You might also like
- Disaster Dollars: Financial Preparation and Recovery for Towns, Businesses, Farms, and IndividualsFrom EverandDisaster Dollars: Financial Preparation and Recovery for Towns, Businesses, Farms, and IndividualsNo ratings yet
- Series 65 Exam Practice Question Workbook: 700+ Comprehensive Practice Questions (2023 Edition)From EverandSeries 65 Exam Practice Question Workbook: 700+ Comprehensive Practice Questions (2023 Edition)No ratings yet
- HDFC ERGO General Insurance Company LimitedDocument6 pagesHDFC ERGO General Insurance Company LimitedShibani DesaiNo ratings yet
- Vipul Corp Lnsurance TPA PVT LTD.: Details of Primary InsuredDocument8 pagesVipul Corp Lnsurance TPA PVT LTD.: Details of Primary InsuredHimansh ChandakNo ratings yet
- Claim Form 10 - EditableDocument9 pagesClaim Form 10 - EditableharshiNo ratings yet
- E Claim FormDocument8 pagesE Claim FormronNo ratings yet
- Heartbeat Claim Form PDFDocument16 pagesHeartbeat Claim Form PDFAnkitThakkarNo ratings yet
- Max Bupa Claims FormDocument16 pagesMax Bupa Claims FormraviNo ratings yet
- Heartbeat Claim FormDocument8 pagesHeartbeat Claim Formto.animeshsen604No ratings yet
- CLAIM FORM FOR HEALTH INSURANCE POLICYDocument6 pagesCLAIM FORM FOR HEALTH INSURANCE POLICYSudipta DeNo ratings yet
- Claim Form for Health InsuranceDocument7 pagesClaim Form for Health InsuranceSwapnil NageNo ratings yet
- Claim FormDocument3 pagesClaim FormVediappan Alies RajaNo ratings yet
- Reimbursement Claim FormDocument7 pagesReimbursement Claim FormashishladooNo ratings yet
- Vipul Corp Lnsurance TPA PVT LTD.: Details of Insurance HistoryDocument7 pagesVipul Corp Lnsurance TPA PVT LTD.: Details of Insurance HistoryChatterjee KushalNo ratings yet
- Claims FormDocument16 pagesClaims FormPhunsukh WangduNo ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance PolicyDocument6 pagesClaim Form - Part A' To 'Claim Form For Health Insurance Policyanil sangwanNo ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance PolicyDocument6 pagesClaim Form - Part A' To 'Claim Form For Health Insurance PolicyMruthunjaya Reddy LakkamNo ratings yet
- Claim FormDocument6 pagesClaim Formashu9649No ratings yet
- VMPL - Claim Form (A)Document3 pagesVMPL - Claim Form (A)Rahul RathodNo ratings yet
- HDFC ERGO General Insurance Company Limited: Claim Form - Part ADocument4 pagesHDFC ERGO General Insurance Company Limited: Claim Form - Part Avizag mdindiaNo ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance PolicyDocument6 pagesClaim Form - Part A' To 'Claim Form For Health Insurance PolicypawanNo ratings yet
- Vipul Corp TPA PVT LTD.: Details of Insurance HistoryDocument6 pagesVipul Corp TPA PVT LTD.: Details of Insurance HistorybrajendraNo ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance PolicyDocument6 pagesClaim Form - Part A' To 'Claim Form For Health Insurance PolicyArunsNo ratings yet
- CLAIM FORM - PART ADocument7 pagesCLAIM FORM - PART AMayuresh DalviNo ratings yet
- Claim Form PDFDocument5 pagesClaim Form PDFmeghaNo ratings yet
- HDFC ERGO General Insurance Company Limited: Claim Form - Part ADocument7 pagesHDFC ERGO General Insurance Company Limited: Claim Form - Part Aharsh SharmaNo ratings yet
- Reimbursement CLaim Form IRDADocument5 pagesReimbursement CLaim Form IRDADhaval ThakkarNo ratings yet
- Claim Form - Part A: To Be Filled in by The InsuredDocument2 pagesClaim Form - Part A: To Be Filled in by The InsuredAli ArsalaanNo ratings yet
- HDFC ERGO General Insurance Claim FormDocument5 pagesHDFC ERGO General Insurance Claim FormMOHNISH MANCHALWARNo ratings yet
- ClaimFormDocument6 pagesClaimFormKanhaiya Lal SahuNo ratings yet
