You might also like
- Acute Appendicitis: Causes, Symptoms and TreatmentDocument46 pagesAcute Appendicitis: Causes, Symptoms and TreatmentRAJAT DUGGALNo ratings yet
- Obstractive SymptomDocument43 pagesObstractive Symptomfairuz saadahNo ratings yet
- Imaging in Child Intussusception 2013: AuthorDocument33 pagesImaging in Child Intussusception 2013: AuthorartooktaviantoNo ratings yet
- IntussusceptionDocument10 pagesIntussusceptionshenlie100% (1)
- Chapter X.4. Intussusception: Case Based Pediatrics For Medical Students and ResidentsDocument5 pagesChapter X.4. Intussusception: Case Based Pediatrics For Medical Students and ResidentsNawaf Rahi AlshammariNo ratings yet
- Congenital Hypertrpphic Pyloric StenosisDocument30 pagesCongenital Hypertrpphic Pyloric StenosisParul VarshneyNo ratings yet
- Intestinal ObstructionDocument9 pagesIntestinal ObstructionMuhammad Fuad Jaafar100% (1)
- Acute AppendicitisDocument5 pagesAcute AppendicitisPrasetya Ismail PermadiNo ratings yet
- Appendix Part 1Document8 pagesAppendix Part 1Abdullah EssaNo ratings yet
- IntussusceptionDocument10 pagesIntussusceptionhya2284No ratings yet
- Jurnal THTDocument46 pagesJurnal THTShida ZakariaNo ratings yet
- Paralytic Ileus Complication of Acute Appendicitis Dudley, M.DDocument6 pagesParalytic Ileus Complication of Acute Appendicitis Dudley, M.Dandre nicholasNo ratings yet
- APENDICITIS Fischers Mastery of Surgery 7th ING PDFDocument33 pagesAPENDICITIS Fischers Mastery of Surgery 7th ING PDFMichel RamirezNo ratings yet
- 2 Semester 1 Major Patho AnatoDocument49 pages2 Semester 1 Major Patho AnatoManushi HenadeeraNo ratings yet
- Acute AppendicitisDocument30 pagesAcute AppendicitisJohn RyanNo ratings yet
- Intussusception PresentationDocument9 pagesIntussusception PresentationAme NasokiaNo ratings yet
- California State of Medicine III, No. THE Surgical Treatment Chro-NIC Tonsillitis.Document2 pagesCalifornia State of Medicine III, No. THE Surgical Treatment Chro-NIC Tonsillitis.Hendra SquidsartNo ratings yet
- APPENDICITISDocument37 pagesAPPENDICITISjohn paul richard mindanaoNo ratings yet
- IntussusceptionDocument4 pagesIntussusceptionBlue TechNo ratings yet
- Case Study Appendicitis: Gian Carlo P. Hijosa BSN 3Y1-10 Ms. Catherine J. CabreraDocument10 pagesCase Study Appendicitis: Gian Carlo P. Hijosa BSN 3Y1-10 Ms. Catherine J. CabreraGiannie Carlonnie HijosaNo ratings yet
- Sabitson - Appendiks EngDocument17 pagesSabitson - Appendiks Engzeek powerNo ratings yet
- Management Acute General Peritonitis: THE OFDocument6 pagesManagement Acute General Peritonitis: THE OFNadia Puspita DewiNo ratings yet
- Posterior Perforation of Gastric Ulcer-A Rare Surgical EmergencyDocument7 pagesPosterior Perforation of Gastric Ulcer-A Rare Surgical EmergencyyourinmyheartNo ratings yet
- HerniaDocument11 pagesHerniaHapsari Wibawani 'winda'100% (1)
- Soleimani 2007Document9 pagesSoleimani 2007ceciliaNo ratings yet
- Appendicitis - PeritonitisDocument37 pagesAppendicitis - PeritonitisanisamayaNo ratings yet
