You might also like
- Affidavit of Child SupportDocument2 pagesAffidavit of Child SupportJfm A Dazlac100% (9)
- 4 - Home Loan TerminolgyDocument210 pages4 - Home Loan Terminolgypurit83No ratings yet
- GROUP EYE CARE INSURANCE CERTIFICATEDocument41 pagesGROUP EYE CARE INSURANCE CERTIFICATEbutt7474No ratings yet
- IMM5743EDocument0 pagesIMM5743EWuilmer B. GuerreroNo ratings yet
- Please DocuSign These Documents UPS On-BoardDocument21 pagesPlease DocuSign These Documents UPS On-BoardJayeven EnglishNo ratings yet
- CCC Insurance Corporation VS CaDocument1 pageCCC Insurance Corporation VS CaAbegail GaledoNo ratings yet
- Terms of Use and Privacy PolicyDocument13 pagesTerms of Use and Privacy PolicyFarveen FarookNo ratings yet
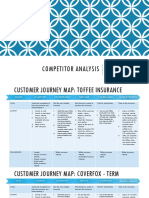
- Customer Journey MapDocument8 pagesCustomer Journey MapRia Narayan0% (1)
- Data Privacy ConsentDocument1 pageData Privacy ConsentNilda Buzeta GarciaNo ratings yet
- DATA PRIVACY CONSENT-EntregoDocument2 pagesDATA PRIVACY CONSENT-EntregoCamille Flores100% (1)
- Ai in Insurance Cheat Sheet DraftDocument8 pagesAi in Insurance Cheat Sheet DraftDinesh YepuruNo ratings yet
- RIBA Principal Designer PSC 2020 Final PDF Consultation VersionDocument36 pagesRIBA Principal Designer PSC 2020 Final PDF Consultation Versionalexandra SBNo ratings yet
- CROSS BORDER DATA TRANSFER CONSENT FORM - DECEMBER (1) (1) (1)Document3 pagesCROSS BORDER DATA TRANSFER CONSENT FORM - DECEMBER (1) (1) (1)FIDELIS MUSEMBINo ratings yet
- Shared FO-DPO-0.003 Member Consent - With Legal Dependents - Rev.04Document3 pagesShared FO-DPO-0.003 Member Consent - With Legal Dependents - Rev.04Jansen SalgadoNo ratings yet
- Consent GeneralDocument2 pagesConsent GeneralcathyNo ratings yet
- Request For Review of A Decision FormDocument3 pagesRequest For Review of A Decision FormArash ShamsNo ratings yet
- Background Check Disclosure Form SummaryDocument9 pagesBackground Check Disclosure Form SummaryLatasha wilson100% (1)
- Claim Dental Care Expenses 19110ADocument2 pagesClaim Dental Care Expenses 19110Alizita777No ratings yet
- Axicare Ealthcare Orporation: Form Template Control: Data Privacy Office/January 29, 2021/FO-DPO-0.002/Rev.05Document2 pagesAxicare Ealthcare Orporation: Form Template Control: Data Privacy Office/January 29, 2021/FO-DPO-0.002/Rev.05Agnasin, Ranelle Michael P.No ratings yet
- Applicant Consent Form: Date of BirthDocument1 pageApplicant Consent Form: Date of BirthErmilyn TablatinNo ratings yet
- Applicant Consent Form: Date of BirthDocument1 pageApplicant Consent Form: Date of BirthJasminNo ratings yet
- Boundless 2022 2023personal Information Collection Statement 1 2Document3 pagesBoundless 2022 2023personal Information Collection Statement 1 2Cui Tsz Ki 5A-07No ratings yet
- Romif (Global) - General - Docx Ali AlmahmoodDocument2 pagesRomif (Global) - General - Docx Ali AlmahmoodMuhamed MudherNo ratings yet
- 2020 Member ConsentDocument2 pages2020 Member ConsentA.D. VenturesNo ratings yet
- HealthConsent CDocument1 pageHealthConsent CsakondathabisoNo ratings yet
- ROMIFDocument2 pagesROMIFChester QuilalaNo ratings yet
- Insurance Direct Billing Submission Fillable FormDocument2 pagesInsurance Direct Billing Submission Fillable FormAfreen FathimaNo ratings yet
- Laya Healthcare out-patient claim form guideDocument2 pagesLaya Healthcare out-patient claim form guideDamoNo ratings yet
- TD Insurance PPN Consent FormDocument2 pagesTD Insurance PPN Consent FormMike Jonas GrabowskiNo ratings yet
