You might also like
- Internal Hexagon Morse Taper Connection PDFDocument7 pagesInternal Hexagon Morse Taper Connection PDFDhanu DhanushreeNo ratings yet
- Avrampou COIR 2013Document8 pagesAvrampou COIR 2013jose luis delgadilloNo ratings yet
- Evaluating The Primary Stability of Implants by Two Different Insertion Methodsin Compromised Bone - A Pilot StudyDocument6 pagesEvaluating The Primary Stability of Implants by Two Different Insertion Methodsin Compromised Bone - A Pilot StudydentureNo ratings yet
- Sciasci Et Al-2018-Clinical Implant Dentistry and Related ResearchDocument6 pagesSciasci Et Al-2018-Clinical Implant Dentistry and Related ResearchBagis Emre GulNo ratings yet
- Influ Com Cera PreDocument11 pagesInflu Com Cera Pre裕介入江No ratings yet
- 1 s2.0 S0021929014005429 MainDocument8 pages1 s2.0 S0021929014005429 MainDANTE DELEGUERYNo ratings yet
- Jaw Density Implant PlanningDocument7 pagesJaw Density Implant Planningmarcela fajardoNo ratings yet
- Comparative Evaluation of Initial Crestal Bone Loss Around Dental Implants Using Flapless or Flap Method: An in Vivo StudyDocument9 pagesComparative Evaluation of Initial Crestal Bone Loss Around Dental Implants Using Flapless or Flap Method: An in Vivo StudyIJAR JOURNALNo ratings yet
- Resonance Frequency Analysis (RFA) and InsertionaDocument11 pagesResonance Frequency Analysis (RFA) and InsertionaPablo BenitezNo ratings yet
- 12TH JC PDFDocument6 pages12TH JC PDFSMART SMARNo ratings yet
- EBSCO FullText 2023 10 06Document25 pagesEBSCO FullText 2023 10 06Marcio FalcaoNo ratings yet
- Correlation Between Miniscrew Stability and Bone Mineral Density in Orthodontic PatientsDocument8 pagesCorrelation Between Miniscrew Stability and Bone Mineral Density in Orthodontic PatientsLaura Juarez navejasNo ratings yet
- Effect of Platform Switching On Peri-Implant Bone: A 3D Finite Element AnalysisDocument6 pagesEffect of Platform Switching On Peri-Implant Bone: A 3D Finite Element AnalysismaiNo ratings yet
- Crestal Bone Level Around Tissue-Level Implants Restored With Platform Matching and Bone-Level ImplantsDocument9 pagesCrestal Bone Level Around Tissue-Level Implants Restored With Platform Matching and Bone-Level Implantscd.brendasotofloresNo ratings yet
- CM Niveis Osseos DiferentesDocument8 pagesCM Niveis Osseos DiferentesMarco TeixeiraNo ratings yet
- Novellino 2013Document6 pagesNovellino 2013Glais FerrariNo ratings yet
- Correlation Between Bone Density and Instantaneous Torque at Implant Site Preparation A Validation On Polyurethane Foam Blocks of A Device Assessing Density of JawbonesDocument8 pagesCorrelation Between Bone Density and Instantaneous Torque at Implant Site Preparation A Validation On Polyurethane Foam Blocks of A Device Assessing Density of Jawbonesdrmezzo68No ratings yet
- Particularităţi de Evaluare Şi Planificare A TratamentuluiDocument5 pagesParticularităţi de Evaluare Şi Planificare A TratamentuluiCiutac ŞtefanNo ratings yet
- Journal - 620 Stress-Diversion Surface SDS Dental Implant OriginalDocument28 pagesJournal - 620 Stress-Diversion Surface SDS Dental Implant OriginalHamdani NurdinNo ratings yet
- Li 2011Document11 pagesLi 2011Hurāirāh ĐāřNo ratings yet
- Which Is The Best Choice After Tooth Extraction, Immediate ImplantDocument10 pagesWhich Is The Best Choice After Tooth Extraction, Immediate Implantjuanita enriquezNo ratings yet
