You might also like
- Establishing A State-of-the-Art Diagnostic and MedDocument6 pagesEstablishing A State-of-the-Art Diagnostic and Medmichellelmarylinda75No ratings yet
- Research For GramarianDocument66 pagesResearch For GramarianDelfhringerNo ratings yet
- Assessment of Health Care Workers Knowledge, Attitude and Practices of Radiation Safety at A Specialist Hospital, Jos, Plateau State, NigeriaDocument6 pagesAssessment of Health Care Workers Knowledge, Attitude and Practices of Radiation Safety at A Specialist Hospital, Jos, Plateau State, NigeriaEditor IJTSRDNo ratings yet
- Cuali Resonancia Magnetica 2023Document6 pagesCuali Resonancia Magnetica 2023Pa Bu GaNo ratings yet
- An Overview of Artificial Intelligence in Medical Physics and Radiation OncologyDocument11 pagesAn Overview of Artificial Intelligence in Medical Physics and Radiation Oncologyxiwevi4103No ratings yet
- Assessment of Patient's Waiting Time in The RadiologyDocument7 pagesAssessment of Patient's Waiting Time in The Radiologygreg_enricoNo ratings yet
- RCT - Scope - of - Practice - Diagnostic - Rad - 22 - May - 2020 - For Current - ScopeDocument5 pagesRCT - Scope - of - Practice - Diagnostic - Rad - 22 - May - 2020 - For Current - ScopeNolizwi NkosiNo ratings yet
- MJMHS 1004Document8 pagesMJMHS 1004Ayu RositaNo ratings yet
- English FinalsDocument28 pagesEnglish FinalsMark M. Alipio100% (1)
- 1 s2.0 S1078817419301518 MainDocument6 pages1 s2.0 S1078817419301518 MainMiro SpiroNo ratings yet
- Bridging The Gap: Understanding Medical Students and Interns Perceptions of Radiology As A Career Choice at Taif University, Saudi ArabiaDocument8 pagesBridging The Gap: Understanding Medical Students and Interns Perceptions of Radiology As A Career Choice at Taif University, Saudi ArabiaIJAR JOURNALNo ratings yet
- Bridging The Gap: Understanding Medical Students' and Interns'perceptions of Radiology As A Career Choice at Taif University, Saudi ArabiaDocument8 pagesBridging The Gap: Understanding Medical Students' and Interns'perceptions of Radiology As A Career Choice at Taif University, Saudi ArabiaIJAR JOURNALNo ratings yet
- CRC ClassificationDocument19 pagesCRC Classificationmehwishsardar0024No ratings yet
- Biomolecules 11 00090 v2Document4 pagesBiomolecules 11 00090 v2Windu KumaraNo ratings yet
- Discovering Associations Between Radiological Features and COVID 19 Patients' DeteriorationDocument8 pagesDiscovering Associations Between Radiological Features and COVID 19 Patients' Deteriorationkadoxe1682No ratings yet
- Oncology Nursing Trends and Issues 3Document7 pagesOncology Nursing Trends and Issues 3DaichiNo ratings yet
- Fonc 12 773840Document25 pagesFonc 12 773840azul2233No ratings yet
- Nuevo Resumen Diapositiva 1Document12 pagesNuevo Resumen Diapositiva 1HTHumanityNo ratings yet
- LUS PneumoniaDocument5 pagesLUS PneumoniaFitriana Kusuma WardhaniNo ratings yet
- Deep Convolutional Neural Networks in Thyroid Disease Detection-Full TextDocument10 pagesDeep Convolutional Neural Networks in Thyroid Disease Detection-Full TextJamesLeeNo ratings yet
- Medical Physics - 2021 - Andersson - Estimation of Patient Skin Dose in Fluoroscopy Summary of A Joint Report by AAPMDocument26 pagesMedical Physics - 2021 - Andersson - Estimation of Patient Skin Dose in Fluoroscopy Summary of A Joint Report by AAPMRoshi_11No ratings yet
- Chest X-Ray Outlier Detection Model Using Dimension Reduction and Edge DetectionDocument11 pagesChest X-Ray Outlier Detection Model Using Dimension Reduction and Edge DetectionHardik AgrawalNo ratings yet
- Chapt 1 PeterDocument63 pagesChapt 1 PeterSamson PeterNo ratings yet
- Identification and Analyzation of Covid-19 in Chest X-Rays A ReviewDocument8 pagesIdentification and Analyzation of Covid-19 in Chest X-Rays A ReviewIJRASETPublicationsNo ratings yet
- 6257155572d49 Nuclear Medicine - EditedDocument4 pages6257155572d49 Nuclear Medicine - EditedBandah Mwiti JosephNo ratings yet
