You might also like
- Somatosensory Teachers Manual: for Somatosensory Science FactsFrom EverandSomatosensory Teachers Manual: for Somatosensory Science FactsNo ratings yet
- Power Lab - Index CardDocument5 pagesPower Lab - Index CardKate Alyssa CatonNo ratings yet
- DR - Sanyal Kumar JR Dept of PMRDocument25 pagesDR - Sanyal Kumar JR Dept of PMRjothiNo ratings yet
- Neuro Lab Physio Ex 6.0Document13 pagesNeuro Lab Physio Ex 6.0KevinDelaCruzNo ratings yet
- 02.neural Lectures Prof - Wilm.neural Lectures - Prof - WilmoreoreDocument19 pages02.neural Lectures Prof - Wilm.neural Lectures - Prof - WilmoreoreManu NedeleaNo ratings yet
- Lab 4Document12 pagesLab 4api-251827644No ratings yet
- Action Potential: Daniela Ayala Grand Canyon UniversityDocument12 pagesAction Potential: Daniela Ayala Grand Canyon Universitydaniela ayalaNo ratings yet
- Biology 30 Student Notes Nervous ReproductionDocument53 pagesBiology 30 Student Notes Nervous ReproductionDennis Limosnero MayorNo ratings yet
- Physiology 3 (Nerve)Document29 pagesPhysiology 3 (Nerve)eman el saeedNo ratings yet
- Nerve Muscle PhysiologyDocument18 pagesNerve Muscle PhysiologyDr P N N Reddy100% (2)
- Unit 8 Learning Guide Name: Brandon Au-Young: InstructionsDocument25 pagesUnit 8 Learning Guide Name: Brandon Au-Young: InstructionsBrandonNo ratings yet
- Neuromuscular JunctionDocument10 pagesNeuromuscular JunctionAfeefuddin ShaikhNo ratings yet
- Lab Exercise 3Document3 pagesLab Exercise 3amarNo ratings yet
- Nerve Conduction NeurobiomechanicsDocument25 pagesNerve Conduction NeurobiomechanicscutinhawayneNo ratings yet
- Nervous System 2Document28 pagesNervous System 2Farina FaraziNo ratings yet
- Aniphys Lab Report 1Document15 pagesAniphys Lab Report 1kristiane93100% (2)
- 2022 Set-EXCITABLE TISSUES Membrane Potential & NeuronsDocument53 pages2022 Set-EXCITABLE TISSUES Membrane Potential & NeuronsSamuel BenjaminNo ratings yet
- What Is Ncs ?Document42 pagesWhat Is Ncs ?rabeyaNo ratings yet
- Nerve Muscle PhysiologyDocument67 pagesNerve Muscle PhysiologyPlutokidNo ratings yet
- M3 L1 Check-In ActivityDocument3 pagesM3 L1 Check-In ActivityZHAREIGHNEILE C. MAMOLONo ratings yet
- Properties of Nerve FibresDocument15 pagesProperties of Nerve Fibresdandasenasourabh1No ratings yet
- Cardiovascular Physiology Review QuestionsDocument44 pagesCardiovascular Physiology Review QuestionsTim100% (1)
- Nerve PhysiologyDocument31 pagesNerve Physiologynirilib100% (4)
- 03 A Microstim DBS Grp12Document24 pages03 A Microstim DBS Grp12burnerbharadwajNo ratings yet
- Squid Lab Packet v3Document8 pagesSquid Lab Packet v3Bradley Chung100% (1)
- RSC Nervous SystemDocument5 pagesRSC Nervous SystemDurre shahwarNo ratings yet
- Simple Muscle Twitch: Excitable TissueDocument26 pagesSimple Muscle Twitch: Excitable Tissueسليمان فايزNo ratings yet
- Axon ReflexDocument38 pagesAxon ReflexKamalakannanNo ratings yet
- Galvano Terapy Topic - 6Document3 pagesGalvano Terapy Topic - 6Gigi CotoraNo ratings yet
- Neuromuscular Junction by Dr. RoomiDocument20 pagesNeuromuscular Junction by Dr. RoomiMudassar Roomi100% (1)
- 3 Nerve and Muscle. (New)Document28 pages3 Nerve and Muscle. (New)Ramadan Physiology100% (2)
- TOPIC 9 NERVOUS CONTROL My Notes 1Document11 pagesTOPIC 9 NERVOUS CONTROL My Notes 1shealtielchigariso06No ratings yet
- 01 Review of Physiology - Excitable Tissue Response of Electrical StimulationDocument2 pages01 Review of Physiology - Excitable Tissue Response of Electrical Stimulation楊畯凱No ratings yet
- Electrotherapy 1 Viva QuestionsDocument9 pagesElectrotherapy 1 Viva QuestionsAmaan Shafique100% (2)
- NURS1108 Lecture 9 - Nervous System ENHANCED 2019Document39 pagesNURS1108 Lecture 9 - Nervous System ENHANCED 2019Jacia’s SpaceshipNo ratings yet
