Professional Documents
Culture Documents
2007 Time To Treatment in Primary Percutaneous
Uploaded by
Alma EscobarOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
2007 Time To Treatment in Primary Percutaneous
Uploaded by
Alma EscobarCopyright:
Available Formats
The n e w e ng l a n d j o u r na l of m e dic i n e
Review article
Current Concepts
Time to Treatment in Primary Percutaneous
Coronary Intervention
Brahmajee K. Nallamothu, M.D., M.P.H., Elizabeth H. Bradley, Ph.D.,
and Harlan M. Krumholz, M.D., S.M.
E
arly administration of reperfusion therapy improves survival From the Health Services Research and
in patients with ST-elevation myocardial infarction by reestablishing coronary Development Center of Excellence, Ann
Arbor Veterans Affairs Medical Center, and
blood flow within the occluded infarct-related artery.1 Primary percutaneous the Department of Internal Medicine, Di-
coronary intervention (PCI) is superior to fibrinolytic therapy when performed rap- vision of Cardiovascular Disease, Univer-
idly by expert teams,2 but its effectiveness may be limited by delays in delivery.3 sity of Michigan Medical School — both
in Ann Arbor (B.K.N.); the Section of
Recent national efforts are drawing attention to the importance of door-to-balloon Health Policy and Administration, Depart-
time as a key indicator of quality of care for patients with ST-elevation myocardial ment of Epidemiology and Public Health
infarction who are treated with primary PCI.4 The American College of Cardiology and the Robert Wood Johnson Clinical
Scholars Program, Department of Medi-
(ACC), in collaboration with the American Heart Association (AHA), the American cine, Yale University School of Medicine,
College of Emergency Physicians (ACEP), the National Heart, Lung, and Blood Institute New Haven, CT (E.H.B., H.M.K.); and
(NHLBI), and other partners, has implemented a national quality-improvement cam- the Section of Cardiovascular Medicine,
Department of Medicine, Yale University
paign to decrease door-to-balloon time in primary PCI.5 The convergence of clinical School of Medicine, and the Center for
and policy interest in door-to-balloon time makes this an opportune occasion to re- Outcomes Research and Evaluation, Yale–
view current knowledge on this topic. New Haven Hospital — both in New Ha-
ven, CT (H.M.K.). Address reprint requests
to Dr. Krumholz at 333 Cedar St., Rm.
Pathoph ysiol o gy of M yo c a r di a l Necrosis I-456 SHM, P.O. Box 208088, New Haven,
CT 06520-8088, or at harlan.krumholz@
yale.edu.
Animal models demonstrate a direct relationship between the duration of coronary-
artery occlusion and the extent of myocardial necrosis.6 Myocardial cell death begins N Engl J Med 2007;357:1631-8.
as early as 20 minutes after coronary-artery occlusion and is usually complete within Copyright © 2007 Massachusetts Medical Society.
6 hours. This period may be extended considerably, however, depending on several
clinical factors, including the presence or absence of intermittent episodes of tran-
sient reperfusion, the extent of collateral circulation, and the presence or absence of
a history of ischemic preconditioning.7,8 Prompt reperfusion therapy can limit myo-
cardial necrosis, although delayed treatment may still provide some benefit by im-
proving left ventricular remodeling and electrical stability.9 Nevertheless, timely treat-
ment produces the most pronounced benefit.
Fibr inoly t ic Ther a py
Patients with ST-elevation myocardial infarction who receive fibrinolytic therapy have
better short- and long-term survival when treatment is instituted rapidly, with early
reestablishment of flow.10 This relationship between time to treatment and outcomes
of fibrinolytic therapy appears to be nonlinear, with the best chance of survival when
fibrinolytic therapy is administered within 2 to 3 hours after the onset of symptoms.11
Little benefit is seen with fibrinolytic therapy after 12 hours, probably because of lost
n engl j med 357;16 www.nejm.org october 18, 2007 1631
Downloaded from www.nejm.org by MARCO I. BANDA MD on November 29, 2008 .
Copyright © 2007 Massachusetts Medical Society. All rights reserved.