- Medical Physics - 2021 - Andersson - Estimation of Patient Skin Dose in Fluoroscopy Summary of A Joint Report by AAPMDocument27 pagesMedical Physics - 2021 - Andersson - Estimation of Patient Skin Dose in Fluoroscopy Summary of A Joint Report by AAPMArwa ZagzoogNo ratings yet
- Journal Pone 0269931Document13 pagesJournal Pone 0269931Abdelali MoufidiNo ratings yet
- Title of The Paper: Student's Name University Course Professor DateDocument5 pagesTitle of The Paper: Student's Name University Course Professor DatebrianNo ratings yet
- 논문원문Document7 pages논문원문Donghee LeeNo ratings yet
- Quality Control of Diagnostic RadiologyDocument7 pagesQuality Control of Diagnostic RadiologySehad KadiriNo ratings yet
- Knowledge of Common Radiological Investigations in Emergency Setting by Physicians in BahrainDocument7 pagesKnowledge of Common Radiological Investigations in Emergency Setting by Physicians in BahrainIJAR JOURNALNo ratings yet
- Radiological Protection in The Perspective of HealthDocument4 pagesRadiological Protection in The Perspective of Healthhizwa harunNo ratings yet
- Sicotj S 24 00004Document35 pagesSicotj S 24 00004Mohammad Ahmad AyasrahNo ratings yet
- Quality Use of AI in Medical Imaging-What Do Radiologists Need To Know?Document8 pagesQuality Use of AI in Medical Imaging-What Do Radiologists Need To Know?SANDEEP REDDYNo ratings yet
- Rationale For Implementing Dose Reference Level As A Quality Assurance Tool in Medical Radiography in NigeriaDocument5 pagesRationale For Implementing Dose Reference Level As A Quality Assurance Tool in Medical Radiography in NigeriaInternational Organization of Scientific Research (IOSR)No ratings yet
- FRANCISSUWALIDocument14 pagesFRANCISSUWALIinno semuNo ratings yet
- Radiomics Breakthrough Could Spark The Head and Neck Cancer Radiotherapy RevolutionDocument9 pagesRadiomics Breakthrough Could Spark The Head and Neck Cancer Radiotherapy Revolutionmazda626 retrocarsNo ratings yet
- s12903 018 0476 8Document6 pagess12903 018 0476 8Gujapaneni Ravi KumarNo ratings yet
- Final ProjectDocument14 pagesFinal Projectapi-298975236No ratings yet
- On The Analyses of Medical Images Using Traditional Machine Learning Techniques and Convolutional Neural NetworksDocument61 pagesOn The Analyses of Medical Images Using Traditional Machine Learning Techniques and Convolutional Neural Networkstemp tempNo ratings yet
- An Assessment of Medical Students Proficiency RegDocument8 pagesAn Assessment of Medical Students Proficiency RegRudolph SunnydaysNo ratings yet
- Radiology Request Forms ResearchDocument8 pagesRadiology Request Forms Researchtruevine_ministryNo ratings yet
- Diagnosing Ventilator-Associated Pneumonia (Vap) in Uk Nhs Icus: The Perceived Value and Role of A Novel Optical TechnologyDocument11 pagesDiagnosing Ventilator-Associated Pneumonia (Vap) in Uk Nhs Icus: The Perceived Value and Role of A Novel Optical Technologycarmen rosa secce pedrazaNo ratings yet
- Health Science Reports - 2023 - Nabavizadeh - Prevalence of Body Dysmorphic Disorder in Rhinoplasty Candidates ADocument11 pagesHealth Science Reports - 2023 - Nabavizadeh - Prevalence of Body Dysmorphic Disorder in Rhinoplasty Candidates Ahans jablonskyNo ratings yet
- 8 Vol 73 No 1Document8 pages8 Vol 73 No 1fara latifaNo ratings yet
- Ijamscrjournal1, IJAMSCR-21-313 PDFDocument5 pagesIjamscrjournal1, IJAMSCR-21-313 PDFARUL CHOKKANNo ratings yet
- Advances in Ultrasound Imaging Techniques and Applications A Comprehensive ReviewDocument3 pagesAdvances in Ultrasound Imaging Techniques and Applications A Comprehensive ReviewTrésor NaraNo ratings yet
- The Role of Coronary Angiography in Diagnostic Precision and Clinical Outcomes of Coronary Artery DiseasesDocument42 pagesThe Role of Coronary Angiography in Diagnostic Precision and Clinical Outcomes of Coronary Artery DiseasesDebjit BanerjeeNo ratings yet
- Deep-Learning-Assisted Detection and SegmentationDocument8 pagesDeep-Learning-Assisted Detection and SegmentationKARANAM SANTOSHNo ratings yet
