You might also like
- Hand Hygiene Knowledge, Perception, and Compliance Among Healthcare WorkersDocument12 pagesHand Hygiene Knowledge, Perception, and Compliance Among Healthcare WorkersIJPHSNo ratings yet
- A Study To Assess The Knowledge and Practices of Hand Hygiene Among Nursing Staff in Different Department of The Hospitals in Uttar PradeshDocument24 pagesA Study To Assess The Knowledge and Practices of Hand Hygiene Among Nursing Staff in Different Department of The Hospitals in Uttar PradeshEditor IJTSRD100% (1)
- Hand Hygiene Guidelines For Front Line Health Care WorkersDocument2 pagesHand Hygiene Guidelines For Front Line Health Care WorkersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Hand Hygiene Compliance, Knowledge and Perception Among Healthcare Workers in A Tertiary Care Center in South IndiaDocument4 pagesHand Hygiene Compliance, Knowledge and Perception Among Healthcare Workers in A Tertiary Care Center in South IndiaIJAR JOURNALNo ratings yet
- MotivasiDocument5 pagesMotivasiIrfan MadamangNo ratings yet
- Knowledge, Attitude and Practices of Hand Hygiene Among Nursing Staff and StudentsDocument12 pagesKnowledge, Attitude and Practices of Hand Hygiene Among Nursing Staff and Studentsjoko samudro100% (1)
- HIVAR_Art_52393-10Document4 pagesHIVAR_Art_52393-10Kristiani AmbengNo ratings yet
- Knowledge of Hand Hygiene and Compliance Among Clinicians - at A Level Six Hospital in Kenya: A Cross Sectional StudyDocument20 pagesKnowledge of Hand Hygiene and Compliance Among Clinicians - at A Level Six Hospital in Kenya: A Cross Sectional StudyIJAR JOURNALNo ratings yet
- Hand Hygiene Compliance in Healthcare WorkersDocument6 pagesHand Hygiene Compliance in Healthcare WorkersRiska IndrianiNo ratings yet
- Hand Hygiene Practices and Perceptions Among Healthcare Workers in Ghana: A WASH Intervention StudyDocument10 pagesHand Hygiene Practices and Perceptions Among Healthcare Workers in Ghana: A WASH Intervention StudyMaizura Syahirah MohtadaNo ratings yet
- Impact On Health Care Associated Infection Rates by Continuous Training of Nursing Staff in Our HospitalDocument4 pagesImpact On Health Care Associated Infection Rates by Continuous Training of Nursing Staff in Our HospitalAnkush JainNo ratings yet
- Predictors of Hand Hygiene Compliance in the ABHR EraDocument8 pagesPredictors of Hand Hygiene Compliance in the ABHR EraI Komang BudianaNo ratings yet
- Macaraan - JPH - Hygiene HabitsDocument2 pagesMacaraan - JPH - Hygiene HabitsWillard MacaraanNo ratings yet
- 5.NJCM Infection Control KayakalpDocument4 pages5.NJCM Infection Control KayakalpDr.Shivaraj BMNo ratings yet
- Smartphone Text Message Service To Foster Hand Hygiene ComplianceDocument6 pagesSmartphone Text Message Service To Foster Hand Hygiene ComplianceEszter TóthNo ratings yet
- Sadulerios 2017Document8 pagesSadulerios 2017I Komang BudianaNo ratings yet
- 2-Article Text-128-2-10-20200328Document8 pages2-Article Text-128-2-10-20200328Siti HamsyiahNo ratings yet
- Journal of Occupational Health - 2020 - Hwang - Responding To The COVID 19 Pandemic The Role of Occupational HealthDocument7 pagesJournal of Occupational Health - 2020 - Hwang - Responding To The COVID 19 Pandemic The Role of Occupational HealthFitrahNo ratings yet