The n e w e ng l a n d j o u r na l of m e dic i n e
opportunities for both myocardial salvage12 and consistent with that in other reports.14,21,24 Other
restoration of blood flow, as the thrombus orga- researchers have noted similar findings, with evi-
nizes within the coronary artery over time.13 dence of smaller infarct sizes, fewer major adverse
cardiovascular events, and better long-term sur-
Pr im a r y P CI vival with door-to-balloon times of 90 minutes or
less.24,25
Longer intervals between the onset of symptoms
and balloon time have been correlated with poorer Per for m a nce w i th R e spec t
outcomes in several,14-17 but not all, studies of pri- t o D o or-t o -B a l l o on T ime
mary PCI.18-20 Some studies have also suggested
that delays in the delivery of primary PCI are im- Guidelines from the ACC–AHA and the European
portant only within the first 2 or 3 hours after the Society of Cardiology recommend a treatment goal
onset of symptoms (since this is the time when of 90 minutes or less for door-to-balloon time (or
myocardial salvage is greatest)21 or in high-risk pa- the time from initial medical contact to treat-
tients, such as those with cardiogenic shock.22 In ment),26,27 and this measure is incorporated into
general, studies that have not shown a relationship national, publicly reported quality indicators for
between the time from the onset of symptoms to hospital performance. The Health Quality Alliance
treatment and outcome have had smaller samples, program, which is a combined effort of the Centers
involved special subpopulations of patients, or in- for Medicare and Medicaid Services and the Joint
cluded narrower ranges of time than studies that Commission, includes door-to-balloon time among
have shown such a relationship. However, it is also its core measures of quality of care for acute myo-
possible that even though the extent of myocardial cardial infarction.4
salvage may be similar for fibrinolytic therapy and Door-to-balloon time, as currently measured
primary PCI in the early period after the onset of by the Health Quality Alliance, addresses several
symptoms, PCI is more effective in restoring flow practical concerns. First (despite its terminology),
and improving outcomes during later periods. Ac- the measure permits the use of devices other than
cordingly, some investigators have hypothesized angioplasty balloons that are occasionally used to
that there is a longer treatment window for primary initially reestablish reperfusion. Second, reporting
PCI than has been suggested in studies of fibrino- on the measure changed substantially in July 2006,
lytic therapy.23 Data supporting this theory are shifting from a treatment goal of 120 minutes or
sparse at this time and are not incorporated into less to one of 90 minutes or less, reporting hospi-
current guideline recommendations. tal median as opposed to mean door-to-balloon
In contrast, delays in door-to-balloon time have time, and allowing for clinicians to exclude from
been consistently associated with poorer outcomes the calculation patients for whom delays are con-
in many studies.15,18-20,24 Using data from the sidered unavoidable. These modifications encour-
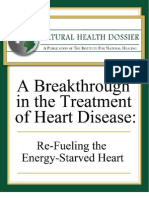
National Registry of Myocardial Infarction, Mc- age a treatment goal that is consistent with the
Namara and colleagues recently noted a strong guidelines, reduce the influence of outlier times,
relationship between door-to-balloon time and in- and acknowledge that delays may be due to ex-
hospital mortality among 29,222 patients with tenuating circumstances in which time is spent on
ST-elevation myocardial infarction.20 When treat- other necessary clinical activities, such as ruling
ment was started within 90 minutes after arrival, out an aortic dissection. Despite these improve-
in-hospital mortality was 3.0%, but it increased to ments, the current measure still has some limita-
4.2%, 5.7%, and 7.4% when delays were 91 to 120 tions. For example, patients in whom ST-elevation
minutes, 121 to 150 minutes, and more than 150 myocardial infarction develops after admission to
minutes, respectively. When adjusted for differ- the hospital or who are transferred from another
ences in patient characteristics, each 15-minute hospital for primary PCI are not currently includ-
reduction in door-to-balloon time from 150 to less ed. These issues deserve more attention in future
than 90 minutes was associated with 6.3 fewer iterations of the measure.
deaths per 1000 patients treated (Fig. 1). This rela- Currently available data suggest that there has
tionship was particularly apparent in patients who been little improvement in door-to-balloon times
arrived at the hospital within 1 hour after the onset in the recent past, and performance on this indi-
of symptoms and had high-risk features, a finding cator lags behind performance on other quality
1632 n engl j med 357;16 www.nejm.org october 18, 2007
Downloaded from www.nejm.org by MARCO I. BANDA MD on November 29, 2008 .
Copyright © 2007 Massachusetts Medical Society. All rights reserved.
Current Concepts
measures for the treatment of acute myocardial
infarction.28,29 In recently reported data from hos- No. of deaths
1.8
25
pitals participating in the National Registry of Relative risk of death
No. of In-Hospital Deaths per 1000
Relative Risk of In-Hospital Death
Myocardial Infarction between 1999 and 2002,
20 1.6
only 35% of all patients were treated within 90
Patients Treated
minutes after arrival at the hospital, and less than
15% of hospitals had a median time of less than 15
1.4
90 minutes.30 Two particular patient subgroups
appear to be at highest risk for long delays in door- 10
to-balloon time: patients who present during off- 1.2
hours (nights and weekends) and those who are 5
transferred from other acute-care facilities. Pa-
tients with ST-elevation myocardial infarction fre- 0 1.0
105 vs. <90 120 vs. <90 135 vs. <90 150 vs. <90
quently present during off-hours, and many health
care facilities are challenged to maintain the avail- Minutes
ability of primary PCI around the clock. Outcomes Figure 1. Relative Risk of In-Hospital Death with Each Additional
with primary PCI are also poorer during off-hours 15-Minute Interval AUTHOR: Krumholz RETAKE
ICM and Number of Deaths Associated with Increases
1st
2nd
in part because of longer delays in activating car- in Door-to-Balloon FIGURE:
REG F Time 1 of 1
as Compared with Treatment within 90 3rd
Minutes.
diac-catheterization laboratories.31 For patients The bars represent
CASE the number of in-hospital deaths per 1000 patients
Revised
Line
who are transferred from other hospitals, there is treated, and the line ARTIST:
EMail represents
ts the relative risk4-C
associated with longer
SIZE
H/T H/T 22p3
the additional challenge of coordinating efforts door-to-balloon times with primary PCI
Enon as
Combo compared with treatment within
90 minutes. Adapted from McNamara et al.20
between facilities on an emergency basis. Unlike AUTHOR, PLEASE NOTE:
Figure has been redrawn and type has been reset.
trauma care systems in many states, for example, Please check carefully.