- Application of Deep Learning For Early Detection of Covid 19 Using CT Scan ImagesDocument8 pagesApplication of Deep Learning For Early Detection of Covid 19 Using CT Scan ImagesResearch ParkNo ratings yet
- Journal Pone 0281073Document14 pagesJournal Pone 0281073chest CSNo ratings yet
- Applsci 13 06582Document29 pagesApplsci 13 06582Marwa AlhajAhmadNo ratings yet
- PIIS2468045123000603Document10 pagesPIIS2468045123000603daniaNo ratings yet
- Assessing The Status of Professional Ethics Among Ghanaian RadiographersDocument31 pagesAssessing The Status of Professional Ethics Among Ghanaian Radiographersdeehans100% (2)
- Fsurg 09 1029991Document9 pagesFsurg 09 1029991Juanito AlojNo ratings yet
- Ultrasonography and Its Role in Clinical DiagnosisDocument5 pagesUltrasonography and Its Role in Clinical DiagnosisCentral Asian StudiesNo ratings yet
- Fdata 06 1120989Document27 pagesFdata 06 1120989smith.williamsNo ratings yet
- Deep Learning Techniques For Detection of COVID-19 Using Chest X-RaysDocument17 pagesDeep Learning Techniques For Detection of COVID-19 Using Chest X-RayspoojaNo ratings yet
- English Pp1Document2 pagesEnglish Pp1Kipkoech FrankNo ratings yet
- StrigaDocument12 pagesStrigaKipkoech FrankNo ratings yet
- Biology Paper 3 QueDocument7 pagesBiology Paper 3 QueKipkoech Frank100% (1)
- EnglishDocument13 pagesEnglishKipkoech FrankNo ratings yet
- Bomet County Integrated Development Plan 2018-2022Document259 pagesBomet County Integrated Development Plan 2018-2022Kipkoech FrankNo ratings yet
- 231/2 Biology Paper 2: Marking Scheme The Royal Exam SeriesDocument2 pages231/2 Biology Paper 2: Marking Scheme The Royal Exam SeriesKipkoech FrankNo ratings yet
- Class 6 April Homework-1Document22 pagesClass 6 April Homework-1Kipkoech FrankNo ratings yet
- Appointment Letter (Sample Copy) : DearDocument7 pagesAppointment Letter (Sample Copy) : DearKipkoech FrankNo ratings yet
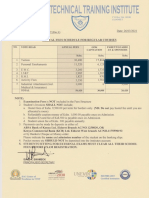
- Rvtti Fee StructureDocument1 pageRvtti Fee StructureKipkoech Frank43% (7)
- Interior SpaceDocument166 pagesInterior SpaceKipkoech FrankNo ratings yet
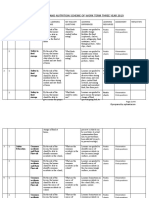
- GRADE 3 TERM 3 2020 ENGLISH LITERACY SCHEMES (MTP)Document4 pagesGRADE 3 TERM 3 2020 ENGLISH LITERACY SCHEMES (MTP)Kipkoech FrankNo ratings yet
- Research On Failure and Collapse of Buildings Final Report 31-10-2019Document82 pagesResearch On Failure and Collapse of Buildings Final Report 31-10-2019Kipkoech FrankNo ratings yet
- Grade 3 Term 3 Schemes of Work - HygieneDocument4 pagesGrade 3 Term 3 Schemes of Work - HygieneKipkoech FrankNo ratings yet
- Elimu Scholarship Application Form 22apr21Document6 pagesElimu Scholarship Application Form 22apr21Kipkoech FrankNo ratings yet
- 2022 Latest Stock List 2-28Document7 pages2022 Latest Stock List 2-28depghimNo ratings yet
- Dosis Radiasi Dari Tindakan Ct-Scan Kepala PDFDocument9 pagesDosis Radiasi Dari Tindakan Ct-Scan Kepala PDFVergeen OllshopNo ratings yet
- Xrays, MRI ActivitiesDocument2 pagesXrays, MRI Activitiessokhna.sall.545No ratings yet
- Proposal @2022Document45 pagesProposal @2022Kidima100% (2)
- Dexa Scan and Its Application: Sarbari Saha Asst Professor RadiologyDocument19 pagesDexa Scan and Its Application: Sarbari Saha Asst Professor Radiologykyuleen05No ratings yet
- Icrp 117Document102 pagesIcrp 117Sari BustillosNo ratings yet
- Resume 10-16-2017Document2 pagesResume 10-16-2017api-336793554No ratings yet
- Villa Arcovis 3000 C-Arm X-Ray System - User ManualDocument595 pagesVilla Arcovis 3000 C-Arm X-Ray System - User ManualLuis Fernando Garcia SNo ratings yet
- PGH MapDocument2 pagesPGH MapAlyssandra Luceno100% (1)
- Fanr Reg 04 V1 For WebsiteDocument11 pagesFanr Reg 04 V1 For WebsiteMitulsinh M RavaljiNo ratings yet
- History of Radiation & PhysicsDocument34 pagesHistory of Radiation & Physicssohaksa bashaNo ratings yet
- 00 Medical-Imaging-Preface-Waleed-AltalabiDocument5 pages00 Medical-Imaging-Preface-Waleed-Altalabiمحمدعبدالخالق العلوانيNo ratings yet