- Final Article JopDocument6 pagesFinal Article JopNaina TalwarNo ratings yet
- 1 s2.0 S0889540614008634 MainDocument7 pages1 s2.0 S0889540614008634 MainPanaite TinelaNo ratings yet
- Litreture Review 5Document6 pagesLitreture Review 5Daniel AtiehNo ratings yet
- JPD 2018 Vol 119 P 611 619Document9 pagesJPD 2018 Vol 119 P 611 619hheussinger3893No ratings yet
- Guidelines For Selecting The Implant Diameter During Immediate Implant Placement of A Fresh Extraction Socket: A Case SeriesDocument10 pagesGuidelines For Selecting The Implant Diameter During Immediate Implant Placement of A Fresh Extraction Socket: A Case SeriesDr. Pragyan SwainNo ratings yet
- Implant Design PDFDocument9 pagesImplant Design PDFnatan XxNo ratings yet
- Manualdefotografia PDFDocument9 pagesManualdefotografia PDFMarco TeixeiraNo ratings yet
- IJAERS-01 August 2021Document7 pagesIJAERS-01 August 2021IJAERS JOURNALNo ratings yet
- Titanium Mesh Ridges RecontructionDocument11 pagesTitanium Mesh Ridges RecontructionМилутинМићићNo ratings yet
- Accuracy of 3D ReconstructionsDocument5 pagesAccuracy of 3D Reconstructionsgileno pagamentosNo ratings yet
- Survival/Success of Dental Implants With Acid-Etched Surfaces: A Retrospective Evaluation After 8 To 10 YearsDocument7 pagesSurvival/Success of Dental Implants With Acid-Etched Surfaces: A Retrospective Evaluation After 8 To 10 YearsBagis Emre GulNo ratings yet
- 2-Referencias y Tecnicas Usadas en Clasificacion Hueso Alveolar - SeriwatanachaiDocument5 pages2-Referencias y Tecnicas Usadas en Clasificacion Hueso Alveolar - SeriwatanachaimnhjrtbnzbNo ratings yet
- Stability of Tapered and Parallel-Walled Dental Implants: A Systematic Review and Meta-AnalysisDocument12 pagesStability of Tapered and Parallel-Walled Dental Implants: A Systematic Review and Meta-AnalysisBagis Emre GulNo ratings yet
- Orto en PulpaDocument4 pagesOrto en PulpaPablo GodinezNo ratings yet
- Precision of Dental Implant Digitization Using Intraoral ScannersDocument7 pagesPrecision of Dental Implant Digitization Using Intraoral ScannersSkAliHassanNo ratings yet
- Influence of Diameter and Length of Implant On Early Dental Implant FailureDocument6 pagesInfluence of Diameter and Length of Implant On Early Dental Implant FailureCatalina AndreeaNo ratings yet
- Influencia Del Diente Intraradicular y Lacorona Ferula Con La Resistencia Ala FracturaDocument6 pagesInfluencia Del Diente Intraradicular y Lacorona Ferula Con La Resistencia Ala FracturacatalinaNo ratings yet
- A Multilevel Analysis of Platform-Switching Flapless Implants Placed at Tissue Level: 4-Year Prospective Cohort StudyDocument13 pagesA Multilevel Analysis of Platform-Switching Flapless Implants Placed at Tissue Level: 4-Year Prospective Cohort Studyhkwgt7vskwNo ratings yet
- 00-2 EJD 2016 (10-1) 0148-0154 (Macedo-Et Al)Document7 pages00-2 EJD 2016 (10-1) 0148-0154 (Macedo-Et Al)Jose Manuel de la FuenteNo ratings yet
- Insertion Torque and Periotest Values Are Important Factors Predicting Outcome After Orthodontic Miniscrew PlacementDocument6 pagesInsertion Torque and Periotest Values Are Important Factors Predicting Outcome After Orthodontic Miniscrew PlacementGiovanni Eduardo Medina MartinezNo ratings yet