care for patients with ST-elevation myocardial in- to reperfusion for some patients with ST-elevation
farction is frequently disjointed. In the United myocardial JOB:
infarction
35716 who otherwise could imme-ISSUE: 10-18-07
States, data on the time from arrival at the initial diately be given fibrinolytic therapy. When both
hospital to PCI at the receiving hospital suggest reperfusion strategies can be rapidly performed,
that median delays are as long as 180 minutes and current evidence from clinical trials and registries
that less than 5% of patients are treated within strongly supports the use of primary PCI, based on
90 minutes.32 its superiority in reestablishing coronary blood
Although several clinical trials have shown flow and the lower risks of reinfarction and intra-
promising results of emergency transfer for pri- cerebral hemorrhage.2,39 PCI is also the best op-
mary PCI as compared with on-site fibrinolytic tion for patients with cardiogenic shock 40 and the
therapy,33 only one of these studies involved hos- only option for those with contraindications to fi-
pitals in the United States.34 European health care brinolytic therapy. However, fibrinolytic therapy
systems have been more successful at rapidly remains a practical option for a large number of
transferring and coordinating care for patients patients when there is no immediate access to a
with ST-elevation myocardial infarction because of catheterization laboratory, particularly since the
better integration of emergency medical systems reduced risk of death associated with primary PCI
and hospital networks.35 In limited areas of the may be restricted to high-risk patients.41
United States, the emergency transfer of such pa- The relevant question for clinicians is how long
tients between referral and tertiary care hospitals a delay in access to primary PCI would make fi-
has also been successfully demonstrated.36-38 brinolytic therapy the preferred reperfusion ther-
apy. Unfortunately, there is no clear answer. Several
Sel ec t ing a R eper f usion meta-regression analyses and a recent pooled anal-
Ther a py ysis of patient-level data have examined this is-
sue.42-45 Although results vary substantially among
Given the substantial resources required, many these studies, all suggest that differences between
hospitals in the United States and Europe lack PCI reperfusion therapies with respect to mortality fa-
capabilities, and even fewer provide around-the- vor primary PCI but diminish as PCI-related delays
clock staffing for these procedures. The decision increase, potentially reaching equipoise between
to use primary PCI could substantially delay access 60 and 120 minutes. A recent observational study
n engl j med 357;16 www.nejm.org october 18, 2007 1633
Downloaded from www.nejm.org by MARCO I. BANDA MD on November 29, 2008 .
Copyright © 2007 Massachusetts Medical Society. All rights reserved.
The n e w e ng l a n d j o u r na l of m e dic i n e
from the National Registry of Myocardial Infarc- these facilities, including the support of senior
tion46 showed a similar association, but the report management, innovative and flexible protocols, in-
noted that the effect of PCI-related delays may de- dividual clinical leaders and collaborative teams,
pend on the patient’s age, location of the infarct, use of data feedback to monitor progress and iden-
and duration of symptoms. Patients who are tify problems and successes, and an organization-
younger, have anterior infarction, and present with al culture that fostered improvement efforts.
a shorter duration of symptoms — all factors re- More recent work has quantified the effects of
lated to the efficacy and safety of fibrinolytic different specific strategies associated with shorter
therapy as well as the dangers of delaying treat- door-to-balloon times, with the use of data from
ment — may have worse outcomes with delays in a national survey of 365 hospitals.49 Strategies
primary PCI as compared with rapid fibrinolytic identified as beneficial in this study ranged from
therapy. This study, however, does not provide approaches with minimal resource requirements,
strong enough evidence that there are subgroups such as activation of the catheterization laboratory
for which PCI-related delays are unimportant. by emergency medicine physicians rather than
Because of the lack of definitive data, there is cardiologists and single-call activation by a central
no consensus on the selection of reperfusion ther- page operator, to more complex practices, such as
apy in situations in which primary PCI is not read- the use of prehospital electrocardiography and 24-
ily available. Triage protocols to determine which hour availability of an on-site cardiologist. Others
patients are better candidates for primary PCI than have reported similar findings, with available data
for immediate fibrinolytic therapy have been pro- particularly supporting the use of prehospital elec-
posed, but they have not gained widespread sup- trocardiography,50,51 activation of the catheter-
port in the United States. As discussions of im- ization laboratory by emergency medicine physi-
proved coordination of care for patients with cians,52,53 and data-monitoring systems with
ST-elevation myocardial infarction across hospitals prompt feedback on door-to-balloon time.54 Only
moves forward, matching individual patients with a minority of the hospitals surveyed used many of
the most appropriate treatment will be an impor- these strategies.49
tant goal for health care systems. In most situa- In an effort to help hospitals improve door-to-
tions, rapid administration of fibrinolytic therapy balloon time and translate research into practice,
— within 30 minutes after arrival at the hospital the ACC, in partnership with the AHA, the ACEP,
for patients without contraindications to its use the NHLBI, and others, initiated the Door-to-Bal-
— is recommended when door-to-balloon times loon (D2B) Alliance, a national quality-improve-
of more than 90 minutes are anticipated with pri- ment effort.5 A tool kit and an implementation
mary PCI. As noted earlier, however, some experts package for the D2B Alliance have been created
have suggested that equipoise between the strat- on the basis of an expert review of the literature
egies may occur with delays in access to primary on strategies for improving door-to-balloon time
PCI of as much as 120 minutes or more, depend- (Table 1).
ing on the clinical scenario.47
C ombinat ion S t r ategie s
Reducing Door-to-Balloon Time
Given that there is a limit to how much door-to-
Evidence is emerging about the best approaches balloon time can be shortened, attempts have been
to improving the timeliness of treatment. Estab- made to minimize the impact of delays on out-
lishing hospital-based strategies to reduce door- comes by combining the two reperfusion strate-
to-balloon time in primary PCI requires funda- gies. In one strategy, commonly referred to as
mental changes within complex clinical systems. facilitated PCI, pharmacologic reperfusion with fi-
Bradley and colleagues performed in-depth site brinolytic therapy and glycoprotein IIb/IIIa recep-
visits at 11 top-performing hospitals within the tor blockers is used to reestablish flow early on
National Registry of Myocardial Infarction that had and is followed by emergency PCI. Clinical trials
dramatically shortened their median door-to-bal- have failed to demonstrate that facilitated PCI im-
loon time over recent years.48 Several critical inno- proves outcomes as compared with primary PCI,
vations at the organizational level were noted at and it may actually result in higher mortality.55,56
1634 n engl j med 357;16 www.nejm.org october 18, 2007
Downloaded from www.nejm.org by MARCO I. BANDA MD on November 29, 2008 .