- Tomography Abdomen Dalam Kasus Tumor Abdomen: Jimed, Vol. 2, No. 1 Issn 2356-301XDocument5 pagesTomography Abdomen Dalam Kasus Tumor Abdomen: Jimed, Vol. 2, No. 1 Issn 2356-301Xbella arviantiNo ratings yet
- Typhon Group Case Log TotalsDocument3 pagesTyphon Group Case Log Totalsapi-574059920No ratings yet
- Documentazione Tubo A Raggi X Tube Documentation Documentation Du TubeDocument4 pagesDocumentazione Tubo A Raggi X Tube Documentation Documentation Du Tubecamq827No ratings yet
- Lab ResultDocument1 pageLab ResultDushyant HoodaNo ratings yet
- Xray Equipment GuidelinesDocument9 pagesXray Equipment Guidelines001bellaNo ratings yet
- Radiation Therapy ICRUDocument1 pageRadiation Therapy ICRUAlina RogojanuNo ratings yet
- Radiation Protection in Diagnostic and Interventional RadiologyDocument44 pagesRadiation Protection in Diagnostic and Interventional RadiologyPaul KennedyNo ratings yet
- Gamma Knife1Document17 pagesGamma Knife1api-247561652No ratings yet
- BrainDocument1 pageBrainDrehsan Memon100% (1)
- Netcare Medical Physicist1Document4 pagesNetcare Medical Physicist1api-250361062No ratings yet
- Radiation Safety Course Powerpoint PresentationDocument59 pagesRadiation Safety Course Powerpoint PresentationJayesh100% (1)
- To Whom It May ConcernDocument1 pageTo Whom It May Concerndrsanjeev15No ratings yet
- Radiation Safety Program: HDR Cobalt-60 and LDR Cesium-137 BRACHYTHERAPY FACILITYDocument38 pagesRadiation Safety Program: HDR Cobalt-60 and LDR Cesium-137 BRACHYTHERAPY FACILITYGregory CagampanNo ratings yet
- Independent Evaluation of Dose-Volume Histogram (DVH) Calculation AccuracyDocument1 pageIndependent Evaluation of Dose-Volume Histogram (DVH) Calculation AccuracyFitriyani MusNo ratings yet
- RT CT1 PPT L08 Computed Tomography BasicsDocument8 pagesRT CT1 PPT L08 Computed Tomography BasicsDebendra Dev KhanalNo ratings yet
- Malone - The Blue Book - Shielding Code of Practice in IrelandDocument36 pagesMalone - The Blue Book - Shielding Code of Practice in IrelandGeorgiana KokonaNo ratings yet
- Quality Control Circle - Desk File and WorkDocument26 pagesQuality Control Circle - Desk File and WorkZuhairi MohamedNo ratings yet
- Book Review Strategies For Radiation Therapy TreatDocument2 pagesBook Review Strategies For Radiation Therapy TreatArtist ArtistNo ratings yet
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (5)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (39)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 4 out of 5 stars4/5 (5)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 4.5 out of 5 stars4.5/5 (84)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeFrom EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeRating: 4.5 out of 5 stars4.5/5 (3)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (44)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (267)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (170)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- I Shouldn't Feel This Way: Name What’s Hard, Tame Your Guilt, and Transform Self-Sabotage into Brave ActionFrom EverandI Shouldn't Feel This Way: Name What’s Hard, Tame Your Guilt, and Transform Self-Sabotage into Brave ActionNo ratings yet
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (46)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (39)
- The Fun Habit: How the Pursuit of Joy and Wonder Can Change Your LifeFrom EverandThe Fun Habit: How the Pursuit of Joy and Wonder Can Change Your LifeRating: 4.5 out of 5 stars4.5/5 (19)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesFrom EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesRating: 4.5 out of 5 stars4.5/5 (1412)
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingFrom EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingRating: 4 out of 5 stars4/5 (1138)
- The Story of Philosophy: The Lives and Opinions of the Greater PhilosophersFrom EverandThe Story of Philosophy: The Lives and Opinions of the Greater PhilosophersNo ratings yet