- Care For Vulnerable Populations during COVID-19 Pandemic: Clinical Updates in COVID-19From EverandCare For Vulnerable Populations during COVID-19 Pandemic: Clinical Updates in COVID-19No ratings yet
- Hand Hygiene Compliance Improved Using PDCADocument5 pagesHand Hygiene Compliance Improved Using PDCAFaozan FikriNo ratings yet
- Drantonamrcontrolinthe PhilippinesDocument27 pagesDrantonamrcontrolinthe PhilippinesJuhne del ReyNo ratings yet
- Care For Vulnerable Populations During COVID-19 PandemicFrom EverandCare For Vulnerable Populations During COVID-19 PandemicNo ratings yet
- 7 AHM Antibiotic PolicyDocument98 pages7 AHM Antibiotic PolicyfaisalNo ratings yet
- Hpmij 03 00153Document6 pagesHpmij 03 00153Azmi SevenfoldismNo ratings yet
- Hospital Infection Control Manual AIIMS Raipur2019 (Word)Document204 pagesHospital Infection Control Manual AIIMS Raipur2019 (Word)Dipali SolankiNo ratings yet
- Zhang 2019Document8 pagesZhang 2019Siti HamsyiahNo ratings yet
- Simplifying The World Health Organization Protocol 3 Steps Versus 6 Steps For Performance of Hand Hygiene in A Cluster-Randomized TrialDocument7 pagesSimplifying The World Health Organization Protocol 3 Steps Versus 6 Steps For Performance of Hand Hygiene in A Cluster-Randomized TrialManuel GuzmanNo ratings yet
- Hand Hygiene ArticleDocument7 pagesHand Hygiene ArticlechijNo ratings yet
- Hand Hygiene For All Initiative: Improving Access and Behaviour in Health Care FacilitiesDocument16 pagesHand Hygiene For All Initiative: Improving Access and Behaviour in Health Care FacilitiesMai BasionyNo ratings yet
- Knowledge, Attitude and Practicesamongprimary Care Workers On Infection, Prevention and Control Amidst The Covid-19 PandemicDocument25 pagesKnowledge, Attitude and Practicesamongprimary Care Workers On Infection, Prevention and Control Amidst The Covid-19 PandemicIJAR JOURNALNo ratings yet
- Translating a hand therapy program into routine care: An effectiveness-implementation studyDocument11 pagesTranslating a hand therapy program into routine care: An effectiveness-implementation studyFranz CalumpitNo ratings yet
- Perspectives and Attitudes of Patients With COVID-19 Toward A Telerehabilitation Programme: A Qualitative StudyDocument12 pagesPerspectives and Attitudes of Patients With COVID-19 Toward A Telerehabilitation Programme: A Qualitative StudyFernando JarixNo ratings yet
- ART2016631Document7 pagesART2016631Tmanoj PraveenNo ratings yet
- Community Teaching Plan: Hygiene Practices in Preventing HaisDocument18 pagesCommunity Teaching Plan: Hygiene Practices in Preventing HaisSamwel KangyNo ratings yet
- Liu 2020Document4 pagesLiu 2020Delta Timur01No ratings yet
- The Ijbm Journal-Nida Khoiriah From Indonesia-Lean HospitalDocument11 pagesThe Ijbm Journal-Nida Khoiriah From Indonesia-Lean Hospitalyanjangmed rspdsNo ratings yet
- Knowledge and Hand Hygiene Practice of Healthcare Workers inDocument11 pagesKnowledge and Hand Hygiene Practice of Healthcare Workers inBarangay MotibotNo ratings yet
- Nurses' Perceptions of Reasons For Persistent Low Rates in Hand Hygiene ComplianceDocument6 pagesNurses' Perceptions of Reasons For Persistent Low Rates in Hand Hygiene CompliancejamuluddinNo ratings yet
- "Clean Care For All - It's in Your Hands": The May 5th, 2019 World Health Organization SAVE LIVES: Clean Your Hands CampaignDocument6 pages"Clean Care For All - It's in Your Hands": The May 5th, 2019 World Health Organization SAVE LIVES: Clean Your Hands CampaignArif WibowoNo ratings yet