- Exer 2 Nerve Conduction Final ShitDocument3 pagesExer 2 Nerve Conduction Final ShitJosephineCarandangNo ratings yet
- Experiment 3 - Frog NerveDocument29 pagesExperiment 3 - Frog NerveRachel CajilesNo ratings yet
- NB (019) An Introduction To Neurons and Communication Between Them UCL RevisedDocument38 pagesNB (019) An Introduction To Neurons and Communication Between Them UCL RevisedZeyad AmrNo ratings yet
- Leech Lab ReportDocument14 pagesLeech Lab Reportapi-339485098No ratings yet
- Low Frequency CurrentsDocument11 pagesLow Frequency CurrentsElias KangwaNo ratings yet
- Muscle Students NotesDocument7 pagesMuscle Students Notesrohitgaur210% (1)
- Neurohormonal Regulation of Body FunctionsDocument34 pagesNeurohormonal Regulation of Body FunctionsjimmyNo ratings yet
- Sensory Action Potentials in Patients With Peripheral Nerve LesionsDocument11 pagesSensory Action Potentials in Patients With Peripheral Nerve LesionsRenard ChristianNo ratings yet
- Biofact Sheet Nerves SynapsesDocument4 pagesBiofact Sheet Nerves SynapsesJonMortNo ratings yet
- Lecture On The Physiology of Neuromuscular Junction (NMJ) by Dr. RoomiDocument18 pagesLecture On The Physiology of Neuromuscular Junction (NMJ) by Dr. RoomiMudassar Roomi100% (3)
- A Review of Neuromuscular MonitoringDocument10 pagesA Review of Neuromuscular Monitoringdrcds99No ratings yet
- NeurophysicsDocument8 pagesNeurophysicsMakavana SahilNo ratings yet
- 22neurophysiology 2CVDocument79 pages22neurophysiology 2CVtNo ratings yet
- Sistem SarafDocument176 pagesSistem SarafRidza Allo LayukNo ratings yet
- Physiology Unit 4 - 231102 - 212048Document23 pagesPhysiology Unit 4 - 231102 - 212048SanchezNo ratings yet
- Exam Prep - Lec 3 - KEYDocument6 pagesExam Prep - Lec 3 - KEYAndrew ShiahNo ratings yet
- Fisiologi NeurofisiologiDocument60 pagesFisiologi NeurofisiologiShabrina Maharani100% (1)
- Quadriceps Muscle Weakness Following AcuteDocument8 pagesQuadriceps Muscle Weakness Following AcutePedro FonsecaNo ratings yet
- Activity 1: The Muscle Twitch and The Latent PeriodDocument10 pagesActivity 1: The Muscle Twitch and The Latent PeriodAndiena ElsafiraNo ratings yet
- Deep Tendon ReflexesDocument9 pagesDeep Tendon ReflexesSyairah Banu DjufriNo ratings yet
- Physiology Study Guide CH 7 Nervous System Neurons KeyDocument4 pagesPhysiology Study Guide CH 7 Nervous System Neurons KeyJamie SamuelNo ratings yet
- Department of Anatomy, Northwestern University Medical SchoolDocument19 pagesDepartment of Anatomy, Northwestern University Medical SchoolAde Dian KaruniaNo ratings yet
- Cns PhysiologyDocument152 pagesCns PhysiologyDr. Niyati Patel100% (1)
- ART20162812Document7 pagesART20162812sumathy ysNo ratings yet
- Monitoring of Neuromuscular Junction: Dr. D. Padmaja Dr. Srinivas ManthaDocument10 pagesMonitoring of Neuromuscular Junction: Dr. D. Padmaja Dr. Srinivas ManthakoolstaroneNo ratings yet
- Chemical Equilibrium and Le Chatelier's Principle: Chemistry 1Document17 pagesChemical Equilibrium and Le Chatelier's Principle: Chemistry 1azamatNo ratings yet
- Test On Gmos GM Foods Cloning b1b2 Grammar Drills Information Gap Activities Reading 96207Document4 pagesTest On Gmos GM Foods Cloning b1b2 Grammar Drills Information Gap Activities Reading 96207Thu Quynh NguyenNo ratings yet
- 6.1 MicrobiologyDocument32 pages6.1 MicrobiologyYsabelle BautistaNo ratings yet
- Question Bank Respiratory SystemDocument13 pagesQuestion Bank Respiratory SystemDK Meerut statusNo ratings yet
- Microscopy and StainingDocument7 pagesMicroscopy and StainingDenmark ManlusocNo ratings yet
- NCERT Class 3 English Baloon ManDocument10 pagesNCERT Class 3 English Baloon ManAnonymous 9WyPyismNo ratings yet
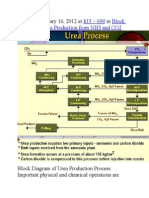
