005Document39 pages4.08 WHO - Cholera - Vaccines - Emergencies - 2005Ricardo AlvaradoNo ratings yet
- Consensus Interim Recommendations On The Use of Coronavac in HK As of 19 Feb 2021Document6 pagesConsensus Interim Recommendations On The Use of Coronavac in HK As of 19 Feb 2021Felipe Barros S.No ratings yet
- COVID-19 Animal Models: Ad Hoc Working GroupDocument4 pagesCOVID-19 Animal Models: Ad Hoc Working GroupAuuhotelarNo ratings yet
- HIV 12 STAT-PAK Public - Report - FinalDocument12 pagesHIV 12 STAT-PAK Public - Report - FinalAbebe TadesseNo ratings yet
- 21 06 04 EUL 0590-010-00 - Sure Status COVID-19 Card Test - PR - V - 1.0Document17 pages21 06 04 EUL 0590-010-00 - Sure Status COVID-19 Card Test - PR - V - 1.0Maciej OONo ratings yet
- Interim Recommendations For Use of The Inactivated Covid-19 Vaccine, Coronavac, Developed by SinovacDocument9 pagesInterim Recommendations For Use of The Inactivated Covid-19 Vaccine, Coronavac, Developed by SinovacNathaly BarretoNo ratings yet
- Mm7038e2 HDocument5 pagesMm7038e2 HJungkook JkNo ratings yet
- WHO DI 33-3 Condoms1Document24 pagesWHO DI 33-3 Condoms1Krishna Mohan.p.rNo ratings yet
- Journal For The Generic Medicines Sector Journal of Generic Medicines: The BusinessDocument13 pagesJournal For The Generic Medicines Sector Journal of Generic Medicines: The BusinessBilal AbbasNo ratings yet
- Operacion Warp SpeedDocument54 pagesOperacion Warp SpeedfibanezNo ratings yet
- A Guide To Introducing: Inactivated Polio VaccineDocument48 pagesA Guide To Introducing: Inactivated Polio VaccineJjNoznaugNo ratings yet
- Reports of Suspected Adverse Reaction To COVID-19 VaccinesDocument23 pagesReports of Suspected Adverse Reaction To COVID-19 VaccinesEngkiong GoNo ratings yet
- Addressing The Challenges and Opportunities of The Polio Endgame: Lessons For The FutureDocument8 pagesAddressing The Challenges and Opportunities of The Polio Endgame: Lessons For The Futuremuhfajar1_42539617No ratings yet
- PACE Outbreaks Ebola Marburg enDocument123 pagesPACE Outbreaks Ebola Marburg enGilbert Solomon Tantono100% (1)
- Interim Statement On COVID-19 Vaccines in The Context of The Circulation of The Omicron SARS-CoV-2 Variant From The WHO Technical Advisory Group On COVID-19 Vaccine Composition (TAG-CO-VAC)Document5 pagesInterim Statement On COVID-19 Vaccines in The Context of The Circulation of The Omicron SARS-CoV-2 Variant From The WHO Technical Advisory Group On COVID-19 Vaccine Composition (TAG-CO-VAC)Sneha SinghNo ratings yet
- s13063 021 05329 yDocument2 pagess13063 021 05329 ymeth holaNo ratings yet
- Joint FAO/WHO Expert Committee On Food Additives (JECFA) : November-2020 - Summary-And-Conclusion - PDF?SFVRSN 52aef206 - 5Document10 pagesJoint FAO/WHO Expert Committee On Food Additives (JECFA) : November-2020 - Summary-And-Conclusion - PDF?SFVRSN 52aef206 - 53utiaNo ratings yet
- Office: of The SecretaryDocument16 pagesOffice: of The SecretaryJoseph RepotenteNo ratings yet
- PV Guidance DocumentDocument54 pagesPV Guidance DocumentRenneyNo ratings yet
- WHO GUide On Vaccine ImplementationDocument80 pagesWHO GUide On Vaccine ImplementationNodarNo ratings yet
- U D C C E: Niversity of Haka Pplied Hemistry and Hemical NgineeringDocument6 pagesU D C C E: Niversity of Haka Pplied Hemistry and Hemical NgineeringMD: Shamim HossainNo ratings yet
- Responding To A Poliovirus Outbreak: Tandard Perating RoceduresDocument34 pagesResponding To A Poliovirus Outbreak: Tandard Perating RoceduresenoNo ratings yet
- Approval Vaccine RussiaDocument2 pagesApproval Vaccine RussialukmanNo ratings yet