- Infection Control Plan FY 2019 PDFDocument6 pagesInfection Control Plan FY 2019 PDFdjprh tbdotsNo ratings yet
- Clinical Protection Handbook: for Healthcare Workers against COVID-19From EverandClinical Protection Handbook: for Healthcare Workers against COVID-19No ratings yet
- Sadulerios2017 PDFDocument5 pagesSadulerios2017 PDFI Komang BudianaNo ratings yet
- Article in Press: Journal of Infection and Public HealthDocument5 pagesArticle in Press: Journal of Infection and Public HealthTiti IndasariNo ratings yet
- Fisioterapia Pós Covid em PortugalDocument2 pagesFisioterapia Pós Covid em PortugalMaria JoanaNo ratings yet
- HandhygieneDocument21 pagesHandhygieneAberaNo ratings yet
- Aplin Snider Et Al 2020 Development and Implementation of An Upper Respiratory Infection Treatment Protocol in ADocument6 pagesAplin Snider Et Al 2020 Development and Implementation of An Upper Respiratory Infection Treatment Protocol in ABBD BBDNo ratings yet
- Assessment of Knowledge and Usage of Hiv Post Exposure Prophylaxis Among Healthcare Workers in A Regional Hospital in GhanaDocument11 pagesAssessment of Knowledge and Usage of Hiv Post Exposure Prophylaxis Among Healthcare Workers in A Regional Hospital in GhanaannisazakirohNo ratings yet
- 3) Z. 10.1016@j.jcrc.2020.06.005 (Alexis Tabah)Document18 pages3) Z. 10.1016@j.jcrc.2020.06.005 (Alexis Tabah)Mastifa HanasitaNo ratings yet
- Donati 2020Document7 pagesDonati 2020marisaNo ratings yet
- Assessment of Preparedness Against Emerging Infectious Disease Among Private Hospitals in A District of South IndiaDocument5 pagesAssessment of Preparedness Against Emerging Infectious Disease Among Private Hospitals in A District of South IndiaNurulfitrahhafidNo ratings yet
- IHI Hand HygieneDocument32 pagesIHI Hand HygieneIan Mizzel A. DulfinaNo ratings yet
- Daftar Tilik Pemenuhan Minimal Untuk PPI Di PuskesmasDocument14 pagesDaftar Tilik Pemenuhan Minimal Untuk PPI Di PuskesmasrosnimalaNo ratings yet
- 3504 - 10. JURNAL B. INDO - Aman Insya AllahDocument11 pages3504 - 10. JURNAL B. INDO - Aman Insya Allahyanjangmed rspdsNo ratings yet
- Initiatives To Reduce Treatments in Bronchiolitis in The Emergency Department and Primary CareDocument7 pagesInitiatives To Reduce Treatments in Bronchiolitis in The Emergency Department and Primary CareMartin Seminario AliagaNo ratings yet
- Hand Hygiene Audit To Study Adherence To Hand Hygiene in A Tertiary Care HospitalDocument4 pagesHand Hygiene Audit To Study Adherence To Hand Hygiene in A Tertiary Care HospitalIJAR JOURNALNo ratings yet
- ADocument4 pagesAphanuel yosefNo ratings yet
- Reducing Hand Recontamination of Healthcare Workers During Covid 19Document2 pagesReducing Hand Recontamination of Healthcare Workers During Covid 19Lujine AłsNo ratings yet
- Compliance with Sharps Injury Prevention Guidelines Among NursesDocument8 pagesCompliance with Sharps Injury Prevention Guidelines Among NursesMrLarry DolorNo ratings yet
- Nurs 390 Group 2 Project 2Document33 pagesNurs 390 Group 2 Project 2api-621785757No ratings yet
- BPC categories focus on hair, skin and oral careDocument45 pagesBPC categories focus on hair, skin and oral careSanket ChintawarNo ratings yet
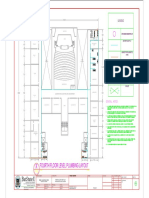
