You might also like
- Hybrid Repair of Aortic Arch AneurysmDocument8 pagesHybrid Repair of Aortic Arch AneurysmFrancesca MazzolaniNo ratings yet
- Jocs.15492 Articulo KozirevDocument7 pagesJocs.15492 Articulo KozirevCorazon MabelNo ratings yet
- Case Reports Intravascular Ultrasound Identification of Intraluminal Embolic Plaque Material During Carotid Angioplasty With StentingDocument5 pagesCase Reports Intravascular Ultrasound Identification of Intraluminal Embolic Plaque Material During Carotid Angioplasty With StentingRicardo Novoa AlvarezNo ratings yet
- 480 FullDocument6 pages480 FullStamenko S. SusakNo ratings yet
- NAIS Initial PaperDocument10 pagesNAIS Initial Paperjesus Porras ColonNo ratings yet
- KalangosDocument3 pagesKalangosCorazon MabelNo ratings yet
- Central Venous Port Placement in Advanced Breast Cancer Patients: Comparison of The Anatomic-Landmark and Ultrasound-Guided TechniquesDocument4 pagesCentral Venous Port Placement in Advanced Breast Cancer Patients: Comparison of The Anatomic-Landmark and Ultrasound-Guided TechniquesLydia AmaliaNo ratings yet
- End Arte Rec To MyDocument7 pagesEnd Arte Rec To MyLuming LiNo ratings yet
- Timetable PosterExDocument45 pagesTimetable PosterExNeo Rodriguez AlvaradoNo ratings yet
- AVF NewDocument81 pagesAVF NewBasit AliNo ratings yet
- Pi Is 0003497500014818Document7 pagesPi Is 0003497500014818GKNo ratings yet
- The Fate of The Distal Aorta After Repair of Acute Type A Aortic DissectionDocument10 pagesThe Fate of The Distal Aorta After Repair of Acute Type A Aortic Dissectionapi-160333876No ratings yet
- Belhajsoulami 2018Document3 pagesBelhajsoulami 2018rédaNo ratings yet
- SN02Document11 pagesSN02Enrique San NorbertoNo ratings yet
- Aaa RotoDocument11 pagesAaa RotoKarely TapiaNo ratings yet
- Results With Continuous Cardiopulmonary Bypass For The Bidirectional Cavopulmonary Anastomosis - ProQuestDocument7 pagesResults With Continuous Cardiopulmonary Bypass For The Bidirectional Cavopulmonary Anastomosis - ProQuestWilliam WiryawanNo ratings yet
- Abdominal Aortic Aneurysm and AcuteDocument8 pagesAbdominal Aortic Aneurysm and AcuteKristanto Ayomi Ayomi AriNo ratings yet
- Radiology Case ReportsDocument5 pagesRadiology Case ReportsLaila Maria UlfahNo ratings yet
- Kim2012Document5 pagesKim2012Stefanie MelisaNo ratings yet
- Original ArticlesDocument8 pagesOriginal ArticlesHugoNo ratings yet
- Acs 06 05 463Document10 pagesAcs 06 05 463Arun MNNo ratings yet
- (10920684 - Neurosurgical Focus) Falcotentorial Meningiomas - Clinical, Neuroimaging, and Surgical Features in Six PatientsDocument7 pages(10920684 - Neurosurgical Focus) Falcotentorial Meningiomas - Clinical, Neuroimaging, and Surgical Features in Six PatientsPutri PrameswariNo ratings yet
- In Practice: Central Vein StenosisDocument15 pagesIn Practice: Central Vein Stenosisnilmania_01No ratings yet
- Disseccao Tipo b2Document6 pagesDisseccao Tipo b2coopervascba.diradmNo ratings yet
- Surgical Management of Tracheal Compression Caused by Mediastinal Goiter: Is Extracorporeal Circulation Requisite钥Document3 pagesSurgical Management of Tracheal Compression Caused by Mediastinal Goiter: Is Extracorporeal Circulation Requisite钥Indra W SaputraNo ratings yet
- Khairy 2017Document7 pagesKhairy 2017Beby Dwi Lestari BajryNo ratings yet
- Aneurysm Growth After Endovascular Sealing of AbdoDocument6 pagesAneurysm Growth After Endovascular Sealing of AbdoibarbomanNo ratings yet
- 10 1 1 525 6842Document6 pages10 1 1 525 6842sandyNo ratings yet
- MJMHS 1316Document3 pagesMJMHS 1316prima ningratNo ratings yet
- A Simple Technique of Portal Vein Resection and Reconstruction During PancreaticoduodenectomyDocument6 pagesA Simple Technique of Portal Vein Resection and Reconstruction During Pancreaticoduodenectomyyacine26No ratings yet