- WHO 2019 EngDocument9 pagesWHO 2019 Engsweet123 cakeNo ratings yet
- Centre's Vaccination PlanDocument27 pagesCentre's Vaccination PlanRepublic WorldNo ratings yet
- India - Vaccination Roll Out PlanDocument27 pagesIndia - Vaccination Roll Out PlanTmailNo ratings yet
- WHO 2019 nCoV Policy Brief Vaccine Trial Design 2021.1 EngDocument38 pagesWHO 2019 nCoV Policy Brief Vaccine Trial Design 2021.1 EngEunike KaramoyNo ratings yet
- National Guidance For The Recovery of Elective Surgery in ChildrenDocument50 pagesNational Guidance For The Recovery of Elective Surgery in ChildrenJulia RamirezNo ratings yet
- WHO 2019 nCoV Lab Testing 2021.1 EngDocument16 pagesWHO 2019 nCoV Lab Testing 2021.1 EngEddy KurniawanNo ratings yet
- PolioPipeline 08Document8 pagesPolioPipeline 08Subhajit BhattacharjeeNo ratings yet
- The Pfizer BioNTech (BNT162b2) COVID-19 Vaccine - What You Need To KnowDocument5 pagesThe Pfizer BioNTech (BNT162b2) COVID-19 Vaccine - What You Need To KnowdianavemNo ratings yet
- Basic Malaria Microscopy Part I. Learner's Guide, 2nd Edition-9241547820Document88 pagesBasic Malaria Microscopy Part I. Learner's Guide, 2nd Edition-9241547820Bien TuanzonNo ratings yet
- EUL 0653-143-00 OnSiteCOVID-19 Ag RapidTest v1.0Document18 pagesEUL 0653-143-00 OnSiteCOVID-19 Ag RapidTest v1.0Maciej OONo ratings yet
- C Ovid Taskforce Update 11Document4 pagesC Ovid Taskforce Update 11Patricia FernándezNo ratings yet
- Annex 2: © World Health Organization WHO Technical Report Series, No. 926, 2004Document25 pagesAnnex 2: © World Health Organization WHO Technical Report Series, No. 926, 2004Iqbal RahmansyahNo ratings yet
- COVID 19 Antigen Testing GuidelinesDocument12 pagesCOVID 19 Antigen Testing GuidelinesStephanie SánchezNo ratings yet
- WHO 2019 nCoV Vaccines SAGE Recommendation BBV152 2022.1 EngDocument10 pagesWHO 2019 nCoV Vaccines SAGE Recommendation BBV152 2022.1 EngJjNo ratings yet
- Lessons Learned and Good Practices Immunization Activities During The COVID 19 Pandemic 2021Document86 pagesLessons Learned and Good Practices Immunization Activities During The COVID 19 Pandemic 2021nejatseid46No ratings yet
- Ivermectin Interest Group v4Document41 pagesIvermectin Interest Group v4SundayTimesZA100% (1)
- Yagisawa Et Al 2021 - Global Trends in Clinical Studies of Ivermectin in COVID-19 - The Japanese Journal of Antibiotics 74-1 - 44-95Document52 pagesYagisawa Et Al 2021 - Global Trends in Clinical Studies of Ivermectin in COVID-19 - The Japanese Journal of Antibiotics 74-1 - 44-95Samsara ChomolungmaNo ratings yet
- Six Month Safety and Efficacy of The BNT162b2 mRNA COVID-19 VaccineDocument21 pagesSix Month Safety and Efficacy of The BNT162b2 mRNA COVID-19 VaccineJoseph Adinolfi Jr.100% (2)
- Oral Iron Supplementation in Iron-Deficient Women-How Much and How OftenDocument9 pagesOral Iron Supplementation in Iron-Deficient Women-How Much and How Oftenshofa nur rahmannisaNo ratings yet
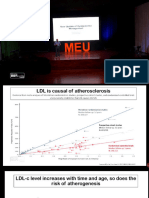
- DislipidemiaDocument35 pagesDislipidemiashofa nur rahmannisaNo ratings yet
- Neurocysticercosis in Qatari Patients - Case ReportsDocument5 pagesNeurocysticercosis in Qatari Patients - Case Reportsshofa nur rahmannisaNo ratings yet
- Processed Pork Is The Most Frequently Consumed Type of PorkDocument9 pagesProcessed Pork Is The Most Frequently Consumed Type of Porkshofa nur rahmannisaNo ratings yet
- Antiepilepsi & AntikonvulsiDocument8 pagesAntiepilepsi & Antikonvulsishofa nur rahmannisaNo ratings yet
