You might also like
- Envolvimento ComunitarioDocument13 pagesEnvolvimento Comunitariosaude publica71% (7)
- Arterial Blood Gas Interpretation – A case study approachFrom EverandArterial Blood Gas Interpretation – A case study approachRating: 1 out of 5 stars1/5 (1)
- Respiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsFrom EverandRespiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsJian-Xin ZhouNo ratings yet
- High Flow Nasal Cannula: Physiological Effects and Clinical ApplicationsFrom EverandHigh Flow Nasal Cannula: Physiological Effects and Clinical ApplicationsAnnalisa CarlucciNo ratings yet
- Medical Mnemonic Sketches : Pulmonary DiseasesFrom EverandMedical Mnemonic Sketches : Pulmonary DiseasesNo ratings yet
- THE BUTEYKO METHOD (Translated): The secret of controlled breathing for health, well-being and vitalityFrom EverandTHE BUTEYKO METHOD (Translated): The secret of controlled breathing for health, well-being and vitalityNo ratings yet
- Pulmonary Function Tests in Clinical PracticeFrom EverandPulmonary Function Tests in Clinical PracticeAli AltalagRating: 5 out of 5 stars5/5 (1)
- Hyperbaric Oxygenation Therapy: Molecular Mechanisms and Clinical ApplicationsFrom EverandHyperbaric Oxygenation Therapy: Molecular Mechanisms and Clinical ApplicationsNariyoshi ShinomiyaNo ratings yet
- Diagnosis and Treatment of Neurogenic Oropharyngeal DysphagiaFrom EverandDiagnosis and Treatment of Neurogenic Oropharyngeal DysphagiaNo ratings yet
- Orthodontics in Obstructive Sleep Apnea Patients: A Guide to Diagnosis, Treatment Planning, and InterventionsFrom EverandOrthodontics in Obstructive Sleep Apnea Patients: A Guide to Diagnosis, Treatment Planning, and InterventionsSu-Jung KimNo ratings yet
- Diagnosis and Treatment of Chronic CoughFrom EverandDiagnosis and Treatment of Chronic CoughSang Heon ChoNo ratings yet
- Pulmonary Endocrine Pathology: Endocrine Cells and Endocrine Tumours of the LungFrom EverandPulmonary Endocrine Pathology: Endocrine Cells and Endocrine Tumours of the LungNo ratings yet
- Obstructive Sleep Apnea, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandObstructive Sleep Apnea, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 3 out of 5 stars3/5 (2)
- Snoring, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandSnoring, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Laryngopharyngeal and Gastroesophageal Reflux: A Comprehensive Guide to Diagnosis, Treatment, and Diet-Based ApproachesFrom EverandLaryngopharyngeal and Gastroesophageal Reflux: A Comprehensive Guide to Diagnosis, Treatment, and Diet-Based ApproachesCraig H. ZalvanNo ratings yet
- Fast Facts: Excessive Daytime Sleepiness Associated with Obstructive Sleep ApneaFrom EverandFast Facts: Excessive Daytime Sleepiness Associated with Obstructive Sleep ApneaNo ratings yet
- Fast Facts: Asthma: Improve patient self-management and drug use, achieve asthma controlFrom EverandFast Facts: Asthma: Improve patient self-management and drug use, achieve asthma controlNo ratings yet
- Basics and modern practice of nasal high-flow therapyFrom EverandBasics and modern practice of nasal high-flow therapyRating: 5 out of 5 stars5/5 (1)