- 6 de Oct - Effect of Incisal Loading During Orthodontic Treatment in AdultsDocument10 pages6 de Oct - Effect of Incisal Loading During Orthodontic Treatment in AdultsLaura Andrea Agudelo WilchesNo ratings yet
- Splinted Vs Nonsplinted ImplantsDocument11 pagesSplinted Vs Nonsplinted ImplantsMathias SchottNo ratings yet
- Clinical Application of Stereolithographic SurgicalDocument2 pagesClinical Application of Stereolithographic SurgicalJeanIvanDosSantosNo ratings yet
- Prediction of Implant Loss and Marginal Bone Loss by Analysis of Dental Panoramic RadiographsDocument6 pagesPrediction of Implant Loss and Marginal Bone Loss by Analysis of Dental Panoramic RadiographsMuhammad RidwanNo ratings yet
- Influence of Thin Mucosal Tissues On Crestal Bone Stability Around Implants With Platform Switching: A 1-Year Pilot StudyDocument6 pagesInfluence of Thin Mucosal Tissues On Crestal Bone Stability Around Implants With Platform Switching: A 1-Year Pilot StudyPedro Maria Crizul BarretoNo ratings yet
- Optimo ImplanteDocument10 pagesOptimo ImplanteGonzalo Junior Crespo PadronNo ratings yet
- Accuracy of Different SurgicalDocument8 pagesAccuracy of Different SurgicalVõHoàngThủyTiênNo ratings yet
- RetrieveDocument10 pagesRetrieveDANTE DELEGUERYNo ratings yet
- Correlation Between The Mechanical Properties and Structural Characteristics of Different Fiber Posts SystemsDocument6 pagesCorrelation Between The Mechanical Properties and Structural Characteristics of Different Fiber Posts SystemsLuis AraújoNo ratings yet
- Correlation Between Placement Torque and Survival of Single-Tooth ImplantsDocument8 pagesCorrelation Between Placement Torque and Survival of Single-Tooth ImplantssheetalNo ratings yet
- 5 PDFDocument6 pages5 PDFalejandra_baltaza_17No ratings yet
- Implant-Bone IntegrationDocument14 pagesImplant-Bone IntegrationADanAlfaNo ratings yet
- Implant-Abutment Connections and Their Effect on Implant Survival Rates and Changes in Marginal Bone Levels (ΔMBL) : A Systematic Review and Meta-Analysis of 45,347 Oral ImplantsDocument25 pagesImplant-Abutment Connections and Their Effect on Implant Survival Rates and Changes in Marginal Bone Levels (ΔMBL) : A Systematic Review and Meta-Analysis of 45,347 Oral Implantshkwgt7vskwNo ratings yet
- Two Distalization Methods Compared in A Novel Patient-Speci Fic Finite Element AnalysisDocument11 pagesTwo Distalization Methods Compared in A Novel Patient-Speci Fic Finite Element AnalysisMaisely Fabiluz Galindo GomNo ratings yet
- Sousa2016 PDFDocument11 pagesSousa2016 PDFEsme ValenciaNo ratings yet
- ContentServer - Asp 11Document12 pagesContentServer - Asp 11Sergio Lamas RamirezNo ratings yet
- Implantoplasty Enhancing Peri-Implant Bone Stability Over A 3-Year Follow-Up: A Case SeriesDocument8 pagesImplantoplasty Enhancing Peri-Implant Bone Stability Over A 3-Year Follow-Up: A Case SeriesBagis Emre GulNo ratings yet
- A Finite Element Study Designs of ImplantsDocument13 pagesA Finite Element Study Designs of ImplantsCarla AnflorNo ratings yet
- Short ImplantsFrom EverandShort ImplantsBoyd J. TomasettiNo ratings yet
- Difference Between PPM and PPMVDocument2 pagesDifference Between PPM and PPMVKhanh TrangNo ratings yet
- Get TRDocDocument185 pagesGet TRDockfrisch1229No ratings yet