- 07 Intussusception and Midgut Volvulus - 2015-05-12 - AHC Media: Continuing Medical Education PublishingDocument10 pages07 Intussusception and Midgut Volvulus - 2015-05-12 - AHC Media: Continuing Medical Education PublishingPridina SyadirahNo ratings yet
- Vermiform AppendixDocument4 pagesVermiform AppendixHarun NasutionNo ratings yet
- Appendicitis Is A Condition Characterized by Inflammation of The Appendix. It Is Classified As A MedicalDocument5 pagesAppendicitis Is A Condition Characterized by Inflammation of The Appendix. It Is Classified As A Medicalbhe_jewelNo ratings yet
- IntussusceptionDocument60 pagesIntussusceptionAhmad Abu KushNo ratings yet
- Acquiredintestinalileus 131003164413 Phpapp01Document53 pagesAcquiredintestinalileus 131003164413 Phpapp01fandiroziNo ratings yet
- Bowel Obstruction and Tumors SheetDocument19 pagesBowel Obstruction and Tumors SheetAbu Ibtihal OsmanNo ratings yet
- Capitol University College of Nursing: Acute AppendicitisDocument28 pagesCapitol University College of Nursing: Acute AppendicitisCatherine Milar DescallarNo ratings yet
- MiniOSCE Surgery 1Document329 pagesMiniOSCE Surgery 1Mohammad BanisalmanNo ratings yet
- Visayas Community Medical Center Department of Surgery: Curan, Jan Kleen Ediza, Janseen Tortugo, Andrea MarieDocument43 pagesVisayas Community Medical Center Department of Surgery: Curan, Jan Kleen Ediza, Janseen Tortugo, Andrea MarieJanseen EdizaNo ratings yet
- Postgrad Med J 2005 Yalamarthi 174 7Document5 pagesPostgrad Med J 2005 Yalamarthi 174 7Novendi RizkaNo ratings yet
- Appendicitis.: The Function of The Appendix THE Origin ofDocument3 pagesAppendicitis.: The Function of The Appendix THE Origin ofSuresh IndiaNo ratings yet
- لقطة شاشة 2022-04-21 في 11.10.40 صDocument55 pagesلقطة شاشة 2022-04-21 في 11.10.40 صEngi KazangyNo ratings yet
- Hernia Examination SchemeDocument4 pagesHernia Examination Schemeatribecalledquest20No ratings yet
- Appendicitis: Differential Diagnoses & Workup Treatment & Medication Follow-UpDocument12 pagesAppendicitis: Differential Diagnoses & Workup Treatment & Medication Follow-UpnetonetinNo ratings yet
- Perforated Appendicitis Signs and ImagingDocument17 pagesPerforated Appendicitis Signs and ImagingEloisamay Barrameda EspirituNo ratings yet
- Assessment of AbdomenDocument3 pagesAssessment of AbdomenAhmed EzzatNo ratings yet
- Grabe Ka FinalDocument57 pagesGrabe Ka FinalJoanne Bernadette AguilarNo ratings yet
- [1]Hernia1-InguinalDocument7 pages[1]Hernia1-InguinalmunafalmahdiNo ratings yet
- IntussusceptionDocument3 pagesIntussusceptionHasan MohammedNo ratings yet
- Small Bowel: Alaa MaaliDocument78 pagesSmall Bowel: Alaa MaaliHalima AssiNo ratings yet
- Defecte Abdominale NNDocument56 pagesDefecte Abdominale NNDiana CostanNo ratings yet
- Appendicitis: Mark W. Jones Hassam Zulfiqar Jeffrey G. DeppenDocument7 pagesAppendicitis: Mark W. Jones Hassam Zulfiqar Jeffrey G. DeppenAndi HairunNo ratings yet
- 18-Month-Old Boy With Abdominal Pain and Rectal Bleeding BackgroundDocument5 pages18-Month-Old Boy With Abdominal Pain and Rectal Bleeding Backgroundcamille nina jane navarroNo ratings yet
- XXXDocument68 pagesXXXUcup SeniorNo ratings yet
