You might also like
- DriversLicenceApplication in NSW in AustraliaDocument2 pagesDriversLicenceApplication in NSW in AustraliaVivi ViNo ratings yet
- Driver's Licence Application Form: Important - Ensure You Read This Information Before Completing The FormDocument2 pagesDriver's Licence Application Form: Important - Ensure You Read This Information Before Completing The Formminka646No ratings yet
- Application For Alaska Driver License, Permit or Identification CardDocument2 pagesApplication For Alaska Driver License, Permit or Identification CardGregNo ratings yet
- DL 1 PDocument2 pagesDL 1 Pdevejo0% (1)
- Heartland Jiffy Lube Application 10-01-09Document7 pagesHeartland Jiffy Lube Application 10-01-09forler98022No ratings yet
- Royal Caribbean Cruises Ltd. (RCL) Is An Equal Opportunity EmployerDocument3 pagesRoyal Caribbean Cruises Ltd. (RCL) Is An Equal Opportunity EmployerUziel Lopez LopezNo ratings yet
- F ASH O OSO: Application For Driver'S LicenseDocument2 pagesF ASH O OSO: Application For Driver'S LicensejoNo ratings yet
- Application For EmploymentDocument4 pagesApplication For EmploymentRudhi WahyudiNo ratings yet
- Job ApplicationDocument6 pagesJob ApplicationKizze' HarrisNo ratings yet
- Application For Drivers License or ADL Form From LTODocument2 pagesApplication For Drivers License or ADL Form From LTOJoselito Azarraga V100% (2)
- Dotc Lto Form 21Document2 pagesDotc Lto Form 21Pjhay PidlaoanNo ratings yet
- DL 1 PDocument2 pagesDL 1 PmerlindebergNo ratings yet
- Civil Cover Sheet ODY (08-2022)Document3 pagesCivil Cover Sheet ODY (08-2022)rsundar48No ratings yet
- I Application For Employment - ManagementDocument6 pagesI Application For Employment - ManagementkhoryeeherngNo ratings yet
- Licence or Learner Permit ApplicationDocument2 pagesLicence or Learner Permit ApplicationvfcaffNo ratings yet
- Application For Employment: Please Answer The Following QuestionsDocument2 pagesApplication For Employment: Please Answer The Following QuestionsJosipBatinovićNo ratings yet
- Lto Driver License Aplication Form BlankDocument1 pageLto Driver License Aplication Form BlankFerdz RanulloNo ratings yet
- Licence or Learner Permit ApplicationDocument2 pagesLicence or Learner Permit ApplicationChris ParkerNo ratings yet
- Laurel SFDocument3 pagesLaurel SFEllyn SantiagoNo ratings yet
- Application Form For Employment 2Document2 pagesApplication Form For Employment 2Fortunate KennyNo ratings yet
- Application For Employment - PT BCKDocument5 pagesApplication For Employment - PT BCKrizkyNo ratings yet
- C-121 CV FromDocument2 pagesC-121 CV FromaungkyawsintdpNo ratings yet
- Application For Student Driver'S Permit / Driver'S License / Conductor'S License (Apl)Document2 pagesApplication For Student Driver'S Permit / Driver'S License / Conductor'S License (Apl)Jerico Garcia100% (4)
- DFA Application Form For FSSO and FSSE ApplicantsDocument2 pagesDFA Application Form For FSSO and FSSE Applicantsp01zawjNo ratings yet
- Personal Detail: HRPD / Rec / 07Document4 pagesPersonal Detail: HRPD / Rec / 07idoy yodiNo ratings yet
- Kotak Proposal Form (KPF) : For Office Use OnlyDocument8 pagesKotak Proposal Form (KPF) : For Office Use OnlyMoolam RaoNo ratings yet
- Applicants Personal Data: Komplek Citypark Blok A4 Cengkareng TimurDocument4 pagesApplicants Personal Data: Komplek Citypark Blok A4 Cengkareng TimurstevendamaiNo ratings yet