- Asthma: Symptoms, Treatments, and Medication for Asthma and BronchitisFrom EverandAsthma: Symptoms, Treatments, and Medication for Asthma and BronchitisNo ratings yet
- Respiration and EmotionFrom EverandRespiration and EmotionY. HarukiNo ratings yet
- Biological and Environmental Effects of ArsenicFrom EverandBiological and Environmental Effects of ArsenicB.A. FowlerNo ratings yet
- Laryngopharyngeal Reflux, A Simple Guide to the Condition, Treatment and Related DiseasesFrom EverandLaryngopharyngeal Reflux, A Simple Guide to the Condition, Treatment and Related DiseasesRating: 3.5 out of 5 stars3.5/5 (2)
- Congenital Cystic Lung Disease: Comprehensive Understanding of its Diagnosis and Treatment from Fetus to ChildhoodFrom EverandCongenital Cystic Lung Disease: Comprehensive Understanding of its Diagnosis and Treatment from Fetus to ChildhoodHaruhiko SagoNo ratings yet
- Metabolic Disorders and Critically Ill Patients: From Pathophysiology to TreatmentFrom EverandMetabolic Disorders and Critically Ill Patients: From Pathophysiology to TreatmentCarole IchaiNo ratings yet
- Modern Anaesthesia:: A Concise Guide to the Study and Practice of Anaesthesia.From EverandModern Anaesthesia:: A Concise Guide to the Study and Practice of Anaesthesia.No ratings yet
- A Simple Guide to Oxygen Therapy, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Oxygen Therapy, Diagnosis, Treatment and Related ConditionsNo ratings yet
- How To Purchase Activate and Check Day Pass Withdesign v3Document15 pagesHow To Purchase Activate and Check Day Pass Withdesign v3leo chiuNo ratings yet
- Participation Terms Sankakiyaku JapaneseDocument5 pagesParticipation Terms Sankakiyaku Japaneseleo chiuNo ratings yet
- Specifications: Selectsecure Mri Surescan 3830 LeadDocument2 pagesSpecifications: Selectsecure Mri Surescan 3830 Leadleo chiuNo ratings yet
- 打針攻略+常見問題 (7 14版本)Document14 pages打針攻略+常見問題 (7 14版本)leo chiuNo ratings yet
- TYRX BrochureDocument28 pagesTYRX Brochureleo chiuNo ratings yet
- HKSME - 疫苗優惠懶人包Document29 pagesHKSME - 疫苗優惠懶人包leo chiuNo ratings yet
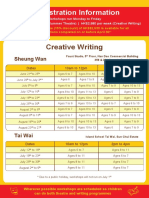
- Summer Programme Schedule 2021Document6 pagesSummer Programme Schedule 2021leo chiuNo ratings yet
- BMW Concessionaires (HK) Limited: Hong Kong Price List For 2021 New BMW Models JUL 2021aDocument2 pagesBMW Concessionaires (HK) Limited: Hong Kong Price List For 2021 New BMW Models JUL 2021aleo chiuNo ratings yet
- BusinessDocument49 pagesBusinessleo chiuNo ratings yet
- Blood Gas AnalyzerDocument1 pageBlood Gas Analyzerleo chiuNo ratings yet
- Initiation and Maintenance of Labour Analgesia: Epidural or CSE, Bolus or Infusion?Document32 pagesInitiation and Maintenance of Labour Analgesia: Epidural or CSE, Bolus or Infusion?leo chiuNo ratings yet
- 活頁簿1Document1 page活頁簿1leo chiuNo ratings yet
- Suma Plaq MSDS 2019Document10 pagesSuma Plaq MSDS 2019Victor Javier Santibañez BarralesNo ratings yet
- IELTS Academic Reading 5Document5 pagesIELTS Academic Reading 5Hương ThuNo ratings yet
- Made 407Document5 pagesMade 407tu nguyen thiNo ratings yet
- By: Dr. Shkar R. SaeedDocument45 pagesBy: Dr. Shkar R. SaeedSimon JosanNo ratings yet
- Jamu Herb Guide Info On Individual HerbsDocument4 pagesJamu Herb Guide Info On Individual HerbsLinda PrideNo ratings yet
- Full SourcesDocument4 pagesFull Sourcesapi-583958001No ratings yet
