0% found this document useful (0 votes)
32 views1 pageIncident Notification Form Template
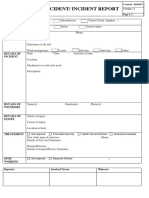
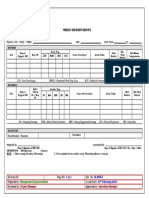
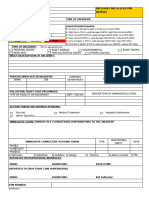
The document outlines the procedure for reporting incidents within a project, requiring the Sub-Contractor to notify the Main Contractor within one hour and submit an Incident Notification Form within twenty-four hours. It includes sections for details such as the type of incident, date, time, location, persons involved, injuries, and treatments. There are also spaces for signatures of the reporter, agreement, and acknowledgment by relevant parties.
Uploaded by
Abdullah AliemraanCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
32 views1 pageIncident Notification Form Template
The document outlines the procedure for reporting incidents within a project, requiring the Sub-Contractor to notify the Main Contractor within one hour and submit an Incident Notification Form within twenty-four hours. It includes sections for details such as the type of incident, date, time, location, persons involved, injuries, and treatments. There are also spaces for signatures of the reporter, agreement, and acknowledgment by relevant parties.
Uploaded by
Abdullah AliemraanCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd