You might also like
- Hernia, (Different Types) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHernia, (Different Types) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- 2nd Year All Clinicals AIMC AcademiaDocument64 pages2nd Year All Clinicals AIMC Academiasaleempanwar96No ratings yet
- HerniaDocument67 pagesHerniaياسر نعيم الربيعي100% (1)
- Abdominal HerniasDocument38 pagesAbdominal HerniasHafizah HoshniNo ratings yet
- Hernia CMEDocument28 pagesHernia CMEsantokh108No ratings yet
- Inguinoscrotal Swellings and Undescended TestisDocument115 pagesInguinoscrotal Swellings and Undescended Testissyirah99No ratings yet
- LEC 08-Hernia-Collective NotesDocument36 pagesLEC 08-Hernia-Collective NotesAmira NabilNo ratings yet
- Gyne ReflectionDocument18 pagesGyne ReflectionKC Dela RosaNo ratings yet
- HerniasDocument6 pagesHerniasYalin AbouhassiraNo ratings yet
- Abdominal Wall, Omentum, Mesentery and Retroperitoneum DR AsepkyDocument33 pagesAbdominal Wall, Omentum, Mesentery and Retroperitoneum DR Asepkyafwan fajriNo ratings yet
- Key PointsDocument34 pagesKey PointsSe YunNo ratings yet
- 13 Genital Tract InjuriesDocument100 pages13 Genital Tract InjuriesRana Vandana100% (1)
- HERNIADocument70 pagesHERNIAmwro789000No ratings yet
- Hernia: DR - Surender Singh DhankharDocument36 pagesHernia: DR - Surender Singh DhankharBharat BhushanNo ratings yet
- Gyne Case COCDocument37 pagesGyne Case COCLian BaylosisNo ratings yet
- HerniaDocument46 pagesHerniaZubairkhan SuraniNo ratings yet
- Guide to Hernias: Inguinal, Femoral, Ventral and Unusual TypesDocument27 pagesGuide to Hernias: Inguinal, Femoral, Ventral and Unusual TypesAdip Grimaldis MirandaNo ratings yet
- DDX Backpain & Lumbar Spine DisorderDocument97 pagesDDX Backpain & Lumbar Spine Disorderilabella315No ratings yet
- Everything You Need to Know About HerniasDocument47 pagesEverything You Need to Know About HerniasmalathiNo ratings yet
- Regions of Abdomen Anatomy ReviewerDocument6 pagesRegions of Abdomen Anatomy ReviewerRYABELLE JESUSA SANCHEZNo ratings yet
- HerniasDocument49 pagesHerniasAliNo ratings yet
- Hernia: Done by D1 GroupDocument47 pagesHernia: Done by D1 Groupanindyadputri100% (1)
- Anorectal Malformation New 2024Document34 pagesAnorectal Malformation New 2024Urologi RSunudNo ratings yet
- UP PGH 2019 Interns Review 1 Benign GyneDocument152 pagesUP PGH 2019 Interns Review 1 Benign GyneTrisNo ratings yet
- لقطة شاشة ٢٠٢٣-١٠-٢٨ في ٦.٢٩.٥٩ صDocument115 pagesلقطة شاشة ٢٠٢٣-١٠-٢٨ في ٦.٢٩.٥٩ صhNo ratings yet
- Inguinal Hernia: From Wikipedia, The Free EncyclopediaDocument6 pagesInguinal Hernia: From Wikipedia, The Free EncyclopediaSherlyn YeeNo ratings yet
- Anatomy Block 3Document16 pagesAnatomy Block 3Eslie NájeraNo ratings yet
- External HerniaDocument136 pagesExternal Herniasanjivdas100% (1)
- LANLUMA Abdomen Protocol - Final VersionDocument25 pagesLANLUMA Abdomen Protocol - Final Versionsyeda tahreemunisaNo ratings yet
- Anal, Perianal, and Pilonidal Diseases - Oct - 2023 2Document15 pagesAnal, Perianal, and Pilonidal Diseases - Oct - 2023 2qq8kx98kt2No ratings yet
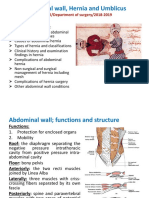
- Abdominal Wall, Hernia and Umblicus: M Kamil/Department of Surgery/2018-2019Document46 pagesAbdominal Wall, Hernia and Umblicus: M Kamil/Department of Surgery/2018-2019AmmarNo ratings yet
- General Consideration Inguinal Hernias: Femoral Hernia Incisional Hernia Umbilial Hernia Hernia of Linea AlbaDocument30 pagesGeneral Consideration Inguinal Hernias: Femoral Hernia Incisional Hernia Umbilial Hernia Hernia of Linea Albainna3003No ratings yet
- SUPPORTS OF UTERUS ShilpaDocument61 pagesSUPPORTS OF UTERUS ShilpaSreelasya83% (6)
- CASE PRESENTATION Nadhirah RahimDocument60 pagesCASE PRESENTATION Nadhirah RahimNadhirah Rahim100% (1)
- Hernia Seminar 2 Aug 2014 FinalDocument20 pagesHernia Seminar 2 Aug 2014 FinalKishan NaiduNo ratings yet
- Inguinal Hernia PresentationDocument23 pagesInguinal Hernia PresentationReema Haji AbdullahNo ratings yet
- Dinding Abdomen PSIKDocument79 pagesDinding Abdomen PSIKSondang DamanikNo ratings yet
- Anatomy and Conditions of the Anal Canal/TITLEDocument59 pagesAnatomy and Conditions of the Anal Canal/TITLELulu ShukkoorNo ratings yet
- Wa0000. 1Document41 pagesWa0000. 1Aditya SinghNo ratings yet
- Cro DiseaseDocument82 pagesCro DiseaseБаяржавхлан СүхбаатарNo ratings yet
- Abdominal Wall Hernia GuideDocument35 pagesAbdominal Wall Hernia GuideMohammad BanisalmanNo ratings yet
- HerniaDocument36 pagesHerniashankarrao3No ratings yet
- Muscles of MasticationDocument112 pagesMuscles of MasticationEazhil RajNo ratings yet
- Hernia and Perianal ConditionsDocument58 pagesHernia and Perianal ConditionsSocial Media workingNo ratings yet
- DK Case 7 WrapDocument13 pagesDK Case 7 WrapSomaNo ratings yet
- 1 - OB 1 (Maternal Anatomy)Document13 pages1 - OB 1 (Maternal Anatomy)Gen XNo ratings yet
- Hernia: RSST Klaten Koas Stase Bedah A13.1Document54 pagesHernia: RSST Klaten Koas Stase Bedah A13.1Bagus WirayudaNo ratings yet
- Anatomy of Epidural Space: Dr. M.Suguna Dept. of Anesthesia GTMC-TheniDocument33 pagesAnatomy of Epidural Space: Dr. M.Suguna Dept. of Anesthesia GTMC-TheniPrabha KaranNo ratings yet
- CH 19 Spinal AnaesthesiaDocument29 pagesCH 19 Spinal AnaesthesiaChristian Leepo100% (1)
- Disorder of Lower LimbDocument76 pagesDisorder of Lower Limb074 Khola WaqarNo ratings yet
- Muscles of MasticationDocument43 pagesMuscles of Masticationchaitree100% (1)
- Inguinal Hernia FinalDocument42 pagesInguinal Hernia FinalRajath Kumar K R KNo ratings yet
- LarynxDocument5 pagesLarynxGeraldine Marie SalvoNo ratings yet
- GIT Cont 071628Document51 pagesGIT Cont 071628Olatomide OlaniranNo ratings yet
- HerniaDocument12 pagesHerniaAdelia Maharani DNo ratings yet
- Imaging Anatomy Musculoskeletal (B. J. Manaster, Julia Crim) (Z-Lib - Org) Split-Merge - extractPDFpagesDocument12 pagesImaging Anatomy Musculoskeletal (B. J. Manaster, Julia Crim) (Z-Lib - Org) Split-Merge - extractPDFpagesChristian ToalongoNo ratings yet
- Abdominal Hernias: Member of A Medical Scheme? Know Your Guaranteed Benefits!Document3 pagesAbdominal Hernias: Member of A Medical Scheme? Know Your Guaranteed Benefits!Annisa KimNo ratings yet
- HerniaDocument100 pagesHerniaangelaanapaku100% (3)
- Groin Hernia and Scrotal Mass GuideDocument82 pagesGroin Hernia and Scrotal Mass GuideJJ JirapathNo ratings yet
