You might also like
- Breakdown Intimation SlipDocument1 pageBreakdown Intimation Slipvirender thakur75% (4)
- 004-JSA Manual WeldingDocument6 pages004-JSA Manual WeldingMoaatazz NouisriNo ratings yet
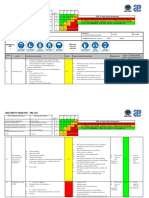
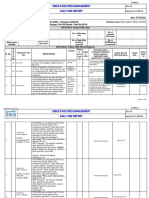
- Job Safety Analysis - Tbl-Jsa: STEP 4: Hazard Risk AssessmentDocument5 pagesJob Safety Analysis - Tbl-Jsa: STEP 4: Hazard Risk AssessmentMoaatazz NouisriNo ratings yet
- 01 Incident Investigation Report FORM HSE-IIPDocument2 pages01 Incident Investigation Report FORM HSE-IIPHSE S4No ratings yet
- Safety Audit ChecklistDocument3 pagesSafety Audit ChecklistSaravana KumarNo ratings yet
- Weekly HSE Performance ReportDocument2 pagesWeekly HSE Performance ReportSaravana KumarNo ratings yet
- 002-JSA RoW Opening and Marking FinalDocument6 pages002-JSA RoW Opening and Marking FinalMoaatazz NouisriNo ratings yet
- Hand Tools Inspection ChecklistDocument2 pagesHand Tools Inspection ChecklistSaravana KumarNo ratings yet
- Weekly Monthly Performance Report - Jerin Sam KurianDocument5 pagesWeekly Monthly Performance Report - Jerin Sam Kurianjerin sam kurianNo ratings yet
- Induction Format BHELDocument1 pageInduction Format BHELMOJIBNo ratings yet
- HSE Activities Monthly ReportDocument1 pageHSE Activities Monthly ReportSaravana KumarNo ratings yet
- AsdssssDocument1 pageAsdssssAviects Avie JaroNo ratings yet
- Daily HSE ReportDocument5 pagesDaily HSE ReportSayeed MalikNo ratings yet
- Monthly HSE Statistics ReportDocument2 pagesMonthly HSE Statistics ReportSaravana KumarNo ratings yet
- Daily HSE ReportDocument4 pagesDaily HSE ReportSayeed MalikNo ratings yet
- Module-1-Emergency Preparedness and Safety ManagementDocument8 pagesModule-1-Emergency Preparedness and Safety ManagementGrace AngNo ratings yet
- RFA FormDocument2 pagesRFA FormRitche Lim BragaisNo ratings yet
- PEN00651-01 JTHB Hydraulic Breaker Operation and Maintenance ManualDocument94 pagesPEN00651-01 JTHB Hydraulic Breaker Operation and Maintenance ManualAlvaroValdebenitoValenzuela60% (5)
- Introduction To Safety in Chemical Process Industry PDFDocument136 pagesIntroduction To Safety in Chemical Process Industry PDFMireia MartíNo ratings yet
- XXX Traning Proposal LetterDocument1 pageXXX Traning Proposal LetterDMAN1982No ratings yet
- Daily HSE ReportDocument5 pagesDaily HSE ReportSayeed Malik100% (1)
- JHA Alu Facade Installation Elevated Station-NewDocument22 pagesJHA Alu Facade Installation Elevated Station-NewnoorNo ratings yet
- Near Miss ReportDocument1 pageNear Miss ReportSaravana KumarNo ratings yet
- Toolbox Meeting Checklist: Sub-See Philippines IncDocument1 pageToolbox Meeting Checklist: Sub-See Philippines IncDanilo OralNo ratings yet
- ICS 207 Incident Organization ChartDocument1 pageICS 207 Incident Organization ChartMesosphere W.L.LNo ratings yet
- Preliminary Hazard AnalysisDocument26 pagesPreliminary Hazard AnalysisShahadat HossainNo ratings yet
- QRQC / 8D Form: D 1. Description of The ProblemDocument5 pagesQRQC / 8D Form: D 1. Description of The ProblemDearRed FrankNo ratings yet