- Pediatric Radiology ShortDocument95 pagesPediatric Radiology ShortNelly ChinelliNo ratings yet
- Melissa Kennedy, Chris A. LiacourasDocument3 pagesMelissa Kennedy, Chris A. LiacourasChristian LoyolaNo ratings yet
- Emptying: Gastro-Jejunostomy CoveringDocument1 pageEmptying: Gastro-Jejunostomy CoveringselviNo ratings yet
- Dr. Pankaj Kumar Assistant Professor Surgical GastroenterologyDocument39 pagesDr. Pankaj Kumar Assistant Professor Surgical GastroenterologyIlham Suryo Wibowo AntonoNo ratings yet
- IntussusceptionDocument24 pagesIntussusceptionOjambo Flavia100% (1)
- Diverticular DiseaseDocument8 pagesDiverticular DiseaseaizatamlikhaNo ratings yet
- AppendicitisDocument4 pagesAppendicitisFebriyana SalehNo ratings yet
- The Anatomy and Diagnosis of AppendicitisDocument11 pagesThe Anatomy and Diagnosis of AppendicitisAnjung WibiksanaNo ratings yet
- Intussusception - Practice Essentials, Background, Etiology and PathophysiologyDocument10 pagesIntussusception - Practice Essentials, Background, Etiology and PathophysiologyfkNo ratings yet
- Refinery Project ProposalDocument47 pagesRefinery Project ProposalAlhikmal MardiansahNo ratings yet
- An Unusual Perforated Appendicitis in Total Situs Inversus in Indonesia - A Case ReportDocument4 pagesAn Unusual Perforated Appendicitis in Total Situs Inversus in Indonesia - A Case Reportalifa ishmahdinaNo ratings yet
- 5794 22276 2 PBDocument4 pages5794 22276 2 PBalifa ishmahdinaNo ratings yet
- Molecular Properties That Influence The Oral Bioavailability of Drug CandidatesDocument10 pagesMolecular Properties That Influence The Oral Bioavailability of Drug Candidatesalifa ishmahdinaNo ratings yet
- Molecular Properties That Influence The Oral Bioavailability of Drug CandidatesDocument10 pagesMolecular Properties That Influence The Oral Bioavailability of Drug Candidatesalifa ishmahdinaNo ratings yet
- Assessment Cover Sheet: BSB52415 Diploma of Marketing and Communication Student NameDocument11 pagesAssessment Cover Sheet: BSB52415 Diploma of Marketing and Communication Student NameChun Jiang0% (1)
- Exam Unit 1 Out and About 1º BachilleratoDocument5 pagesExam Unit 1 Out and About 1º Bachilleratolisikratis1980No ratings yet
- Cultures of Learning: Language Classrooms in China: Martin Cortazzi Lixian JinDocument54 pagesCultures of Learning: Language Classrooms in China: Martin Cortazzi Lixian JinyhoulhandhariNo ratings yet
- ANNEX III-Site Components Drawings SetDocument96 pagesANNEX III-Site Components Drawings SetDenice Erika ManzanoNo ratings yet
- Pediatrics Study ScheduleDocument2 pagesPediatrics Study ScheduleNatnaelNo ratings yet
- Project Name: Purchase Order Management Creation Date: 26 October 2021 Created By: Sofiyan PathanDocument2 pagesProject Name: Purchase Order Management Creation Date: 26 October 2021 Created By: Sofiyan PathanAtul PawarNo ratings yet
- Julia Henzler - Resume 2 27Document1 pageJulia Henzler - Resume 2 27api-491391730No ratings yet
- Boston Globe Article - Jonnie Williams & Frank O'DonnellDocument3 pagesBoston Globe Article - Jonnie Williams & Frank O'DonnellFuzzy PandaNo ratings yet