- Architecture Department Floor PlanDocument1 pageArchitecture Department Floor PlanEasy WriteNo ratings yet
- Assessment Standard 7.2-4 Personal Environmental Safety TESTDocument4 pagesAssessment Standard 7.2-4 Personal Environmental Safety TESTnurse1990No ratings yet
- BRC Global Standards For Packaging MaterialDocument11 pagesBRC Global Standards For Packaging MaterialHamid HamidNo ratings yet
- Virex®II 256: One-Step Disinfectant Cleaner and DeodorantDocument2 pagesVirex®II 256: One-Step Disinfectant Cleaner and DeodorantPriyankhaNo ratings yet
- LoA 202 2023 SCRP Emergency Fisheries Activities in Badhaadhe DistrictDocument58 pagesLoA 202 2023 SCRP Emergency Fisheries Activities in Badhaadhe DistrictibrahimNo ratings yet
- Klercide Quat BiguanideDocument12 pagesKlercide Quat BiguanideLee Cole100% (1)
- Boutique Hotel Pitch Deck XLDocument32 pagesBoutique Hotel Pitch Deck XLBea RamosNo ratings yet
- Swachh Bharat AbhiyanDocument2 pagesSwachh Bharat AbhiyanAkshayNo ratings yet
- TratamientoBiologicoAerobio RevAfinidad2011 PDFDocument9 pagesTratamientoBiologicoAerobio RevAfinidad2011 PDFAlberto VELOSA ROANo ratings yet
- Northern California Master Geographic Letter List: CountiesDocument28 pagesNorthern California Master Geographic Letter List: CountiesPrajwal DSNo ratings yet
- Hand Hygiene and Vital Signs DiscussionDocument11 pagesHand Hygiene and Vital Signs DiscussionA CNo ratings yet
- Transform your toilet into a healthier bidetDocument2 pagesTransform your toilet into a healthier bidetscrufftruffleNo ratings yet
- CYDFI Scholarship Program Water ProjectDocument7 pagesCYDFI Scholarship Program Water ProjectDanilo Talaba100% (1)
- PastafssaiDocument27 pagesPastafssaiRISHI FOOD TESTING LABNo ratings yet
- OS Hotel Operation L1 & L2Document183 pagesOS Hotel Operation L1 & L2Kejela AbrahamNo ratings yet
- The Poisoned NeedleDocument220 pagesThe Poisoned NeedleMATRIX528100% (10)
- Septic TanksDocument34 pagesSeptic TanksNiel Gongora100% (1)
- Zero Open Defecation ProgramDocument64 pagesZero Open Defecation ProgramAlexandra BanteguiNo ratings yet
- Sanitation Quo Vadis MagtibayDocument5 pagesSanitation Quo Vadis MagtibayBoni MagtibayNo ratings yet
- Health6 - q1 - Mod2 - Self Management Skills - v4Document24 pagesHealth6 - q1 - Mod2 - Self Management Skills - v4ronie aduana67% (3)
- Your Booking at Radisson Gurugram Sohna Road City Center Is Confirmed!Document4 pagesYour Booking at Radisson Gurugram Sohna Road City Center Is Confirmed!Rohit RaiNo ratings yet
- Preventing Healthcare-Associated InfectionsDocument16 pagesPreventing Healthcare-Associated InfectionsRDi JNo ratings yet
- Importance of Swachh Bharat Abhiyan for Rural AreasDocument35 pagesImportance of Swachh Bharat Abhiyan for Rural AreasPriyanshu Agrawal100% (1)
- Review On CoparDocument25 pagesReview On CoparJaylord VerazonNo ratings yet
- Food Hygiene and HaccpDocument65 pagesFood Hygiene and HaccpFirda ShofiaNo ratings yet
- MSDS Colalube 3404Document3 pagesMSDS Colalube 3404mndmattNo ratings yet
- Mecha Woreda WASH 3 Years Strategic Plan Translated From AmharicDocument19 pagesMecha Woreda WASH 3 Years Strategic Plan Translated From AmharicAbebaw AzagiNo ratings yet
- Hotel CodeDocument17 pagesHotel CodeJayvee Latosa DividinaNo ratings yet
- MSDSDocument31 pagesMSDSvienkoNo ratings yet