Copyright © 2007 Massachusetts Medical Society. All rights reserved.
Current Concepts
Table 1. Hospital-Based Strategies Associated with Shorter Door-to-Balloon Time and Potential Tools to Implement Them.*
Hospital-Based Strategy Description Potential Tools
Prehospital ECG and activation Greater use of prehospital ECGs by emergency Prehospital ECG policy
medical services, with early activation of Clinical pathway (ECG in emergency department)
catheterization laboratory en route Guidelines for rapid assessment
Protocol for obtaining prompt ECG
Emergency department bypass Direct transfer to the catheterization laboratory Prehospital ECG policy
by emergency medical services using pre- Guidelines for direct activation of catheteriza-
hospital ECGs tion laboratory
Process for triaging patients and Establishment of physical space and guidelines Dedicated personnel and private area for obtain-
rapidly obtaining ECG in the in the emergency department for obtaining ing ECG in triage
emergency department ECGs during triage evaluations
Emergency department activation Activation of the catheterization laboratory Activation policy
of the catheterization laboratory team by emergency medicine physicians
without routine cardiology consultation
Single-call activation Establishment of a single-call system for acti- Alert system
vating the entire catheterization laboratory
team
Rapid arrival of PCI team at hospital Establishment of the expectation that team Staff policy
members will be available to receive the
patient 20–30 min after being paged
Process of performing PCI Clearance of elective cases during routine work Guidelines for work flow during the day and
hours; preparation of angioplasty tables maintaining availability of standardized
during off-hours; clear demarcation of roles equipment during off-hours
for technical and nursing staff Protocol for typical diagnostic and PCI ap-
proaches
Prompt data feedback Routine data monitoring of performance Time-entry form
with provision of prompt feedback E-mail team members door-to-balloon times
after procedure
Senior management commitment Organizational environment with strong sup- Leadership development program
port by senior management as well as a
culture that fosters and sustains organiza-
tional change directed at improving door-
to-balloon time
Team-based approach Emphasis on a team-based approach that Tutorial on continuous quality improvement
provides seamless care from arrival of Team training program
ambulance to balloon inflation before
reperfusion — limit handoffs, one team;
organizational support for continuous
quality improvement
* ECG denotes electrocardiogram, and PCI percutaneous coronary intervention. Adapted from the D2B Alliance.5
However, many of these trials included patients catheterization with the pharmacoinvasive ap-
at hospitals where primary PCI was already rapidly proach is performed at a later time (e.g., the
available, and the approach has yet to be evaluated next day) as opposed to noninvasive risk strati-
in a large number of patients at high risk for pro- fication.
longed delays to mechanical reperfusion, such as Although anecdotal reports indicate that clini-
transfer patients. Another widely discussed strat- cians are increasingly using facilitated PCI and the
egy is the pharmacoinvasive approach,57 in which pharmacoinvasive approach, neither can be recom-
emergency PCI is not routinely performed after mended at this time. This is especially true when
fibrinolytic therapy but is reserved for failed re- full-dose fibrinolytic therapy is combined with
perfusion based on evidence of improved clinical emergency PCI. This practice, one form of facili-
outcomes in this setting (i.e., rescue PCI).58 After tated PCI, should be strongly discouraged, given its
successful reperfusion, routine (nonemergency) potential harm.
n engl j med 357;16 www.nejm.org october 18, 2007 1635
Downloaded from www.nejm.org by MARCO I. BANDA MD on November 29, 2008 .
Copyright © 2007 Massachusetts Medical Society. All rights reserved.
The n e w e ng l a n d j o u r na l of m e dic i n e
using “bypass” protocols that are similar to the
F u t ur e Ch a l l enge s
in Improv ing T ime trauma model. This would allow patients with ST-
t o T r e atmen t in Pr im a r y P CI elevation myocardial infarction to be triaged di-
rectly to hospitals with PCI capabilities by emer-
Targeting improvement of door-to-balloon time gency medical services rather than to the nearest
at hospitals that already provide primary PCI is hospital. However, this approach would be best
the aim of current efforts such as the D2B Alli- implemented with the use of prehospital electro-
ance. If successful, this work will enhance qual- cardiography, which is still uncommon in the
ity at these facilities. Future challenges will be to United States.63
optimize primary PCI as its use extends to larger Systems of care that integrate many of these
populations of patients by shortening the overall approaches are being developed in some regions
time from the onset of symptoms to treatment. of the United States and are the focus of the
This focus will include strategies for reducing the AHA program Mission Lifeline.64 Although there
time from symptom onset to initial contact by pa- is early evidence of success in limited areas, broad
tients with the health care system and improving generalizability of these systems has yet to be dem-
the use of emergency medical systems, both of onstrated. Any improvements in access to primary
which have been largely unresponsive to tradition- PCI with these strategies also must be balanced
al public education campaigns.59 against the use of immediate fibrinolytic therapy,
In an effort to expand the availability of PCI, which remains a reasonable alternative for reper-
some regions are now permitting primary PCI at fusion therapy in selected instances. Matching
hospitals with catheterization laboratories but no patients with the most appropriate treatment and
on-site cardiac surgery or elective PCI. Early stud- location will entail developing a level of coordina-
ies suggest improved clinical outcomes with this tion and collaboration among hospitals beyond
approach, as compared with fibrinolytic therapy, what is currently available in the U.S. health care
when it is associated with a dedicated, primary PCI system but is achievable.
