You might also like
- Money Saving Tips - A White Paper: Techniques I've Actually Used: Thinking About Money, #2From EverandMoney Saving Tips - A White Paper: Techniques I've Actually Used: Thinking About Money, #2No ratings yet
- DxwebDocument7 pagesDxwebjamespaulgilbertNo ratings yet
- Deduction StatementDocument4 pagesDeduction StatementAdam Di GiuseppeNo ratings yet
- Important Questions Answers Why This MattersDocument10 pagesImportant Questions Answers Why This MattersJunior GatbuntonNo ratings yet
- Important Questions Answers Why This MattersDocument10 pagesImportant Questions Answers Why This MattersbrineshrimpNo ratings yet
- Go Paperless: Your 2021 Rate and Benefit UpdateDocument5 pagesGo Paperless: Your 2021 Rate and Benefit UpdateSixta Simbulan100% (1)
- Summary of 2022 Benefit Changes: MedicalDocument5 pagesSummary of 2022 Benefit Changes: MedicalChinnu SalimathNo ratings yet
- WWW - Healthcare.Gov/Sbc-Glossary/: Important Questions Answers Why This MattersDocument10 pagesWWW - Healthcare.Gov/Sbc-Glossary/: Important Questions Answers Why This MattersSai SandeepNo ratings yet
- Important Information About Your Insurance: GPO Box 1901 Melbourne VIC 3001 Australia T 1300 300 273 F 1300 366 273Document8 pagesImportant Information About Your Insurance: GPO Box 1901 Melbourne VIC 3001 Australia T 1300 300 273 F 1300 366 273Antoine Nabil ZakiNo ratings yet
- Sumario Every Day BrozeDocument9 pagesSumario Every Day BrozeMiriangely GonzalezNo ratings yet
- 1500SBC2021Document8 pages1500SBC2021Carlos Andres Correa Gomez (Carlos Gomez)No ratings yet
- AA1B Index Statement of AccountsDocument5 pagesAA1B Index Statement of AccountsbscurNo ratings yet
- SBC - Cdo - 2019 2Document6 pagesSBC - Cdo - 2019 2Dinko KajtezovićNo ratings yet
- 2013 Benefits SummaryDocument0 pages2013 Benefits SummarybalajisaireddyNo ratings yet
- Eligibility Results NoticeDocument11 pagesEligibility Results NoticeJoshua HillNo ratings yet
- OE Powerpoint PresentationDocument35 pagesOE Powerpoint PresentationAnonymous ibpKT07GNo ratings yet
- UnitedHealthcare Choice Plus 1000Document10 pagesUnitedHealthcare Choice Plus 1000govindhegdeNo ratings yet
- United Healthcare UHC Premier 1500 CEFP GoldDocument14 pagesUnited Healthcare UHC Premier 1500 CEFP GoldSteveNo ratings yet
- Summary of Benefits: Quartz Medicare Advantage (HMO), in Partnership With UW HealthDocument20 pagesSummary of Benefits: Quartz Medicare Advantage (HMO), in Partnership With UW HealthChris CoulmanNo ratings yet
- G622CHC Blue Choice Gold PPO 022: This Is Only A SummaryDocument8 pagesG622CHC Blue Choice Gold PPO 022: This Is Only A SummaryAnonymous nx3VC6zHn2No ratings yet
- Important Questions Answers Why This MattersDocument10 pagesImportant Questions Answers Why This MattersGeraldine HerreraNo ratings yet
- SpdsDocument39 pagesSpdsVinod KumarNo ratings yet
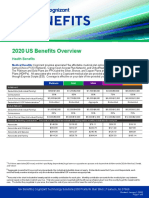
- 2020 US Benefits OverviewDocument5 pages2020 US Benefits OverviewrdmNo ratings yet
- S608CHC Blue Choice Silver PPO 024: This Is Only A SummaryDocument8 pagesS608CHC Blue Choice Silver PPO 024: This Is Only A SummaryAnonymous nx3VC6zHn2No ratings yet
- BlueSelect 1456B Coverage SummaryDocument10 pagesBlueSelect 1456B Coverage SummarybrineshrimpNo ratings yet
- CJL 5000 Hsa Plan 2024 SBC Final 10182023Document8 pagesCJL 5000 Hsa Plan 2024 SBC Final 10182023dominicvjohnson03No ratings yet
- Healthyblue Advantage Platinum 500: Important Questions Answers Why This MattersDocument12 pagesHealthyblue Advantage Platinum 500: Important Questions Answers Why This MattersBertrandNo ratings yet
- How To Release An IRS Wage Garnishment or Bank LevyDocument9 pagesHow To Release An IRS Wage Garnishment or Bank LevyKeith Duke JonesNo ratings yet
- Habasit 2017 Benefits GuideDocument2 pagesHabasit 2017 Benefits GuideBlackBunny103No ratings yet
- Eligibility Results NoticeDocument12 pagesEligibility Results NoticeDesign to BlessNo ratings yet