- HerniaDocument11 pagesHerniaHapsari Wibawani 'winda'100% (1)
- HERNIADocument34 pagesHERNIAAtiqah ShahNo ratings yet
- Part 2.herniaDocument38 pagesPart 2.herniaapi-19641337No ratings yet
- Hernias UltrasoundDocument35 pagesHernias UltrasoundRafa Rodríguez AveigaNo ratings yet
- Everything You Need to Know About Hernia Types and SymptomsDocument47 pagesEverything You Need to Know About Hernia Types and SymptomsPhuntsho OngmoNo ratings yet
- (Artigo) Groin Hernias in Adults Solomon. (2015)Document8 pages(Artigo) Groin Hernias in Adults Solomon. (2015)Beatriz BelottiNo ratings yet
- Thesis On HerniaDocument6 pagesThesis On Herniasunshineblackburnhayward100% (2)
- Hernias Types and TreatmentDocument19 pagesHernias Types and Treatmenthussain AltaherNo ratings yet
- Femoral CanalDocument2 pagesFemoral CanalHassan MohamedNo ratings yet
- Types of HerniasDocument12 pagesTypes of HerniasAudrey100% (4)
- Laparoscopic Inguinal and Femoral Hernia Repair in Adults - UpToDateDocument22 pagesLaparoscopic Inguinal and Femoral Hernia Repair in Adults - UpToDategdi3No ratings yet
- Abdominal Wall HerniasDocument29 pagesAbdominal Wall Herniasbunny_totsNo ratings yet
- Hernia Types and DiagnosisDocument47 pagesHernia Types and DiagnosisteamirNo ratings yet
- ERN Intercoll MRCS Bk2Document48 pagesERN Intercoll MRCS Bk2Rocita HoNo ratings yet
- Inguinal Hernia - Knowledge at AMBOSSDocument1 pageInguinal Hernia - Knowledge at AMBOSSEstellaNo ratings yet
- Hernia FinalDocument21 pagesHernia FinalYeoh Shu TingNo ratings yet
- Hernia Ebook FullDocument24 pagesHernia Ebook FullMiguelon GarciaNo ratings yet
- Diagnosis Icd X Tindakan Icd 9 CMDocument8 pagesDiagnosis Icd X Tindakan Icd 9 CMlinaNo ratings yet
- 5 HerniaDocument5 pages5 HerniaFarhinNo ratings yet
- Hernia CaseDocument9 pagesHernia CaseFatima Love Ariate-Arcasetas100% (1)
- GIT DisordersDocument171 pagesGIT DisordersKatrina PonceNo ratings yet
- Sample: Pediatric Hernia Inguinal and Femoral RepairDocument8 pagesSample: Pediatric Hernia Inguinal and Femoral RepairSamuel Sebastian SirapanjiNo ratings yet
- HerniaDocument16 pagesHerniamuhammad akbarNo ratings yet
- Femoral Hernia - A Review of Clinical AnatomyDocument6 pagesFemoral Hernia - A Review of Clinical AnatomyFatur RasyidNo ratings yet
- General Surgery OME PDFDocument25 pagesGeneral Surgery OME PDFNathan Korean KimNo ratings yet
- Femoral Hernia. The SAGES Manual of Hernia Repair.Document12 pagesFemoral Hernia. The SAGES Manual of Hernia Repair.Eri ContrerasNo ratings yet
- The Abdomen 98 QDocument78 pagesThe Abdomen 98 QNahidNo ratings yet
- Different Eponymous Types of HerniaDocument3 pagesDifferent Eponymous Types of HerniaNizam Mischievous'Lovely Schremo BoyysNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (17)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (403)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Algorithms to Live By: The Computer Science of Human DecisionsFrom EverandAlgorithms to Live By: The Computer Science of Human DecisionsRating: 4.5 out of 5 stars4.5/5 (722)
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)