- Published January 16, 2012 at In: 813 × 699 Block Diagram of Urea Production From NH3 and CO2Document9 pagesPublished January 16, 2012 at In: 813 × 699 Block Diagram of Urea Production From NH3 and CO2himanshuchawla654No ratings yet
- Biosensors For Environmental ApplicationsDocument15 pagesBiosensors For Environmental ApplicationsBenjamin HonorioNo ratings yet
- EXPERIMENT 3.6: Determining The Concentration of An External Solution Which Is Isotonic To The Cell Sap of A PlantDocument2 pagesEXPERIMENT 3.6: Determining The Concentration of An External Solution Which Is Isotonic To The Cell Sap of A PlantAmsyidi AsmidaNo ratings yet
- Angiogenesis and Direct Myocardial RevascularizationDocument364 pagesAngiogenesis and Direct Myocardial RevascularizationPerdana SidaurukNo ratings yet
- Preliminary Experiment: Visual Observation and InterpretationDocument3 pagesPreliminary Experiment: Visual Observation and InterpretationRuchie Ann Pono BaraquilNo ratings yet
- CROSS TREE - Sorte I Selekcije Voćaka I Vinove Loze Iz Severozapadne Srbije I Istočne Hrvatske PDFDocument153 pagesCROSS TREE - Sorte I Selekcije Voćaka I Vinove Loze Iz Severozapadne Srbije I Istočne Hrvatske PDFrraattaarrrraattaaNo ratings yet
- Preparation of Histological SpecimensDocument4 pagesPreparation of Histological SpecimensAqilah HazwaniNo ratings yet
- Human Genetics Concepts and Applications 11Th Edition Ricki Lewis Test Bank Full Chapter PDFDocument36 pagesHuman Genetics Concepts and Applications 11Th Edition Ricki Lewis Test Bank Full Chapter PDFdavid.cordero230100% (14)
- Science of The Total Environment: Megan Carve Graeme Allinson, Dayanthi Nugegoda, Jeff ShimetaDocument16 pagesScience of The Total Environment: Megan Carve Graeme Allinson, Dayanthi Nugegoda, Jeff ShimetaFABIANA PASSAMANINo ratings yet
- RPT SC Year 2 (DLP) 2022-2023Document21 pagesRPT SC Year 2 (DLP) 2022-2023ANNIE MARGARET A/P ANTHONY MoeNo ratings yet
- High-Yield NephrologyDocument6 pagesHigh-Yield NephrologyAhmad SobihNo ratings yet
- Veterinary Gross Anatomy Female Genital TractDocument10 pagesVeterinary Gross Anatomy Female Genital TractTatenda MagejaNo ratings yet
- LPL - Amit Sharma FPSC Loni Road-Gzb Shop No-4, Saharanpur Road, Loni Road, Main Tiraha, Loni, Ghaziabad, Loni S.ODocument3 pagesLPL - Amit Sharma FPSC Loni Road-Gzb Shop No-4, Saharanpur Road, Loni Road, Main Tiraha, Loni, Ghaziabad, Loni S.OKaran PrabhakarNo ratings yet
- ABCD Vocal Technique Handout PDFDocument9 pagesABCD Vocal Technique Handout PDFRanieque RamosNo ratings yet
- 16S RRNA Gene Sequencing For Bacterial IdentificationDocument4 pages16S RRNA Gene Sequencing For Bacterial IdentificationBenjamin UcichNo ratings yet
- The Impact of Your Internal Terrain On Your FasciaDocument16 pagesThe Impact of Your Internal Terrain On Your Fasciazzip1961100% (1)
- Trabalho em Saúde e A Implantação Do Acolhimento Na Atenção Primária À Saúde - Afeto, Empatia Ou AlteridadeDocument13 pagesTrabalho em Saúde e A Implantação Do Acolhimento Na Atenção Primária À Saúde - Afeto, Empatia Ou AlteridadeAmérico PastorNo ratings yet
- Life Span: HumanDocument738 pagesLife Span: HumanWAJEEHA GOHARNo ratings yet
- Circulatory SystemDocument16 pagesCirculatory SystemHarinder KaurNo ratings yet
- 7 Pearson SquareDocument19 pages7 Pearson Squareapi-235944649No ratings yet
- Cham PowerpointDocument19 pagesCham PowerpointElizabeth GenotivaNo ratings yet
- Instant Download Business Communication 16th Edition Lehman Test Bank PDF Full ChapterDocument32 pagesInstant Download Business Communication 16th Edition Lehman Test Bank PDF Full Chapterarthrosisretake8hro100% (8)
- Nominalization (Exercise)Document2 pagesNominalization (Exercise)KryzQuinonesNo ratings yet
- MSDS Ecaro-25Document10 pagesMSDS Ecaro-25ValenteNo ratings yet