- ELEC 4170 1 Diode Rectifiers Fall 2022Document14 pagesELEC 4170 1 Diode Rectifiers Fall 2022Tafheem AlphaNo ratings yet
- Valve Catalogue General Imsubs Pvt. Ltd.Document20 pagesValve Catalogue General Imsubs Pvt. Ltd.Spark MeditechNo ratings yet
- BibliographyDocument5 pagesBibliographyMonal ParekhNo ratings yet
- Using Oracle Database Vault With Oracle Database 12c - D86597GC10 - 1080544 - USDocument3 pagesUsing Oracle Database Vault With Oracle Database 12c - D86597GC10 - 1080544 - USJinendraabhi0% (1)
- TL140 Workshop Manual (CT9E004)Document613 pagesTL140 Workshop Manual (CT9E004)kris75% (8)
- 01 01 14 2Document12 pages01 01 14 2brains26No ratings yet
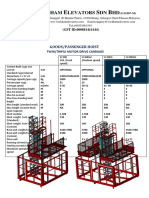
- SC200 RevDocument2 pagesSC200 RevAshraf MuhtarNo ratings yet
- Design of Triangular Reinforced Concrete Beam in Usd: March 2011Document10 pagesDesign of Triangular Reinforced Concrete Beam in Usd: March 2011Husen GhoriNo ratings yet
- Loctite Instant Adhesives: Instant Solutions in Every DropDocument9 pagesLoctite Instant Adhesives: Instant Solutions in Every DroptejassidhpuraNo ratings yet
- Global System For Mobile Communications (GSM) : 1 Summer Internship ReportDocument51 pagesGlobal System For Mobile Communications (GSM) : 1 Summer Internship ReportAvay SinghNo ratings yet
- N Queen ProblemDocument2 pagesN Queen ProblemManikandanNo ratings yet
- Getting Started With Openfoam: Eric PatersonDocument41 pagesGetting Started With Openfoam: Eric PatersonReza Nazari0% (1)
- MEISER Grating PDFDocument136 pagesMEISER Grating PDFEngr Qaisar NazeerNo ratings yet
- Panaray 802 Series III Loudspeaker: General DescriptionDocument4 pagesPanaray 802 Series III Loudspeaker: General Descriptionadibecha100% (1)
- A Preliminary Literature Review of Digital Transformation Case StudiesDocument6 pagesA Preliminary Literature Review of Digital Transformation Case StudiesLucija IvancicNo ratings yet
- Progressreport WritingDocument16 pagesProgressreport WritingSheraz AliNo ratings yet
- Flange DimensionsDocument7 pagesFlange DimensionsDave DonohueNo ratings yet
- Uni - 02-0056-Q24063, YPFB Andina SA, 901-042-059-001 - 15h30m - 08122022Document7 pagesUni - 02-0056-Q24063, YPFB Andina SA, 901-042-059-001 - 15h30m - 08122022josecordova2014No ratings yet
- TQMDocument55 pagesTQMTanmoy GuhaNo ratings yet
- Lab Open Ended Dry Sieve AnalysisDocument9 pagesLab Open Ended Dry Sieve Analysiskhairul hisyamNo ratings yet
- Product Handling: Complete Solutions From A Single SourceDocument24 pagesProduct Handling: Complete Solutions From A Single Sourcemarciojunk100% (1)
- 2 - WCDMA Power ControlDocument50 pages2 - WCDMA Power ControlSabrine Chahbi100% (1)
- Mujahadeen AR-15Document13 pagesMujahadeen AR-15Chris Leahy100% (2)
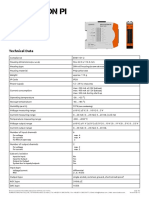
- Datasheet RevPi AIODocument2 pagesDatasheet RevPi AIOsebadansNo ratings yet
- Display Nec NL6448BC33 74 PreDocument30 pagesDisplay Nec NL6448BC33 74 PrehenryvyperNo ratings yet
- Peugeot 206Document1 pagePeugeot 206Sergio Hernandez0% (1)
- Metallographic Sample Preparation Techniques: BackgroundDocument8 pagesMetallographic Sample Preparation Techniques: BackgroundQA LAB ISMNo ratings yet
- N-1-1 Contingency Analysis Using Powerworld SimulatorDocument15 pagesN-1-1 Contingency Analysis Using Powerworld Simulatorchandana901No ratings yet