- RFA FormDocument2 pagesRFA FormRalph TarrojaNo ratings yet
- TVL - He - Housekeeping: Guest Orientation On House RulesDocument20 pagesTVL - He - Housekeeping: Guest Orientation On House Rulesjowindel mandabonNo ratings yet
- Weekly Incident ReportDocument2 pagesWeekly Incident ReportBorislav VulićNo ratings yet
- Curriculum Map-Tle 9Document17 pagesCurriculum Map-Tle 9Regina Minguez Sabanal100% (5)
- SIEMENS Sinamics Perfect Harmony gh180 Catalog d17 Global 2018 PDFDocument75 pagesSIEMENS Sinamics Perfect Harmony gh180 Catalog d17 Global 2018 PDFJavier AriasNo ratings yet
- Machine Reliability and Condition Monitoring: A Comprehensive Guide to Predictive Maintenance PlanningFrom EverandMachine Reliability and Condition Monitoring: A Comprehensive Guide to Predictive Maintenance PlanningRating: 4.5 out of 5 stars4.5/5 (2)
- Development of Safety Culture Interaction Model For Construction ProjectsDocument12 pagesDevelopment of Safety Culture Interaction Model For Construction Projectshalisa kurniatiNo ratings yet
- FM-NC-01 NonConformanceDocument1 pageFM-NC-01 NonConformancesajjad abdullahNo ratings yet
- 3) Daily KY TrainingDocument2 pages3) Daily KY TrainingNitesh KumarNo ratings yet
- Incident Investigation Report - 21st Sep' 2021Document2 pagesIncident Investigation Report - 21st Sep' 2021SAHADEO REDDYNo ratings yet
- 09 - Monthly Hse ReportDocument1 page09 - Monthly Hse ReportMohamed RizwanNo ratings yet
- FORM 08 - Intervention Report - CRANK SHEAR - Copie - CopieDocument2 pagesFORM 08 - Intervention Report - CRANK SHEAR - Copie - CopieRamy Hassan EmaraNo ratings yet
- Flush Report - TemplateDocument1 pageFlush Report - TemplatevfuntanillaNo ratings yet
- IMSP 10 - 01 Flash Report-Communication of IncidentDocument2 pagesIMSP 10 - 01 Flash Report-Communication of IncidentMichael RujuwaNo ratings yet
- Incident Investigation ReportDocument4 pagesIncident Investigation ReportZohaib TahirNo ratings yet
- 02 - Incident Investigation Report - 9th Apr' 2021Document2 pages02 - Incident Investigation Report - 9th Apr' 2021SAHADEO REDDYNo ratings yet
- Cm-Mech - (42 To 43) - Send To MGPS at ( 27-07-2020)Document2 pagesCm-Mech - (42 To 43) - Send To MGPS at ( 27-07-2020)ali morisyNo ratings yet
- Incident Investigation ReportDocument4 pagesIncident Investigation ReportZohaib TahirNo ratings yet
- 5-Monthly Hse ReportDocument1 page5-Monthly Hse ReportMohamed RizwanNo ratings yet
- 3) Daily KY TrainingDocument2 pages3) Daily KY TrainingNitesh KumarNo ratings yet
- Intervention Report (Trouble) : Page: 1/1 Review Date: 17/12/2020 Redaction Date: 22/10/2019 Reference: PS1-FORM-08Document1 pageIntervention Report (Trouble) : Page: 1/1 Review Date: 17/12/2020 Redaction Date: 22/10/2019 Reference: PS1-FORM-08Ramy Hassan EmaraNo ratings yet
- Cm-Inst - (23 To 24) - Send To MGPS at ( 27-07-2020)Document2 pagesCm-Inst - (23 To 24) - Send To MGPS at ( 27-07-2020)ali morisyNo ratings yet