development program.60 As compared with trans- Supported by grants from the National Heart, Lung, and Blood
fer for primary PCI, primary PCI at hospitals with- Institute (R01HL072575) and the Patrick and Catherine Weldon
Donaghue Medical Research Foundation (02-102, to Dr. Bradley).
out on-site cardiac surgery has been associated No potential conflict of interest relevant to this article was
with shorter times to treatment, with some data reported.
suggesting similar short-term mortality.61,62 The We thank Drs. Eric R. Bates and Henry H. Ting for their re-
view of earlier drafts of the manuscript, Mr. Yongfei Wang for
evidence in this area, however, is very limited. providing analytic support, and Ms. Maria Johnson for help with
More recently, there has been great interest in the preparation of the manuscript.
References
1. Keeley EC, Hillis LD. Primary PCI for Jennings RB. The wavefront phenomenon from all randomised trials of more than
myocardial infarction with ST-segment el- of ischemic cell death. 1. Myocardial infarct 1000 patients. Lancet 1994;343:311-22.
evation. N Engl J Med 2007;356:47-54. size vs duration of coronary occlusion in [Erratum, Lancet 1994;343:742.]
2. Keeley EC, Boura JA, Grines CL. Pri- dogs. Circulation 1977;56:786-94. 11. Boersma E, Maas AC, Deckers JW, Si-
mary angioplasty versus intravenous 7. Christian TF, Schwartz RS, Gibbons moons ML. Early thrombolytic treatment
thrombolytic therapy for acute myocardi- RJ. Determinants of infarct size in reper- in acute myocardial infarction: reapprais-
al infarction: a quantitative review of 23 fusion therapy for acute myocardial in- al of the golden hour. Lancet 1996;348:
randomised trials. Lancet 2003;361:13-20. farction. Circulation 1992;86:81-90. 771-5.
3. Giugliano RP, Braunwald E. Selecting 8. Kloner RA, Shook T, Antman EM, et 12. EMERAS (Estudio Multicéntrico Es-
the best reperfusion strategy in ST-eleva- al. Prospective temporal analysis of the treptoquinasa Repúblicas de América del
tion myocardial infarction: it’s all a mat- onset of preinfarction angina versus out- Sur) Collaborative Group. Randomised trial
ter of time. Circulation 2003;108:2828-30. come: an ancillary study in TIMI-9B. Cir- of late thrombolysis in patients with sus-
4. Hospital Compare — a quality tool culation 1998;97:1042-5. pected acute myocardial infarction. Lan-
for adults, including people with Medicare. 9. Kim CB, Braunwald E. Potential ben- cet 1993;342:767-72.
Washington, DC: Department of Health efits of late reperfusion of infarcted myo- 13. Chesebro JH, Knatterud G, Roberts R,
and Human Services. (Accessed September cardium: the open artery hypothesis. Cir- et al. Thrombolysis in Myocardial Infarc-
21, 2007, at http://www.hospitalcompare. culation 1993;88:2426-36. tion (TIMI) trial, phase I: a comparison
hhs.gov/.) 10. Fibrinolytic Therapy Trialists’ (FTT) between intravenous tissue plasminogen
5. D2B: An Alliance for Quality home Collaborative Group. Indications for fibri- activator and intravenous streptokinase:
page. (Accessed September 21, 2007, at nolytic therapy in suspected acute myocar- clinical findings through hospital dis-
http://www.d2balliance.org.) dial infarction: collaborative overview of charge. Circulation 1987;76:142-54.
6. Reimer KA, Lowe JE, Rasmussen MM, early mortality and major morbidity results 14. Antoniucci D, Valenti R, Migliorini A,
1636 n engl j med 357;16 www.nejm.org october 18, 2007
Downloaded from www.nejm.org by MARCO I. BANDA MD on November 29, 2008 .
Copyright © 2007 Massachusetts Medical Society. All rights reserved.
Current Concepts
et al. Relation of time to treatment and matter? Observations from four current dial infarction for percutaneous coronary
mortality in patients with acute myocar- reperfusion trials. J Am Coll Cardiol 2005; intervention. Am Heart J 2005;150:373-
dial infarction undergoing primary coro- 45:Suppl 3:225A. abstract. 84.
nary angioplasty. Am J Cardiol 2002;89: 26. Antman EM, Anbe DT, Armstrong 37. Henry TD, Sharkey SW, Burke MN, et al.
1248-52. PW, et al. ACC/AHA guidelines for the A regional system to provide timely access
15. Brodie BR, Stone GW, Cox DA, et al. management of patients with ST-eleva- to percutaneous coronary intervention for
Impact of treatment delays on outcomes tion myocardial infarction: a report of the ST-elevation myocardial infarction. Circula-
of primary percutaneous coronary inter- American College of Cardiology/Ameri- tion 2007;116:721-8.
vention for acute myocardial infarction: can Heart Association Task Force on Prac- 38. Ting HH, Rihal CS, Gersh BJ, et al.
analysis from the CADILLAC trial. Am tice Guidelines (Committee to Revise the Regional systems of care to optimize time-
Heart J 2006;151:1231-8. 1999 Guidelines for the Management of liness of reperfusion therapy for ST-eleva-
16. De Luca G, Suryapranata H, Ottervan- Patients with Acute Myocardial Infarc- tion myocardial infarction: the Mayo Clin-
ger JP, Antman EM. Time delay to treat- tion). Circulation 2004;110:e82-e292. ic STEMI protocol. Circulation 2007;116:
ment and mortality in primary angioplas- [Errata, Circulation 2005;111:2013-4, 2007; 729-36.
ty for acute myocardial infarction: every 115:e411.] 39. Stenestrand U, Lindbäck J, Wallentin
minute of delay counts. Circulation 2004; 27. Van de Werf F, Ardissino D, Betriu A, L. Long-term outcome of primary percuta-
109:1223-5. et al. Management of acute myocardial neous coronary intervention vs prehospital
17. De Luca G, Suryapranata H, Zijlstra F, infarction in patients presenting with ST- and in-hospital thrombolysis for patients
et al. Symptom-onset-to-balloon time and segment elevation. Eur Heart J 2003;24:28- with ST-elevation myocardial infarction.
mortality in patients with acute myocar- 66. JAMA 2006;296:1749-56.
dial infarction treated by primary angio- 28. Jha AK, Li Z, Orav EJ, et al. Care in U. 40. Hochman JS, Sleeper LA, Webb JG, et
plasty. J Am Coll Cardiol 2003;42:991-7. S. hospitals — the Hospital Quality Alli- al. Early revascularization in acute myo-
18. Berger PB, Ellis SG, Holmes DR Jr, et ance program. N Engl J Med 2005;353:265- cardial infarction complicated by cardio-
al. Relationship between delay in perform- 74. genic shock. N Engl J Med 1999;341:625-
ing direct coronary angioplasty and early 29. Williams SC, Schmaltz SP, Morton DJ, 34.
clinical outcome in patients with acute Koss RG, Loeb JM. Quality of care in U.S. 41. Thune JJ, Hoefsten DE, Lindholm MG,
myocardial infarction: results from the hospitals as reflected by standardized et al. Simple risk stratification at admis-
Global Use of Strategies to Open Occluded measures, 2002–2004. N Engl J Med 2005; sion to identify patients with reduced
Arteries in Acute Coronary Syndromes 353:255-64. mortality from primary angioplasty. Cir-
(GUSTO-IIb) trial. Circulation 1999;100: 30. McNamara RL, Herrin J, Bradley EH, culation 2005;112:2017-21.
14-20. et al. Hospital improvement in time to re- 42. Kent DM, Lau J, Selker HP. Balancing
19. Cannon CP, Gibson CM, Lambrew CT, perfusion in patients with acute myocar- the benefits of primary angioplasty
et al. Relationship of symptom-onset-to- dial infarction, 1999 to 2002. J Am Coll against the benefits of thrombolytic ther-
balloon time and door-to-balloon time Cardiol 2006;47:45-51. apy for acute myocardial infarction: the
with mortality in patients undergoing an- 31. Magid DJ, Wang Y, Herrin J, et al. Re- importance of timing. Eff Clin Pract
gioplasty for acute myocardial infarction. lationship between time of day, day of 2001;4:214-20.
JAMA 2000;283:2941-7. week, timeliness of reperfusion, and in- 43. Nallamothu BK, Antman EM, Bates
20. McNamara RL, Wang Y, Herrin J, et hospital mortality for patients with acute ER. Primary percutaneous coronary inter-
al. Effect of door-to-balloon time on mor- ST-segment elevation myocardial infarc- vention versus fibrinolytic therapy in
tality in patients with ST-segment eleva- tion. JAMA 2005;294:803-12. acute myocardial infarction: does the
tion myocardial infarction. J Am Coll Car- 32. Nallamothu BK, Bates ER, Herrin J, et choice of fibrinolytic agent impact on the
diol 2006;47:2180-6. al. Times to treatment in transfer patients importance of time-to-treatment? Am J
21. Brodie BR, Stuckey TD, Wall TC, et al. undergoing primary percutaneous coro- Cardiol 2004;94:772-4.
Importance of time to reperfusion for 30- nary intervention in the United States: 44. Betriu A, Masotti M. Comparison of
day and late survival and recovery of left National Registry of Myocardial Infarction mortality rates in acute myocardial in-
ventricular function after primary angio- (NRMI)-3/4 analysis. Circulation 2005; farction treated by percutaneous coronary
plasty for acute myocardial infarction. 111:761-7. intervention versus fibrinolysis. Am J Car-
J Am Coll Cardiol 1998;32:1312-9. 33. Dalby M, Bouzamondo A, Lechat P, diol 2005;95:100-1.
22. Brodie BR, Stuckey TD, Muncy DB, et Montalescot G. Transfer for primary an- 45. Boersma E. Does time matter? A pooled
al. Importance of time-to-reperfusion in gioplasty versus immediate thrombolysis analysis of randomized clinical trials com-
patients with acute myocardial infarction in acute myocardial infarction: a meta- paring primary percutaneous coronary in-
with and without cardiogenic shock treat- analysis. Circulation 2003;108:1809-14. tervention and in-hospital fibrinolysis in
ed with primary percutaneous coronary 34. Grines CL, Westerhausen DR Jr, Grines acute myocardial infarction patients. Eur
intervention. Am Heart J 2003;145:708-15. LL, et al. A randomized trial of transfer Heart J 2006;27:779-88.