- Application Form IPOH Sales & Service 2022Document4 pagesApplication Form IPOH Sales & Service 2022Muhammad Akmal RazmiNo ratings yet
- Employment Application: Eva Airways CorporationDocument7 pagesEmployment Application: Eva Airways CorporationbibikhaikhoiNo ratings yet
- Form DPP Suzuki RevDocument4 pagesForm DPP Suzuki RevarryarryNo ratings yet
- Aac Application TritonDocument3 pagesAac Application TritonRazvan BuleteNo ratings yet
- TMP Tech Application FormDocument2 pagesTMP Tech Application Formje_carD23No ratings yet
- DFA Application Form Revision 02Document2 pagesDFA Application Form Revision 02ynah manaloiNo ratings yet
- Blank Job Application Form Application Form 10192018231845Document2 pagesBlank Job Application Form Application Form 10192018231845Damonta HenryNo ratings yet
- Am S ApplicationformDocument5 pagesAm S ApplicationformDivay BakshiNo ratings yet
- Cv/Application Form: GIVE FULL DETAILS (University or Equivalent)Document6 pagesCv/Application Form: GIVE FULL DETAILS (University or Equivalent)Nijo JosephNo ratings yet
- Driver'S License and Identification Card Application: Yes, I Would Like To Become An Organ, Eye and Tissue DonorDocument2 pagesDriver'S License and Identification Card Application: Yes, I Would Like To Become An Organ, Eye and Tissue DonorWintersNNo ratings yet
- Special Request/Authorization: For Official Use Only Privacy SensitiveDocument1 pageSpecial Request/Authorization: For Official Use Only Privacy SensitiveRaymondSanchezNo ratings yet
- O o o o o o o o o o O: Application For Permit, Driver License or Non-Driver Id CardDocument3 pagesO o o o o o o o o o O: Application For Permit, Driver License or Non-Driver Id CardGHNo ratings yet
- MV 44Document3 pagesMV 44strangequark87No ratings yet
- JCF Application FormDocument9 pagesJCF Application FormDray Day67% (9)
- Criminal Complaint Against Brandon BostianDocument9 pagesCriminal Complaint Against Brandon BostianAnna OrsoNo ratings yet
- Application For Driver'S License: ROM MA K-JoviDocument2 pagesApplication For Driver'S License: ROM MA K-JoviMark Jovin RomNo ratings yet
- L ELA ALA ERA: Application For Driver'S LicenseDocument2 pagesL ELA ALA ERA: Application For Driver'S LicenseDon Facundo BiryaniNo ratings yet
- Insur. AppDocument8 pagesInsur. Appswarna sNo ratings yet
- Asialink Loan Application v7 FillableDocument2 pagesAsialink Loan Application v7 FillableJovelyn MarimonNo ratings yet
- Employment Application: San Francisco Housing AuthorityDocument5 pagesEmployment Application: San Francisco Housing AuthoritySIDED1No ratings yet
- PNSC ApplicationFormDocument5 pagesPNSC ApplicationFormalbaraka.shippingNo ratings yet
- Chellship Application FormDocument6 pagesChellship Application FormvinithNo ratings yet
- Form 2 (See Rules 10, 14, 17 and 18)Document16 pagesForm 2 (See Rules 10, 14, 17 and 18)Nikhil G MenonNo ratings yet
- EDC Application Form EM 042Document2 pagesEDC Application Form EM 042Armie May RicoNo ratings yet
- Employee Application Form - Actual SynergyDocument2 pagesEmployee Application Form - Actual SynergyPatrico Rillah SetiawanNo ratings yet
- DL 180Document2 pagesDL 180Joe DonahueNo ratings yet