- NCR-Corrective & Preventive Action RequestDocument2 pagesNCR-Corrective & Preventive Action RequestRakesh SidhuNo ratings yet
- P20028 CP01 NCN 087 22Document5 pagesP20028 CP01 NCN 087 22Gridlines Bloom Residences Ph 1No ratings yet
- PRI-HSE-FRM-002 Weekly HSE ReportDocument1 pagePRI-HSE-FRM-002 Weekly HSE ReportTopeNo ratings yet
- CM-ELEC - (61 and 73) - SEND TO MGPS AT (04-11-2020) ReprintDocument2 pagesCM-ELEC - (61 and 73) - SEND TO MGPS AT (04-11-2020) Reprintali morisyNo ratings yet
- P20028 CP01 NCN 085 22Document3 pagesP20028 CP01 NCN 085 22Gridlines Bloom Residences Ph 1No ratings yet
- S200 Acifm MNT 50 RPT XXXXXXX 01080Document2 pagesS200 Acifm MNT 50 RPT XXXXXXX 01080fayasibrahimkuttyNo ratings yet
- HSE FRM-12 Weekly HSE ReportDocument1 pageHSE FRM-12 Weekly HSE ReportChecep SuyantoNo ratings yet
- Monthly Injury Record-SiteDocument1 pageMonthly Injury Record-SiteMR. MANTU DWIVEDINo ratings yet
- Laporan Manhours Periode April 2021Document3 pagesLaporan Manhours Periode April 2021HSE HSENo ratings yet
- Forms 1Document22 pagesForms 1jonathan ebajoNo ratings yet
- Annex 11 Non Compliance Traitement Sheet 23-05-2022Document1 pageAnnex 11 Non Compliance Traitement Sheet 23-05-2022vigoNo ratings yet
- NC TemplateDocument1 pageNC TemplateSupun ChanakaNo ratings yet
- Accident ReportDocument3 pagesAccident ReportEko SpdNo ratings yet
- Cm-Elec - (53 To 55) - Send To MGPS at (23-08-2020)Document3 pagesCm-Elec - (53 To 55) - Send To MGPS at (23-08-2020)ali morisyNo ratings yet
- Sor 01Document7 pagesSor 01Cherrycherry BetonioNo ratings yet
- Boot Dross Processing Facility, Project at RAK & Early Start Jubail PlantDocument4 pagesBoot Dross Processing Facility, Project at RAK & Early Start Jubail PlantElavarasan JayachandranNo ratings yet
- FRM-SLC-001 Safety Incident ReportDocument3 pagesFRM-SLC-001 Safety Incident ReportJNo ratings yet
- URM-0819-098-MA - Cover - Warping - Condition - KDC-X7200DABEN MA12Document7 pagesURM-0819-098-MA - Cover - Warping - Condition - KDC-X7200DABEN MA12Sahid Nugroho WNo ratings yet
- FORM 08 - Intervention Report - Cold SHEAR ClutchDocument2 pagesFORM 08 - Intervention Report - Cold SHEAR ClutchRamy Hassan EmaraNo ratings yet
- Cm-Mech - (49 To 50) - Send To MGPS at (13-08-2020)Document3 pagesCm-Mech - (49 To 50) - Send To MGPS at (13-08-2020)ali morisyNo ratings yet
- Analisis Técnico Causa Raiz Fallo Freno de Hoist 2 RTG 710Document4 pagesAnalisis Técnico Causa Raiz Fallo Freno de Hoist 2 RTG 710JUAN FELIPE CASTRO GONZALEZNo ratings yet
- Dcrj-Riy3-Material Submittal For CCTV System-01-231130Document1 pageDcrj-Riy3-Material Submittal For CCTV System-01-231130Ahmed AdelNo ratings yet
- Cm-Elec - (41 To 45) - Send To MGPS at (16-03-2021)Document5 pagesCm-Elec - (41 To 45) - Send To MGPS at (16-03-2021)Ali AlmorisyNo ratings yet
- BSD - 022 Compressed Gas Cylinder - HandlingDocument3 pagesBSD - 022 Compressed Gas Cylinder - HandlingZakkaudin KhanNo ratings yet
- BSD - 016 Block MachineDocument4 pagesBSD - 016 Block MachineZakkaudin KhanNo ratings yet