23. Schömig A, Ndrepepa G, Kastrati A. for primary angioplasty versus on-site 46. Pinto DS, Kirtane AJ, Nallamothu BK,
Late myocardial salvage: time to recog- thrombolysis in patients with high-risk et al. Hospital delays in reperfusion for ST-
nize its reality in the reperfusion therapy myocardial infarction: the Air Primary elevation myocardial infarction: implica-
of acute myocardial infarction. Eur Heart Angioplasty in Myocardial Infarction study. tions when selecting a reperfusion strate-
J 2006;27:1900-7. J Am Coll Cardiol 2002;39:1713-9. gy. Circulation 2006;114:2019-25.
24. Brodie BR, Hansen C, Stuckey TD, et 35. Kalla K, Christ G, Karnik R, et al. 47. Van de Werf FJ. Fine-tuning the selec-
al. Door-to-balloon time with primary per- Implementation of guidelines improves tion of a reperfusion strategy. Circulation
cutaneous coronary intervention for acute the standard of care: the Viennese regis- 2006;114:2002-3.
myocardial infarction impacts late cardiac try on reperfusion strategies in ST-eleva- 48. Bradley EH, Curry LA, Webster TR, et
mortality in high-risk patients and patients tion myocardial infarction (Vienna STEMI al. Achieving rapid door-to-balloon times:
presenting early after the onset of symp- registry). Circulation 2006;113:2398-405. how top hospitals improve complex clinical
toms. J Am Coll Cardiol 2006;47:289-95. 36. Henry TD, Unger BT, Sharkey SW, et al. systems. Circulation 2006;113:1079-85.
25. O’Neill WW, Grines CL, Dixon SR, et Design of a standardized system for trans- 49. Bradley EH, Herrin J, Wang Y, et al.
al. Does a 90-minute door-to-balloon time fer of patients with ST-elevation myocar- Strategies for reducing the door-to-balloon
n engl j med 357;16 www.nejm.org october 18, 2007 1637
Downloaded from www.nejm.org by MARCO I. BANDA MD on November 29, 2008 .
Copyright © 2007 Massachusetts Medical Society. All rights reserved.
Current Concepts
time in acute myocardial infarction. N Engl cet 2006;367:579-88. [Erratum, Lancet JAMA 2002;287:1943-51. [Erratum, JAMA
J Med 2006;355:2308-20. 2006;367:1656.] 2002;287:3212.]
50. Curtis JP, Portnay EL, Wang Y, et al. 56. Primary versus tenecteplase-facilitated 61. Wharton TP, Grines LL, Turco MA, et
The pre-hospital electrocardiogram and percutaneous coronary intervention in pa- al. Primary angioplasty in acute myocar-
time to reperfusion in patients with acute tients with ST-segment elevation acute myo- dial infarction at hospitals with no sur-
myocardial infarction, 2000-2002: findings cardial infarction (ASSENT-4 PCI): ran- gery on-site (the PAMI-No SOS study) ver-
from the National Registry of Myocardial domised trial. Lancet 2006;367:569-78. sus transfer to surgical centers for primary
Infarction-4. J Am Coll Cardiol 2006;47: 57. Armstrong PW. A comparison of phar- angioplasty. J Am Coll Cardiol 2004;43:
1544-52. macologic therapy with/without timely 1943-50.
51. Swor R, Hegerberg S, McHugh-McNally coronary intervention vs. primary percu- 62. Wharton TP. Should patients with
A, Goldstein M, McEachin CC. Prehospi- taneous intervention early after ST-eleva- acute myocardial infraction be transferred
tal 12-lead ECG: efficacy or effectiveness? tion myocardial infarction: the WEST to a tertiary center for primary angioplas-
Prehosp Emerg Care 2006;10:374-7. (Which Early ST-elevation myocardial in- ty or receive it at qualified hospitals in
52. Thatcher JL, Gilseth TA, Adlis S. Im- farction Therapy) study. Eur Heart J 2006; community? The case for community hos-
proved efficiency in acute myocardial in- 27:1530-8. pital angioplasty. Circulation 2005;112:
farction care through commitment to 58. Wijeysundera HC, Vijayaraghavan R, 3509-20.
emergency department-initiated primary Nallamothu BK, et al. Rescue angioplasty 63. Garvey JL, MacLeod BA, Sopko G, et
PCI. J Invasive Cardiol 2003;15:693-8. or repeat fibrinolysis after failed fibrino- al. Pre-hospital 12-lead electrocardiogra-
53. Jacoby J, Axelband J, Patterson J, Bel- lytic therapy for ST-segment myocardial phy programs: a call for implementation
letti D, Heller M. Cardiac cath lab activa- infarction: a meta-analysis of randomized by emergency medical services systems pro-
tion by the emergency physician without trials. J Am Coll Cardiol 2007;49:422-30. viding advanced life support — National
prior consultation decreases door-to-bal- 59. Luepker RV, Raczynski JM, Osganian Heart Attack Alert Program (NHAAP) Co-
loon time. J Invasive Cardiol 2005;17: S, et al. Effect of a community interven- ordinating Committee; National Heart,
154-5. tion on patient delay and emergency med- Lung, and Blood Institute (NHLBI); Na-
54. Ward MR, Lo ST, Herity NA, Lee DP, ical service use in acute coronary heart tional Institutes of Health. J Am Coll Car-
Yeung AC. Effect of audit on door-to-infla- disease: The Rapid Early Action for Coro- diol 2006;47:485-91.
tion times in primary angioplasty/stenting nary Treatment (REACT) Trial. JAMA 2000; 64. Jacobs AK, Antman EM, Ellrodt G, et
for acute myocardial infarction. Am J Car- 284:60-7. al. Recommendation to develop strategies
diol 2001;87:336-8, A9. 60. Aversano T, Aversano LT, Passamani to increase the number of ST-segment-ele-
55. Keeley EC, Boura JA, Grines CL. E, et al. Thrombolytic therapy vs primary vation myocardial infarction patients with
Comparison of primary and facilitated percutaneous coronary intervention for timely access to primary percutaneous cor-
percutaneous coronary interventions for myocardial infarction in patients present- onary intervention. Circulation 2006;113:
ST-elevation myocardial infarction: quan- ing to hospitals without on-site cardiac 2152-63.
titative review of randomised trials. Lan- surgery: a randomized controlled trial. Copyright © 2007 Massachusetts Medical Society.
collections of articles on the journal’s web site
The Journal’s Web site (www.nejm.org) sorts published articles into
more than 50 distinct clinical collections, which can be used as convenient
entry points to clinical content. In each collection, articles are cited in reverse
chronologic order, with the most recent first.
1638 n engl j med 357;16 www.nejm.org october 18, 2007
Downloaded from www.nejm.org by MARCO I. BANDA MD on November 29, 2008 .
Copyright © 2007 Massachusetts Medical Society. All rights reserved.
You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Treatment of Heart DiseaseDocument9 pagesTreatment of Heart DiseaseOriol Borràs Ferré100% (2)
- Evidence-Based Nursing Care of Patient With Acute Myocardial Infarction: Case ReportDocument7 pagesEvidence-Based Nursing Care of Patient With Acute Myocardial Infarction: Case ReportAhmed AlkhaqaniNo ratings yet
- EKG Clep TestDocument13 pagesEKG Clep TestElissa LafondNo ratings yet
- NCP For Acute Coronary SyndromeDocument3 pagesNCP For Acute Coronary Syndromesarahtot75% (4)
- Ecg Interpretation:: The BasicsDocument40 pagesEcg Interpretation:: The BasicsRavi SharmaNo ratings yet
- Ebook Electrocardiography For Healthcare Professionals PDF Full Chapter PDFDocument67 pagesEbook Electrocardiography For Healthcare Professionals PDF Full Chapter PDFkenneth.bell482100% (28)
- Cardiac ArrestDocument19 pagesCardiac ArrestHaimelien De LimosNo ratings yet
- History of Present IllnessDocument1 pageHistory of Present IllnessMenly SusadaNo ratings yet
- Pediatric Chest PainDocument77 pagesPediatric Chest PaintraviscNo ratings yet
- DR Mustika Mahbubi SPJP FIHA-How To Treat Acute Coronary Sydrome (STEMI Patient) in Pre and Post HospitalDocument59 pagesDR Mustika Mahbubi SPJP FIHA-How To Treat Acute Coronary Sydrome (STEMI Patient) in Pre and Post HospitalHiszom AsyhariNo ratings yet
- Ecg PDFDocument38 pagesEcg PDFKeerthana BalachandiranNo ratings yet
- Protocol of Management of Acute Heart FailureDocument5 pagesProtocol of Management of Acute Heart FailureMc inloveNo ratings yet
- Terapi Cairan PD Syok KardiogenikDocument27 pagesTerapi Cairan PD Syok KardiogenikSri AsmawatiNo ratings yet
- 28,29 Management of Cardiac ArrhythmiasDocument41 pages28,29 Management of Cardiac ArrhythmiasSL Dr ChEMiSNo ratings yet
- Pharma Medical Director Cardiology in NYC Resume Ronald HabermanDocument3 pagesPharma Medical Director Cardiology in NYC Resume Ronald HabermanRonaldHabermanNo ratings yet
- Yashwanth - IHD HFrEfDocument16 pagesYashwanth - IHD HFrEfYashwanth N BNo ratings yet
- HealthDocument21 pagesHealthLalita NaiduNo ratings yet
- Cardiologia Banco Con 2016Document192 pagesCardiologia Banco Con 2016Francisco JavierNo ratings yet
- Jurnal 1. OAVRT DogsDocument8 pagesJurnal 1. OAVRT DogsAlda AdeliaNo ratings yet
- Modified by Dr. Salah H Sinjary College of Medicine HMU Department of Medicine 07504454134Document47 pagesModified by Dr. Salah H Sinjary College of Medicine HMU Department of Medicine 07504454134Chro MANo ratings yet
- Holter Angel SuarezDocument8 pagesHolter Angel SuarezDRA.MARIANGELA N SUÁREZ BNo ratings yet
- PericarditisDocument11 pagesPericarditisrbarcellonaNo ratings yet
- RAVEL 4 AnosDocument13 pagesRAVEL 4 AnosRui FonteNo ratings yet
- Written ExaminationDocument26 pagesWritten ExaminationDigos CdrrmoNo ratings yet
- IM 3A PE Cardiology Dr. JumangitDocument12 pagesIM 3A PE Cardiology Dr. JumangitCzara DyNo ratings yet
- A Seminar On ECGDocument16 pagesA Seminar On ECGVibha C PrabhuNo ratings yet
- Causes of Chest DiscomfortDocument8 pagesCauses of Chest DiscomfortNoelle Grace Ulep BaromanNo ratings yet
- Pre LimesDocument53 pagesPre LimesRikke LegarthNo ratings yet
- Whole MagDocument132 pagesWhole MagshemagononlyNo ratings yet
- HBP 2 0 For WebsiteDocument52 pagesHBP 2 0 For Websitepraks758No ratings yet