- 2011 111 Acta Chir Belg PDFDocument4 pages2011 111 Acta Chir Belg PDFMarc Lloyd AlfonsoNo ratings yet
- Article - Sequential Bypass Grafting On The Beating Heart - Blood Flow CharacteristicsDocument4 pagesArticle - Sequential Bypass Grafting On The Beating Heart - Blood Flow Characteristicsfluid_man_brazilNo ratings yet
- JUMDC 6 Arterio VenousDocument6 pagesJUMDC 6 Arterio VenousMudassar SaeedNo ratings yet
- Journal of Cardiothoracic Surgery Journal of Cardiothoracic SurgeryDocument12 pagesJournal of Cardiothoracic Surgery Journal of Cardiothoracic SurgeryFendry KolondamNo ratings yet
- Concomitant Bentall Operation Plus Aortic Arch Replacement SurgeryDocument7 pagesConcomitant Bentall Operation Plus Aortic Arch Replacement Surgeryprofarmah6150No ratings yet
- Aortaresektion Marulli 2015Document6 pagesAortaresektion Marulli 2015t.krbekNo ratings yet
- Ahn 2011Document4 pagesAhn 2011Residentes PediatríaNo ratings yet
- Review Article: Computed Tomography in The Evaluation For Transcatheter Aortic Valve Implantation (TAVI)Document13 pagesReview Article: Computed Tomography in The Evaluation For Transcatheter Aortic Valve Implantation (TAVI)Paul SchoenhagenNo ratings yet
- Clinical Implications of The Angiosome Model in Peripheral Vascular DiseaseDocument13 pagesClinical Implications of The Angiosome Model in Peripheral Vascular DiseaseAntonioNo ratings yet
- Ross OtoHNS2005 ArterialCouplingDocument5 pagesRoss OtoHNS2005 ArterialCouplingSungjin SongNo ratings yet
- 1 s2.0 S0929664608602041 MainDocument9 pages1 s2.0 S0929664608602041 MainEko SiswantoNo ratings yet
- Anastasiadou Trombose Aneurisma2017Document4 pagesAnastasiadou Trombose Aneurisma2017Margarita AucejoNo ratings yet
- Ytad 271Document2 pagesYtad 271Juan LakiNo ratings yet
- Primary and Staged Transposition Arteriovenous Fistulas (Superficialization)Document5 pagesPrimary and Staged Transposition Arteriovenous Fistulas (Superficialization)Anonymous LnWIBo1GNo ratings yet
- Transaortic Valve ReplacementDocument11 pagesTransaortic Valve ReplacementManuela CulicaNo ratings yet
- CT Angiography of The Lower Extremities The Peripheral Vascular System Presents Unique Imaging ChallengesDocument7 pagesCT Angiography of The Lower Extremities The Peripheral Vascular System Presents Unique Imaging ChallengesDavid Puyó100% (1)
- Alexandria Journal of Medicine: Rehab Abdel Rahman El BakryDocument5 pagesAlexandria Journal of Medicine: Rehab Abdel Rahman El BakrySatrio Budi WicaksonoNo ratings yet
- CT Angiography in Vertebral Artery DissectionDocument6 pagesCT Angiography in Vertebral Artery DissectionDaniel AraujoNo ratings yet
- 1 s2.0 0735109788900940 MainDocument11 pages1 s2.0 0735109788900940 MainHarish SubramanianNo ratings yet
- Clinical: "Off-Pump Myocardial Revascularization"Document15 pagesClinical: "Off-Pump Myocardial Revascularization"api-626131140No ratings yet
- Lap Chole DictationDocument2 pagesLap Chole DictationAshish DongreNo ratings yet
- Single-Incision Thoracoscopic Surgery For Primary Spontaneous PneumothoraxDocument4 pagesSingle-Incision Thoracoscopic Surgery For Primary Spontaneous PneumothoraxRiani NazilaNo ratings yet
- Arthroscopic Suture Bridge Transosseus Equivalent Fixation of RC TendonDocument8 pagesArthroscopic Suture Bridge Transosseus Equivalent Fixation of RC TendonIlias GalanopoulosNo ratings yet
- Endoskopik 2.brankialDocument5 pagesEndoskopik 2.brankialDogukan DemirNo ratings yet
- Surgical Treatment of Venous Malformations in Klippel-Trénaunay SyndromeDocument8 pagesSurgical Treatment of Venous Malformations in Klippel-Trénaunay SyndromenikitagustiNo ratings yet
- Et0420 MedAffairs MouawadDocument5 pagesEt0420 MedAffairs MouawadAna Silvia LebrOnNo ratings yet
- PregnancyDocument4 pagesPregnancymutiahmuftihNo ratings yet