- Epidemiologi Kerja 2020Document33 pagesEpidemiologi Kerja 2020shofa nur rahmannisaNo ratings yet
- Imaging of Acute Abdomen in PregnancyDocument18 pagesImaging of Acute Abdomen in Pregnancyshofa nur rahmannisaNo ratings yet
- Obstetric ExaminationDocument26 pagesObstetric Examinationshofa nur rahmannisaNo ratings yet
- Currentstatusof Cognitivebehavioral Therapyforadult Attention-Deficit Hyperactivity DisorderDocument13 pagesCurrentstatusof Cognitivebehavioral Therapyforadult Attention-Deficit Hyperactivity Disordershofa nur rahmannisaNo ratings yet
- Tomato Leaf CurlDocument7 pagesTomato Leaf CurlArpitha Shankar BandiNo ratings yet
- Transcription Prokaryotes 2012-cDocument27 pagesTranscription Prokaryotes 2012-cAnupama PatiNo ratings yet
- Biotechnology Principles & ProcessesDocument3 pagesBiotechnology Principles & ProcessesKambaska Kumar BeheraNo ratings yet
- Vpa 25Document11 pagesVpa 25Ada CelisNo ratings yet
- Modul Interna Tropical MedicineDocument25 pagesModul Interna Tropical MedicineYifada SNo ratings yet
- History of Public HealthDocument38 pagesHistory of Public HealthEdgar DumagpiNo ratings yet
- Parasitology (Quiz 2)Document6 pagesParasitology (Quiz 2)Frances Jewel Len SuyoNo ratings yet
- Motility TestDocument14 pagesMotility TestmaleehaNo ratings yet
- Interpretation of Urinalysis Results PDFDocument7 pagesInterpretation of Urinalysis Results PDFDagnachew kasayeNo ratings yet
- Questions of Moodle Final 2019Document6 pagesQuestions of Moodle Final 2019Miki AberaNo ratings yet
- 12 Aerobic Gram-Positive BacilliDocument68 pages12 Aerobic Gram-Positive BacilliClarence SantosNo ratings yet
- Thrombocytopenia: Pathophysiology and ClassificationDocument4 pagesThrombocytopenia: Pathophysiology and Classificationvenni dimitriNo ratings yet
- T Box MutationDocument5 pagesT Box Mutationapi-399849391No ratings yet
- Cell Biology MCQDocument17 pagesCell Biology MCQVineet Mehta78% (9)
- CSF SamplesDocument14 pagesCSF SamplesEPHANTUS WAINAINANo ratings yet
- Fungi Classification MapDocument3 pagesFungi Classification MapShoaibNo ratings yet
- Medical Biology: T I L Ea A K - 1 G A M A TaDocument376 pagesMedical Biology: T I L Ea A K - 1 G A M A Tatiffylola100% (1)
- Genetics ExamDocument6 pagesGenetics ExamanewflorescaNo ratings yet
- Common Intestinal ParasitesDocument16 pagesCommon Intestinal ParasitesbaliuwNo ratings yet
- SV Bio 2021 1 enDocument7 pagesSV Bio 2021 1 enibrahimantar.25No ratings yet
- Laboratory Biological Safety Training v2Document63 pagesLaboratory Biological Safety Training v2mercentNo ratings yet
- Hepatitis C: Symptoms and SignsDocument2 pagesHepatitis C: Symptoms and Signsmueen hashmiNo ratings yet
- Ageing Research Reviews: A B C D e F C D eDocument18 pagesAgeing Research Reviews: A B C D e F C D eBradyNo ratings yet
- Hematology Part 1 NotesDocument23 pagesHematology Part 1 NotesDr. Benson BenjaminNo ratings yet
- Fenben Cancer Protocol 2Document10 pagesFenben Cancer Protocol 2Mikee Zoleta LaurelNo ratings yet
- Review On Canine Transmissible Venereal Tumor (CTVT)Document9 pagesReview On Canine Transmissible Venereal Tumor (CTVT)Igor UlcarNo ratings yet
- Pathogen Song LyricsDocument1 pagePathogen Song LyricsBenjie Modelo ManilaNo ratings yet
- BANABA Lagerstroemia Speciosa LEAF Extract As Anti-Bacterial SoapDocument1 pageBANABA Lagerstroemia Speciosa LEAF Extract As Anti-Bacterial SoapbelmarinaNo ratings yet
- Paper Seminario Jose EpulefDocument11 pagesPaper Seminario Jose EpulefJL EulefiNo ratings yet
- Science Q3 WK5.Document14 pagesScience Q3 WK5.Hellow FriendzNo ratings yet