- Admissions Application Form RevisedDocument6 pagesAdmissions Application Form Revisedsafadastgir31No ratings yet
- Saeed and Mohamed Al Naboodah Group: Paste (1) PhotographDocument3 pagesSaeed and Mohamed Al Naboodah Group: Paste (1) PhotographprakashvkarunNo ratings yet
- Saps Preliminary Trainee Application Form (2019/2020)Document1 pageSaps Preliminary Trainee Application Form (2019/2020)Fortune SotsuNo ratings yet
- Quezon CityDocument73 pagesQuezon CityDAGOHOY4200% (1)
- Railway Corrosion and Stray Currents TTGN3Document16 pagesRailway Corrosion and Stray Currents TTGN3manualvazNo ratings yet
- Preliminary Design Report (Group 5)Document10 pagesPreliminary Design Report (Group 5)Shubhankit MohanNo ratings yet
- Yale-ShawBox All Products-YLT-L1001Document2 pagesYale-ShawBox All Products-YLT-L1001Mahmoud AllamNo ratings yet
- BOI Northern Investment in Sri LankaDocument46 pagesBOI Northern Investment in Sri LankaBalachandran NavaratnasamyNo ratings yet
- Factors Affecting Pavement Design PDFDocument2 pagesFactors Affecting Pavement Design PDFKris33% (3)
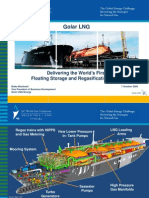
- Golar LNGDocument28 pagesGolar LNGrajee7100% (2)
- EWM Transaction CodesDocument22 pagesEWM Transaction CodesChuks Osagwu100% (1)
- 2007Document418 pages2007RaduoesNo ratings yet
- CAP 3400 Air Operator Certification Manual (Helicopters)Document238 pagesCAP 3400 Air Operator Certification Manual (Helicopters)Saragh BhandaryNo ratings yet
- 13 Characteristics of An Air Traffic ControllerDocument2 pages13 Characteristics of An Air Traffic ControllerWayne FarleyNo ratings yet
- Using Drone: Ils / Vor / PapiDocument28 pagesUsing Drone: Ils / Vor / Papifika puteraNo ratings yet
- PC4000 11 A4 InternetDocument9 pagesPC4000 11 A4 InternetvitaliyNo ratings yet
- Air & Sea TravelDocument8 pagesAir & Sea TravelKhổng Tuyết NhiNo ratings yet
- Curriculum Vitae: A.Sahaya LeninDocument5 pagesCurriculum Vitae: A.Sahaya LeninMuhammed ThanzeelNo ratings yet
- Transport - Lifting Instructions (Crane)Document1 pageTransport - Lifting Instructions (Crane)Agung WitonoNo ratings yet
- Insurance Claim Procedure For Damage or Loss of MaterialDocument2 pagesInsurance Claim Procedure For Damage or Loss of MaterialAMIT GUPTANo ratings yet
- Torts Full Text Cases For ThursdayDocument102 pagesTorts Full Text Cases For ThursdayPaulo BurroNo ratings yet
- Fuel ContaminationDocument2 pagesFuel ContaminationFranco PugaNo ratings yet
- Top 7 Types of River Training WorksDocument13 pagesTop 7 Types of River Training WorksRanvier SinghNo ratings yet
- Calibraciones ChryslerDocument497 pagesCalibraciones ChryslerEd Klb100% (6)
- Konakn Railway VisitDocument12 pagesKonakn Railway Visit4MT17ME160 VIGHNESHNo ratings yet
- Collocations 2Document3 pagesCollocations 2tngdtNo ratings yet
- 3RD Moot ProbDocument8 pages3RD Moot ProbSIMRAN PRADHANNo ratings yet
- nanni-ProductGuide enDocument76 pagesnanni-ProductGuide enmakNo ratings yet
- Circular WeavingDocument28 pagesCircular Weavinggovardhan6rao50% (2)
- c175 Cat 2825kva - EdgDocument13 pagesc175 Cat 2825kva - EdgAmir Asyraf SuhailiNo ratings yet
- BSBEdge Report PDFDocument165 pagesBSBEdge Report PDFMITHUN KUMAR BEHERANo ratings yet
- Funda TSD ShortCutDocument12 pagesFunda TSD ShortCutAmitShukla100% (1)
- User Manual-28040020402ADocument172 pagesUser Manual-28040020402Atosve33% (3)