- Laparoscopic Cholecystectomy After Conservative Su - 2024 - International JournaDocument4 pagesLaparoscopic Cholecystectomy After Conservative Su - 2024 - International JournaRonald QuezadaNo ratings yet
- Prospective Evaluation of Factors Associated With Early Failure of Arteriovenous Fistulae in Hemodialysis PatientsDocument5 pagesProspective Evaluation of Factors Associated With Early Failure of Arteriovenous Fistulae in Hemodialysis PatientsIvor WilopoNo ratings yet
- Aortic RegurgitationFrom EverandAortic RegurgitationJan VojacekNo ratings yet
- Ease Us Fix ToolDocument7 pagesEase Us Fix ToolGregorio TironaNo ratings yet
- Relay ProtectionDocument26 pagesRelay Protectionnogeshwar100% (1)
- Dissertation Bowden PDFDocument98 pagesDissertation Bowden PDFmostafaNo ratings yet
- Microsoft Power Platform Adoption PlanningDocument84 pagesMicrosoft Power Platform Adoption PlanningcursurilemeleNo ratings yet
- Architect Strengths and Weaknesses - 16personalitiesDocument4 pagesArchitect Strengths and Weaknesses - 16personalitiesIsaacNo ratings yet
- ERP and Oracle E-Business Suite ConceptsDocument73 pagesERP and Oracle E-Business Suite ConceptsAlaa Mostafa100% (1)
- Basic Principle of Semiconductor DiodesDocument5 pagesBasic Principle of Semiconductor DiodessatishasdNo ratings yet
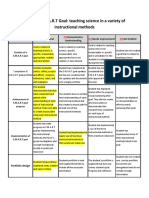
- Smart Goals Rubric 2Document2 pagesSmart Goals Rubric 2api-338549230100% (2)
- Warm Mix Asphalt: "National Perspective"Document46 pagesWarm Mix Asphalt: "National Perspective"Royhan RizkyNo ratings yet
- Summer Internship Project On: "Basics of PHP"Document45 pagesSummer Internship Project On: "Basics of PHP"its me Deepak yadav100% (1)
- Analog Circuits - IDocument127 pagesAnalog Circuits - IdeepakpeethambaranNo ratings yet
- Subgrade Preparation in Earth CutDocument3 pagesSubgrade Preparation in Earth Cutusama buttNo ratings yet
- Trade Secrets Lawsuit V ReebokDocument17 pagesTrade Secrets Lawsuit V ReebokDarren Adam HeitnerNo ratings yet
- 4 5827923419810760428Document250 pages4 5827923419810760428T M Santhosh KumarNo ratings yet
- Methods of TrainingDocument26 pagesMethods of TrainingDevanshuNo ratings yet
- 10 Professional Tax Software Must-Haves White PaperDocument2 pages10 Professional Tax Software Must-Haves White PaperRakesh KumarNo ratings yet
- Members 24 AprilDocument356 pagesMembers 24 Aprilpriyanka chaurasia100% (1)
- Child Has Does: The Adultery, Child Be and Entitled His Own, The Child's That His DueDocument1 pageChild Has Does: The Adultery, Child Be and Entitled His Own, The Child's That His DuerickmortyNo ratings yet
- ZF SI 6hp Family Tree enDocument2 pagesZF SI 6hp Family Tree enfercho573No ratings yet
- How The CBO Works: Jonathan Lewis WWW - Jlcomp.demon - Co.ukDocument37 pagesHow The CBO Works: Jonathan Lewis WWW - Jlcomp.demon - Co.ukomeratisNo ratings yet
- 12 Things You Must Know To Win A Full Scholarship in SwedenDocument51 pages12 Things You Must Know To Win A Full Scholarship in SwedenEmmanuel GeraldNo ratings yet
- Mil DTL 11891g EngDocument96 pagesMil DTL 11891g EngJohn DrakosNo ratings yet
- Satyam GargDocument2 pagesSatyam GargSatyam GargNo ratings yet
- Grundfosliterature 3081153Document120 pagesGrundfosliterature 3081153Cristian RinconNo ratings yet
- Python Lab10 Report SummaryDocument8 pagesPython Lab10 Report SummaryVivekananda ParamahamsaNo ratings yet
- 1.1.4.A PulleyDrivesSprockets FinishedDocument4 pages1.1.4.A PulleyDrivesSprockets FinishedJacob DenkerNo ratings yet
- SafeShop Business Plan PDFDocument16 pagesSafeShop Business Plan PDFkalchati yaminiNo ratings yet
- Parts of A Business LetterDocument7 pagesParts of A Business LetterCharmine SacdalanNo ratings yet
- Crime MappingDocument13 pagesCrime MappingRea Claire QuimnoNo ratings yet
- UNIT V WearableDocument102 pagesUNIT V WearableajithaNo ratings yet