- Understanding Money: How To Make It Work For YouDocument46 pagesUnderstanding Money: How To Make It Work For YouMonique BagaporoNo ratings yet
- Understanding Your EOBDocument1 pageUnderstanding Your EOBkrishna EnagaluruNo ratings yet
- En 05 11015Document36 pagesEn 05 11015Kenneth GarrisonNo ratings yet
- Eligibility Results NoticeDocument12 pagesEligibility Results NoticeLagannNo ratings yet
- AMBETTER SECURE C5 STDDocument9 pagesAMBETTER SECURE C5 STDanarepsdcNo ratings yet
- 2020 Ankura Benefits GuideDocument20 pages2020 Ankura Benefits GuidegpperkNo ratings yet
- 2017 UHC EPO Benefit Summary Muping Health InsuranceDocument16 pages2017 UHC EPO Benefit Summary Muping Health InsurancescartoonNo ratings yet
- 02 28 2019Document4 pages02 28 2019Deep khatkarNo ratings yet
- Anthem Silver Preferred Blue PPO 3000 20 7250 W HSA NH PPO Small 6UPP 01 01 2023 English SBC CYDocument12 pagesAnthem Silver Preferred Blue PPO 3000 20 7250 W HSA NH PPO Small 6UPP 01 01 2023 English SBC CYsantiagomNo ratings yet
- 91e42b93-5ed0-4112-93fd-4403b365bb74Document32 pages91e42b93-5ed0-4112-93fd-4403b365bb74hekmatNo ratings yet
- Age Pension B295053424Document2 pagesAge Pension B295053424JOHAN SEBASTIAN GOMEZ ALVAREZNo ratings yet
- TNS Brochure 2021Document9 pagesTNS Brochure 2021chugn245No ratings yet
- SBC Summary: What This Health Plan CoversDocument10 pagesSBC Summary: What This Health Plan CoversGeorge OnacillaNo ratings yet
- Sione and Andrea (Rework)Document10 pagesSione and Andrea (Rework)Ammer Yaser MehetanNo ratings yet
- B601CHC Blue Choice Bronze PPO 031: This Is Only A SummaryDocument8 pagesB601CHC Blue Choice Bronze PPO 031: This Is Only A SummaryAnonymous nx3VC6zHn2No ratings yet
- Tax Year 2013 DeskReferenceGuideDocument8 pagesTax Year 2013 DeskReferenceGuideMia JacksonNo ratings yet
- Lesson 1 DebtDocument21 pagesLesson 1 DebtAlf ChingNo ratings yet
- Allowed Amount Balance Billing Coinsurance Copayment Deductible ProviderDocument7 pagesAllowed Amount Balance Billing Coinsurance Copayment Deductible Providergary kornegayNo ratings yet
- UPMC Small Business Advantage Gold PPO $1,500 $35/$50 BenefitsDocument7 pagesUPMC Small Business Advantage Gold PPO $1,500 $35/$50 BenefitsTim ZNo ratings yet
- Bronze 60 PPO MJ002189 01-24 SBCDocument9 pagesBronze 60 PPO MJ002189 01-24 SBCwannieNo ratings yet
- EligibilityResultsNotice 4Document12 pagesEligibilityResultsNotice 4Aaron MarcyNo ratings yet
- Plan Plan Plan Premium: Important Questions Answers Why This MattersDocument8 pagesPlan Plan Plan Premium: Important Questions Answers Why This Mattersrocerev539No ratings yet
- Aetna SBC 2024 Standard Plan Express ScriptsDocument15 pagesAetna SBC 2024 Standard Plan Express Scriptskatika3011No ratings yet
- WP Tep Leaving Your Employer en PDFDocument8 pagesWP Tep Leaving Your Employer en PDFJayNo ratings yet
- Medical Deductibles: High Deductible Health Plan (HDHP)Document3 pagesMedical Deductibles: High Deductible Health Plan (HDHP)Sergio ArtinanoNo ratings yet
- Benefits SummaryDocument2 pagesBenefits SummaryGustavo StorNo ratings yet
- Important Questions Answers Why This Matters:: Oscar: Silver Simple Plan Coverage Period: 01/01/2022 - 12/31/2022Document10 pagesImportant Questions Answers Why This Matters:: Oscar: Silver Simple Plan Coverage Period: 01/01/2022 - 12/31/2022Rolando Vicente godinezNo ratings yet
- EligibilityResultsNotice 2Document12 pagesEligibilityResultsNotice 2Shannon GambleNo ratings yet
- Budget Basics For Modular Home Buyers - How Much Home Can I Afford?Document3 pagesBudget Basics For Modular Home Buyers - How Much Home Can I Afford?SEAN NNo ratings yet
- Maryland Vital Statistics: Infant Mortality in MarylandDocument4 pagesMaryland Vital Statistics: Infant Mortality in MarylandOswaldo ParraNo ratings yet
- Food Allergies Prevention SystemDocument11 pagesFood Allergies Prevention SystemOswaldo ParraNo ratings yet
- Traditional Venezuelan Christmas Food: By: Carmen Victoria GarciaDocument27 pagesTraditional Venezuelan Christmas Food: By: Carmen Victoria GarciaOswaldo ParraNo ratings yet