- Reimbursement Claim FormDocument2 pagesReimbursement Claim FormOmpalNo ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance PolicyDocument6 pagesClaim Form - Part A' To 'Claim Form For Health Insurance PolicyshuvanNo ratings yet
- Reimbursement Claim FormDocument4 pagesReimbursement Claim FormhariharanccetNo ratings yet
- HDFC Group Health Insurance - Claim ManualDocument6 pagesHDFC Group Health Insurance - Claim ManualNeir KrNo ratings yet
- CLAIM FORM - PART ADocument5 pagesCLAIM FORM - PART ARummy RajaNo ratings yet
- Claim Form - Group Health InsuranceDocument5 pagesClaim Form - Group Health Insurancevizag mdindiaNo ratings yet
- Health Insurance - Claim Form - Part A (To Be Filled by Insured)Document4 pagesHealth Insurance - Claim Form - Part A (To Be Filled by Insured)Shaikh AyyubNo ratings yet
- Health Assurance Claim FormDocument8 pagesHealth Assurance Claim FormHarmeet MaanNo ratings yet
- Health Insurance Claim FormDocument4 pagesHealth Insurance Claim Formaditya TestNo ratings yet
- Claim Form Part ADocument4 pagesClaim Form Part Ajeparal482No ratings yet
- Aditya Birla Claim Form Part ADocument8 pagesAditya Birla Claim Form Part Astatus addaNo ratings yet
- HDFC ERGO General Insurance Claim FormDocument8 pagesHDFC ERGO General Insurance Claim FormYash ChaudharyNo ratings yet
- Claim Form - HospitalizationDocument8 pagesClaim Form - HospitalizationNishantShah100% (1)
- Myhealth-Suraksha-Claim-Form (1) - RemovedDocument2 pagesMyhealth-Suraksha-Claim-Form (1) - Removedaditya727No ratings yet
- Myhealth Suraksha Claim FormDocument5 pagesMyhealth Suraksha Claim Formaditya727No ratings yet
- Care (Health Insurance Product) Claim FormDocument11 pagesCare (Health Insurance Product) Claim FormanshoeNo ratings yet
- Claim Form: Claim Form Part A Section A - Details of Primary InsuredDocument8 pagesClaim Form: Claim Form Part A Section A - Details of Primary InsuredAnonymous d8d8k1LiyNo ratings yet
- To Be Filled in by The Insured: Details of Primary InsuredDocument4 pagesTo Be Filled in by The Insured: Details of Primary Insurednaveen pointNo ratings yet
- Claim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part ADocument7 pagesClaim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part Aharmeet singhNo ratings yet
- ProHealth V7 ClaimFormA April23Document7 pagesProHealth V7 ClaimFormA April23njthakkarNo ratings yet
- Group Health - Claim FormDocument6 pagesGroup Health - Claim FormSubhash SharmaNo ratings yet
- ReimbursementFormA B2016 PDFDocument5 pagesReimbursementFormA B2016 PDFranganathNo ratings yet
- Care Health Claim FormDocument4 pagesCare Health Claim Formkishor_more47No ratings yet
- Claim Reimbursement FormDocument7 pagesClaim Reimbursement FormBagavathi RNo ratings yet
- Easy Ways To Speed Up The Claims Process: Manipalcigna Prohealth Insurance Policy Claim Form ADocument6 pagesEasy Ways To Speed Up The Claims Process: Manipalcigna Prohealth Insurance Policy Claim Form ARamesh WalkeNo ratings yet
- 05-01-2022 - Manuj Om HospitalisationDocument20 pages05-01-2022 - Manuj Om HospitalisationManuj RathoreNo ratings yet
- Claim Form - Part A General InsuranceDocument3 pagesClaim Form - Part A General Insurancejignesh vyasNo ratings yet
- Florida Real Estate Exam Prep: Everything You Need to Know to PassFrom EverandFlorida Real Estate Exam Prep: Everything You Need to Know to PassNo ratings yet
- Iran-United States Claims Arbitration: Debates on Commercial and Public International LawFrom EverandIran-United States Claims Arbitration: Debates on Commercial and Public International LawNo ratings yet
- EDocument315 pagesEALIA ZAFIRAHNo ratings yet
- GE Panda Ires Warmer Operation and Maintenance ManualDocument90 pagesGE Panda Ires Warmer Operation and Maintenance Manualiman hilmanNo ratings yet
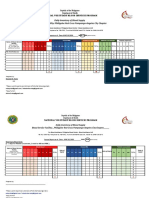