- A World AT: Annual Report On Global Preparedness For Health EmergenciesDocument48 pagesA World AT: Annual Report On Global Preparedness For Health EmergenciesWeb AdevarulNo ratings yet
- LungtengB3L1Reading and Voc (The Day I Broke the Rules) 1120816單字及課本句型答案Document88 pagesLungtengB3L1Reading and Voc (The Day I Broke the Rules) 1120816單字及課本句型答案雷佳惠No ratings yet
- ENFRMEDAD DIARREICA AGUDA Diapos EnvDocument20 pagesENFRMEDAD DIARREICA AGUDA Diapos EnvAngie AndradeNo ratings yet
- ANEXO 6 - DVC-SSOMA-SG-PG-009 Requisitos de Ingreso A Obra para Subcontratistas Ver.03Document9 pagesANEXO 6 - DVC-SSOMA-SG-PG-009 Requisitos de Ingreso A Obra para Subcontratistas Ver.03carlosNo ratings yet
- Trabajo FinalDocument17 pagesTrabajo FinalFrancisco GabrielNo ratings yet
- Drug Control and Enforcement ActDocument82 pagesDrug Control and Enforcement ActTito MnyenyelwaNo ratings yet
- Las Plantas Fabrican Su Propio Alimento CAÑALDocument9 pagesLas Plantas Fabrican Su Propio Alimento CAÑALPaola Baranda Kltz'No ratings yet
- Behavioral Science - Case StudyDocument3 pagesBehavioral Science - Case StudyYolo GuyNo ratings yet
- Autoevaluacion NutriciónDocument3 pagesAutoevaluacion Nutricióncarla sandovalNo ratings yet
- Violencia en El Enamoramiento PresentacionDocument24 pagesViolencia en El Enamoramiento PresentacionJaime Adriano Canchuricra100% (1)
- Los MedicosDocument14 pagesLos MedicosThyare GaleasNo ratings yet
- Resumeen de AnemiaDocument4 pagesResumeen de Anemiastefany trujilloNo ratings yet
- Relación Histórica Entre El Sujeto y La Droga DrogaDocument18 pagesRelación Histórica Entre El Sujeto y La Droga DrogaPAULA CATERINE BRAVO MORENONo ratings yet
- 7931 Pgsst-004 Programa de Inspecciones de SeguridadDocument12 pages7931 Pgsst-004 Programa de Inspecciones de SeguridadCristian Andres Lloreda Mosquera100% (1)
- "Los Aportes de La Neurociencia A La Atención y Educación de La Primera InfanciaDocument7 pages"Los Aportes de La Neurociencia A La Atención y Educación de La Primera InfanciaAlejandra SanchezNo ratings yet
- Guía TamizDocument4 pagesGuía TamizFlor SFNo ratings yet
- Diccionario de Competencias Laborales AromasyntDocument33 pagesDiccionario de Competencias Laborales AromasyntKAROL DANIELA GIL VERANo ratings yet
- Sistema Inmune 5toDocument6 pagesSistema Inmune 5toJose HerreraNo ratings yet
- Prevenir Lesiones Durante La Actividad FisicaDocument3 pagesPrevenir Lesiones Durante La Actividad FisicalosmisteriosdemovilleNo ratings yet
- DE Thi HKI - 2019-2020 - TN - 11DDocument7 pagesDE Thi HKI - 2019-2020 - TN - 11DChi MaiNo ratings yet
- MA - Caminhos - para - Uma - Convivencia - Saudavel - Perspectiva - Saude 11out PDFDocument130 pagesMA - Caminhos - para - Uma - Convivencia - Saudavel - Perspectiva - Saude 11out PDFÁlex NogueiraNo ratings yet
- Commissions Lutte Contre La Grippe D'origine Aviaire-AlgérieDocument2 pagesCommissions Lutte Contre La Grippe D'origine Aviaire-AlgérieSim VetNo ratings yet
- T10606 - Diseño de Una Metodología para La Valoración Del Riesgo Ocupacional en Trabajadores Que Manipulan NanomaterialesDocument70 pagesT10606 - Diseño de Una Metodología para La Valoración Del Riesgo Ocupacional en Trabajadores Que Manipulan NanomaterialesCeleste FernandezNo ratings yet