- AXA Non Death Claim FormDocument4 pagesAXA Non Death Claim FormKenji ChinNo ratings yet
- Claim Form: (For Reimbursement of Expenses)Document4 pagesClaim Form: (For Reimbursement of Expenses)Shankar NathNo ratings yet
- Claim Health Care Benefits 19132ADocument2 pagesClaim Health Care Benefits 19132ACharles MoncyNo ratings yet
- QLM Life Medical Insurance Reimbursement FormDocument2 pagesQLM Life Medical Insurance Reimbursement FormWillard CustodioNo ratings yet
- UHIP Claim Form: Sun Life Assurance Company of Canada - 50150Document3 pagesUHIP Claim Form: Sun Life Assurance Company of Canada - 50150metstephNo ratings yet
- Portablehousingbenefit Signed 78c23934 4a73 4208 b98c Bd02ae35ee57Document3 pagesPortablehousingbenefit Signed 78c23934 4a73 4208 b98c Bd02ae35ee57eguasglobalresourcesltdNo ratings yet
- Privacy PolicyDocument3 pagesPrivacy PolicytheodorusardihartokoNo ratings yet
- UNUM Brochure 1.1.2020Document4 pagesUNUM Brochure 1.1.2020icbinwNo ratings yet
- STD Claim FormDocument8 pagesSTD Claim Formapi-314323052No ratings yet
- PH IcformDocument4 pagesPH IcformHihiNo ratings yet
- Privacy Notice Consent FormDocument2 pagesPrivacy Notice Consent Formapi-636475491No ratings yet
- April 2019 Hangar Flying NewsletterDocument7 pagesApril 2019 Hangar Flying NewsletterBeagle75No ratings yet
- Application For Assistance - Consents (Part 1)Document4 pagesApplication For Assistance - Consents (Part 1)L R RetiNo ratings yet
- Data Privacy Notice ExplainedDocument5 pagesData Privacy Notice Explainedangela maeNo ratings yet
- InLife Claims ReimbursementDocument2 pagesInLife Claims ReimbursementpluknoahjairusballertaNo ratings yet
- Group Medicare Enrollment FormDocument5 pagesGroup Medicare Enrollment FormChinmay P KalelkarNo ratings yet
- Fair Processing NoticeDocument5 pagesFair Processing NoticeSayem AhmedNo ratings yet
- ConsentDocument2 pagesConsentKatlego HectorNo ratings yet
- Revised Certified List Under Oath-ClientDocument2 pagesRevised Certified List Under Oath-ClientErene Rose EpanNo ratings yet
- Data Privacy Statement - 2018-04 (April 05)Document12 pagesData Privacy Statement - 2018-04 (April 05)lmcs.pacificcrossNo ratings yet
- OMA OM en Claims TravelDelayDocument4 pagesOMA OM en Claims TravelDelayreshwan aliNo ratings yet
- Declaration and Consent by Applicant: Page 1 of 2Document2 pagesDeclaration and Consent by Applicant: Page 1 of 2francesca zackeyNo ratings yet
- Ti Claim FormDocument8 pagesTi Claim FormHihiNo ratings yet
- Claim FormDocument4 pagesClaim Formmuhammad haroonNo ratings yet
- Reimbursement Form - GamayonDocument2 pagesReimbursement Form - Gamayonreese93No ratings yet
- Consent and declarationDocument2 pagesConsent and declarationsenthilkumar kNo ratings yet
- Durable Po ADocument5 pagesDurable Po AScottNo ratings yet
- Summary of Notice of Privact Practice Conditions of Admission andDocument3 pagesSummary of Notice of Privact Practice Conditions of Admission andShahho MustafaNo ratings yet
- Practo Privacy Policy FinalDocument17 pagesPracto Privacy Policy FinalRaghavBaldwaNo ratings yet
- Afya Imara App FormDocument10 pagesAfya Imara App Formiamcate9No ratings yet
- (V) (Vi) (Vii)Document2 pages(V) (Vi) (Vii)Jansen YenNo ratings yet
- Applicant Consent Form: Date of BirthDocument1 pageApplicant Consent Form: Date of BirthJoyce Axie KhoNo ratings yet
- Group Hospital Claim Form GuideDocument5 pagesGroup Hospital Claim Form GuideGelson Herrera0% (5)