- Daily Inventory of Blood Supply Blood Service Facility: Philippine Red Cross Pampanga-Angeles City ChapterDocument2 pagesDaily Inventory of Blood Supply Blood Service Facility: Philippine Red Cross Pampanga-Angeles City ChapterFrances DeiNo ratings yet
- Instillation of Eye MedicationDocument2 pagesInstillation of Eye MedicationissaiahnicolleNo ratings yet
- JURNAL Penelitian TB ParuDocument6 pagesJURNAL Penelitian TB ParuCarseen Jilly Leo EvlistNo ratings yet
- RTMC 2008-Registration SessionsDocument4 pagesRTMC 2008-Registration SessionsAamir HamaadNo ratings yet
- Gongsun Sp-4: Grandfather GrandsonDocument2 pagesGongsun Sp-4: Grandfather Grandsonray72roNo ratings yet
- List of Allianz Efu Network (Panel) Hospitals: Hospital Wise S. No Province City Hospital Name Address Contact NoDocument5 pagesList of Allianz Efu Network (Panel) Hospitals: Hospital Wise S. No Province City Hospital Name Address Contact Nozeeshan shoukat50% (2)
- Gambaran Klinis Dan Laboratorium Pada Pasien Pneumonia Di Icu Rsud Raden Mattaher JambiDocument7 pagesGambaran Klinis Dan Laboratorium Pada Pasien Pneumonia Di Icu Rsud Raden Mattaher JambigusdeNo ratings yet
- Carrying and Transporting An Injured PersonDocument29 pagesCarrying and Transporting An Injured PersonAiza Rhea SantosNo ratings yet
- Edhi Foundation: M. Qasim Butt Babar Saadat C.J. Danyaal Bin RazaDocument20 pagesEdhi Foundation: M. Qasim Butt Babar Saadat C.J. Danyaal Bin RazaSyed ArslanNo ratings yet
- JUWAK - Jassim - Deliverables#2 CONT.Document3 pagesJUWAK - Jassim - Deliverables#2 CONT.Jassim JuwakNo ratings yet
- Implant Driver Compatibility-ChartDocument1 pageImplant Driver Compatibility-ChartBo WangNo ratings yet
- Continuous Versus IntermittentDocument15 pagesContinuous Versus Intermittentطارق الوادعيNo ratings yet
- NCM 104 Home VisitDocument10 pagesNCM 104 Home VisitPinsoy, Bruce riano e.No ratings yet
- RLE 40 ChecklistDocument3 pagesRLE 40 ChecklistJenny Turado ArbitrarioNo ratings yet
- Numerical Solution of SIRS Model for Dengue Fever TransmissionDocument12 pagesNumerical Solution of SIRS Model for Dengue Fever TransmissionRohan sharmaNo ratings yet
- Audit of Dispensary Near Misses in CommuDocument2 pagesAudit of Dispensary Near Misses in CommuKeymah HassanNo ratings yet
- Manual Blood Processing and Storage Sets: Description No. QtyDocument1 pageManual Blood Processing and Storage Sets: Description No. QtyCampaign MediaNo ratings yet
- Al Amin SarkerDocument2 pagesAl Amin SarkerRazib KhanNo ratings yet
- PBSC AllDocument2 pagesPBSC Allkuruvagadda sagarNo ratings yet
- Mindray PM 8000 Express User ID10229Document324 pagesMindray PM 8000 Express User ID10229Salmon 123No ratings yet
- Notification District Health Society Chittoor MO ANM Pharmacist PostsDocument8 pagesNotification District Health Society Chittoor MO ANM Pharmacist PostsRohitRajakNo ratings yet
- The Behavioral Inattention Test For Unilateral Visual NeglectDocument7 pagesThe Behavioral Inattention Test For Unilateral Visual NeglectDharmik PrajapatiNo ratings yet
- Severe Acute Respiratory Syndrome Coronavirus 2 (Sars Cov 2Document16 pagesSevere Acute Respiratory Syndrome Coronavirus 2 (Sars Cov 2Renea Joy ArruejoNo ratings yet
- Beckman Coulter PK TP Feb2012Document16 pagesBeckman Coulter PK TP Feb2012Inês LoboNo ratings yet
- Manuskrip Raihan Alfisahrin SarfanDocument10 pagesManuskrip Raihan Alfisahrin Sarfansarfanraihan27No ratings yet
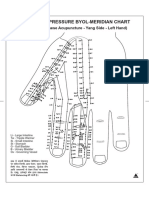
- Byol Maridian ChartDocument2 pagesByol Maridian ChartPranicHealingCentre63% (8)
- 11 NCP Pressure UlcerDocument6 pages11 NCP Pressure UlcerICa MarlinaNo ratings yet
- Color Therapy by Lacramioara BledeaDocument7 pagesColor Therapy by Lacramioara BledeaLily BledeaNo ratings yet