- Data Structures and Algorithms in Java ™: Sixth EditionDocument8 pagesData Structures and Algorithms in Java ™: Sixth EditionIván Bartulin Ortiz0% (1)
- The Korean MiracleDocument20 pagesThe Korean MiracleDivya GirishNo ratings yet
- The Control of Building Motion by Friction Dampers: Cedric MARSHDocument6 pagesThe Control of Building Motion by Friction Dampers: Cedric MARSHAlam Mohammad Parvez SaifiNo ratings yet
- BCG ReportDocument9 pagesBCG Reportjlgjlj ljglkhNo ratings yet
- WMS INFINEON PROJECT TOWER (11Kv VCB INSTALLATION) - REV-1Document5 pagesWMS INFINEON PROJECT TOWER (11Kv VCB INSTALLATION) - REV-1tana100% (1)
- PDA Technical Documents on Sterilization ProcessesDocument3 pagesPDA Technical Documents on Sterilization ProcessesManas MishraNo ratings yet
- Fairfield Institute of Management & Technology E-Commerce: Lab/Practical File Subject Code: 112Document24 pagesFairfield Institute of Management & Technology E-Commerce: Lab/Practical File Subject Code: 112AYUSHNo ratings yet
- ADWEA Approved Vendor List - 18.4.2013Document297 pagesADWEA Approved Vendor List - 18.4.2013Anonymous kjvaeVJNNo ratings yet
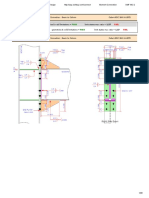
- Result Summary - Overall: Moment Connection - Beam To Column Code AISC 360-16 LRFDDocument29 pagesResult Summary - Overall: Moment Connection - Beam To Column Code AISC 360-16 LRFDYash Suthar100% (2)
- Training Programme EvaluationDocument14 pagesTraining Programme Evaluationthanhloan1902No ratings yet
- Top Answers to Mahout Interview QuestionsDocument6 pagesTop Answers to Mahout Interview QuestionsPappu KhanNo ratings yet
- Course Code Part Sem Paper Code Paper NameDocument3 pagesCourse Code Part Sem Paper Code Paper Nameshiv mishraNo ratings yet
- Research 10 Mod2Document28 pagesResearch 10 Mod2Fernadez RodisonNo ratings yet
- 02 Lightning Rods and AccessoriesDocument78 pages02 Lightning Rods and Accessoriesmoosuhaib100% (1)
- Computer Organization and Assembly Language: Lecture 1 - Basic ConceptsDocument13 pagesComputer Organization and Assembly Language: Lecture 1 - Basic ConceptsNosreffejDelRosarioNo ratings yet
- Kelley DavisDocument3 pagesKelley Davisapi-626701108No ratings yet
- ISO 13485 Version 2016 Requirements NotesDocument24 pagesISO 13485 Version 2016 Requirements Notesda_reaper_dasNo ratings yet
- Pizza Hut Final!Document15 pagesPizza Hut Final!Alisha ParabNo ratings yet
- I3rc Insights Pvt. Ltd. India - Company Credentials PDFDocument28 pagesI3rc Insights Pvt. Ltd. India - Company Credentials PDFManoj Kumar JhaNo ratings yet
- HORIZONTAL DISTRIBUTION OF FORCES - Part 1-2Document1 pageHORIZONTAL DISTRIBUTION OF FORCES - Part 1-2Inna PotesNo ratings yet
- PW 160-Taliban Fragmentation Fact Fiction and Future-PwDocument28 pagesPW 160-Taliban Fragmentation Fact Fiction and Future-Pwrickyricardo1922No ratings yet
- Challenges Faced by Irregular StudentsDocument13 pagesChallenges Faced by Irregular StudentsTicag Teo80% (5)












































![[1]Hernia1-Inguinal](https://imgv2-1-f.scribdassets.com/img/document/722138726/149x198/9e3ffe53d3/1712853076?v=1)