- Dental Orthodontics Search On 3-7-2014Document4 pagesDental Orthodontics Search On 3-7-2014Oswaldo ParraNo ratings yet
- Catalog Part 2Document68 pagesCatalog Part 2Oswaldo ParraNo ratings yet
- Math 08 RTQDocument88 pagesMath 08 RTQOswaldo ParraNo ratings yet
- Cuneiform Luvian Lexicon-Vol02 PDFDocument307 pagesCuneiform Luvian Lexicon-Vol02 PDFJuju PoilNo ratings yet
- Review Quiz in English1Document8 pagesReview Quiz in English1Ricardo RicafortNo ratings yet
- Kendriya Vidyalaya Sangathan Raipur Region Sample Paper TERM - 2 EXAM (2021-22) Class: VII Subject:ENGLISH SET-1 Time: 90 Min Max. Marks: 40Document3 pagesKendriya Vidyalaya Sangathan Raipur Region Sample Paper TERM - 2 EXAM (2021-22) Class: VII Subject:ENGLISH SET-1 Time: 90 Min Max. Marks: 40pvreachNo ratings yet
- An Introductory English Grammar by N. C. StagebergDocument377 pagesAn Introductory English Grammar by N. C. StagebergMohmmed Qasm85% (41)
- Vaughan Review Oct 2009Document36 pagesVaughan Review Oct 2009Luis fabiano Rivera canales100% (1)
- II Partial Homework 6 IndividualDocument3 pagesII Partial Homework 6 Individualjavier salezNo ratings yet
- Academic WritingDocument9 pagesAcademic WritingJoel PallanNo ratings yet
- Actividades Ingles IIIDocument14 pagesActividades Ingles IIINadia Castaño NoreñaNo ratings yet
- Lagos JSS English Schemes of WorkDocument23 pagesLagos JSS English Schemes of Workfaith100% (2)
- HEBREW SAL 2014 (Updated June 2014)Document21 pagesHEBREW SAL 2014 (Updated June 2014)Chevi litsNo ratings yet
- Abnormal Child Psychology - 6thDocument32 pagesAbnormal Child Psychology - 6thAzzura BalqisNo ratings yet
- My Name Is Wuyi. I Am A TeacherDocument2 pagesMy Name Is Wuyi. I Am A TeacherDian UtamiNo ratings yet
- Nama: Rahmi Binarti NIM: BIG201017 Uas English Semantics: A. B. C. D. eDocument3 pagesNama: Rahmi Binarti NIM: BIG201017 Uas English Semantics: A. B. C. D. eAzizah Rusmin NoviaNo ratings yet
- Grade 6 week 26.Document4 pagesGrade 6 week 26.Heba SamirNo ratings yet
- Contoh Recount TextDocument2 pagesContoh Recount Text1Bkomala widia sovaNo ratings yet
- How Does Learning About Affixes (Prefixes and Suffixes) Help EnglDocument177 pagesHow Does Learning About Affixes (Prefixes and Suffixes) Help EnglNoviNo ratings yet
- Gerundijum-Glagolska ImenicaDocument5 pagesGerundijum-Glagolska ImenicajelenabogdanNo ratings yet
- Interviewing As A Data Collection Method: A Critical Review: January 2014Document8 pagesInterviewing As A Data Collection Method: A Critical Review: January 2014Duc-2D-19 Pham Thi Khanh DuyenNo ratings yet
- Auyero, Javier. Patients of The StateDocument26 pagesAuyero, Javier. Patients of The StateDaniela VelasquezNo ratings yet
- Mid-term Test of Second Language AcquisitionDocument8 pagesMid-term Test of Second Language AcquisitionElut HidaNo ratings yet
- Lesson1 RevDocument55 pagesLesson1 RevYusuf Abdul HaqNo ratings yet
- Speaking (A2 Pre-Intermediate) : English For LifeDocument2 pagesSpeaking (A2 Pre-Intermediate) : English For LifeSuresh DassNo ratings yet
- Unit 7: City Living: GrammarDocument16 pagesUnit 7: City Living: GrammarNicholas RomeroNo ratings yet
- Dap An Van Hoa - Tieng Viet - KH2Document8 pagesDap An Van Hoa - Tieng Viet - KH2Hoanh Anh NguyenNo ratings yet
- Oral Communication in Context LM For SHSPDFDocument191 pagesOral Communication in Context LM For SHSPDFornopia45_548639769No ratings yet
- 2011 OL English Past Paper and AnswersDocument32 pages2011 OL English Past Paper and AnswersMeghawarna RajanayakaNo ratings yet
- Perfect TOEFL Speaking - Final - PaperDocument86 pagesPerfect TOEFL Speaking - Final - PaperNazarNo ratings yet
- ctl2011 4235 Wky201 PDFDocument22 pagesctl2011 4235 Wky201 PDFmaka durglishviliNo ratings yet
- AssimilationDocument2 pagesAssimilationErine ContranoNo ratings yet
- Stage 2 Compound SentenceDocument10 pagesStage 2 Compound SentenceGabriel CisnerosNo ratings yet