- P20028 CP01 NCN 086 22Document3 pagesP20028 CP01 NCN 086 22Gridlines Bloom Residences Ph 1No ratings yet
- Cm-Elec - (51 To 51) - Send To MGPS at (12-08-2020)Document1 pageCm-Elec - (51 To 51) - Send To MGPS at (12-08-2020)ali morisyNo ratings yet
- Safe Worker Assessment CriteriaDocument1 pageSafe Worker Assessment CriteriaSaravana KumarNo ratings yet
- Fire FightingDocument1 pageFire FightingSaravana KumarNo ratings yet
- Electrical Leads Sockets Plugs Inspection ChecklistDocument2 pagesElectrical Leads Sockets Plugs Inspection ChecklistSaravana KumarNo ratings yet
- Toilet ChecklistDocument1 pageToilet ChecklistSaravana KumarNo ratings yet
- The 10 Golden Rules of GMPDocument5 pagesThe 10 Golden Rules of GMPSabbir HossainNo ratings yet
- Summer Training Report On Nakoda LTDDocument82 pagesSummer Training Report On Nakoda LTDSanup SimonNo ratings yet
- Mocha 0046-5Document5 pagesMocha 0046-5Manoj Lalita GoswamiNo ratings yet
- JSA Painting Aut Tranformer Unit 3 OutageDocument7 pagesJSA Painting Aut Tranformer Unit 3 OutageMarhendraNo ratings yet
- Unit-3 Fire ProtectionDocument39 pagesUnit-3 Fire Protectionpmovie194No ratings yet
- Safety Data Sheet: G2980 Heavy Duty Headlight Restoration KitDocument28 pagesSafety Data Sheet: G2980 Heavy Duty Headlight Restoration KitStacy WoodsNo ratings yet
- Lowering of Materials by Single HydraDocument1 pageLowering of Materials by Single HydraJack PNo ratings yet
- Ergonomic Hazards ChecklistDocument3 pagesErgonomic Hazards ChecklistRui AraujoNo ratings yet
- OHS Legal AND Other External Requirements Procedure: ScopeDocument3 pagesOHS Legal AND Other External Requirements Procedure: ScopeKoshalNo ratings yet
- 3HAC052982 PS IRB 14000-EnDocument126 pages3HAC052982 PS IRB 14000-EnJosé Manuel MoaNo ratings yet
- Safety Data Sheet: 1. IdentificationDocument7 pagesSafety Data Sheet: 1. IdentificationJose CuellarNo ratings yet
- Simatic Ipc 547JDocument202 pagesSimatic Ipc 547JJdar WarakronNo ratings yet
- AGRT04-19 - Guide To Road Tunnels - Part 4 - Retrofitting TunnelsDocument60 pagesAGRT04-19 - Guide To Road Tunnels - Part 4 - Retrofitting TunnelsLeventNo ratings yet
- Dubai Municipality Requirement For Training and Consultancy Programs in Food SafetyDocument14 pagesDubai Municipality Requirement For Training and Consultancy Programs in Food SafetyMohamed Mohzin GhouseNo ratings yet
- Report Format - OIP-2021 - Format-1Document46 pagesReport Format - OIP-2021 - Format-1Pranay Ikkurthy100% (1)
- PTW 2Document4 pagesPTW 2saqib11No ratings yet
- Guide For The Meatpacking Industry: U.S. Department of Labor Occupational Safety and Health Administration 1988Document16 pagesGuide For The Meatpacking Industry: U.S. Department of Labor Occupational Safety and Health Administration 1988Sheyda RBNo ratings yet
- ID FOI Greenfields Centre Health and Safety Audit Form 2016 20190702Document20 pagesID FOI Greenfields Centre Health and Safety Audit Form 2016 20190702Malefane Cortez TlatlaneNo ratings yet
- SCBA Wiki PDFDocument6 pagesSCBA Wiki PDFomar benounaNo ratings yet