- Reimbursement Request Form: Jayson Delos Reyes 43-00-00134-00865-0 1 White and CaseDocument2 pagesReimbursement Request Form: Jayson Delos Reyes 43-00-00134-00865-0 1 White and CaseJayson Delos ReyesNo ratings yet
- All States Federal FCRA Disclosure and AuthorizationDocument6 pagesAll States Federal FCRA Disclosure and Authorizationmarckeyiahayes1102No ratings yet
- Va ReleaseDocument1 pageVa Releaseapi-326532936No ratings yet
- Application Form: General Information: Selection Criteria For AccommodationDocument5 pagesApplication Form: General Information: Selection Criteria For AccommodationSIDDIG HASSAN SALAMAMNo ratings yet
- Pioneer v. Yap: Violation of co-insurance clause voids fire insurance policyDocument3 pagesPioneer v. Yap: Violation of co-insurance clause voids fire insurance policyShanicaNo ratings yet
- Sales of Goods - Law Teacher: HistoryDocument8 pagesSales of Goods - Law Teacher: Historysamuel samNo ratings yet
- British Microlight Test Pilot HandbookDocument8 pagesBritish Microlight Test Pilot HandbookErik HadleyNo ratings yet
- Form For Withdrawal by Claimant Due To Death of SubscriberDocument6 pagesForm For Withdrawal by Claimant Due To Death of SubscriberAkash MalikNo ratings yet
- Table of Benefits For Insurance CoverageDocument1 pageTable of Benefits For Insurance CoverageKareem EidNo ratings yet
- PFP T5Document7 pagesPFP T5JennieNo ratings yet
- ACE Variable IC Online Mock Exam - 08182021Document11 pagesACE Variable IC Online Mock Exam - 08182021Ana FelicianoNo ratings yet
- July 26 Benzie County Board of Commissioners Packet Ironman ContractDocument7 pagesJuly 26 Benzie County Board of Commissioners Packet Ironman ContractColin MerryNo ratings yet
- Cover Note MCI PT Antareja ResourcesDocument12 pagesCover Note MCI PT Antareja ResourcesHR & GA DepartmentNo ratings yet
- Foundation Course FC BOOK-URDU (State Life Pakistan)Document110 pagesFoundation Course FC BOOK-URDU (State Life Pakistan)Kamran AbdullahNo ratings yet
- CIR Vs Lincoln Case GR 119176Document4 pagesCIR Vs Lincoln Case GR 119176Alvin-Evelyn GuloyNo ratings yet
- Practitioner's Guide to Stochastic ReservingDocument75 pagesPractitioner's Guide to Stochastic ReservingDamien ServaisNo ratings yet
- Affidavit of Undertaking Surety ObligorDocument2 pagesAffidavit of Undertaking Surety ObligorrgcervantesNo ratings yet
- Banking On Governance, Insuring SustainabilityDocument258 pagesBanking On Governance, Insuring SustainabilityAhren CodyNo ratings yet
- Immigration Consulting AgreementDocument7 pagesImmigration Consulting AgreementDsmile EnterprisesNo ratings yet
- Risk Management Ch3Document33 pagesRisk Management Ch3Chucky ChungNo ratings yet
- Welcome Letter - 2023-24Document3 pagesWelcome Letter - 2023-24OlenaNo ratings yet
- Difference Types of Insurance Companies by Baqir SiddiqueDocument2 pagesDifference Types of Insurance Companies by Baqir Siddiquem.bqairNo ratings yet
- Cengage Advantage Books Fundamentals of Business Law Summarized Cases 9th Edition Roger Leroy Miller Solutions ManualDocument15 pagesCengage Advantage Books Fundamentals of Business Law Summarized Cases 9th Edition Roger Leroy Miller Solutions Manualwadeperlid9d98k100% (31)
- Life Contingencies II: ObjectivesDocument2 pagesLife Contingencies II: Objectivesdavid AbotsitseNo ratings yet
- Enriquez v. Sun Life AssuranceDocument3 pagesEnriquez v. Sun Life AssuranceMIKAELA THERESE OBACHNo ratings yet
- Saral Jeevan Bima Brochure-BRDocument10 pagesSaral Jeevan Bima Brochure-BRprabuNo ratings yet