You might also like
- Thyroglossal Duct CystDocument38 pagesThyroglossal Duct CystMilrose GamboaNo ratings yet
- Gold Standards in Medical FieldDocument8 pagesGold Standards in Medical FieldJyothisankar Radhakrishnan100% (2)
- #Immunoprophylaxis and ImmunizationsDocument3 pages#Immunoprophylaxis and Immunizationsameerabest100% (1)
- DR Dicky L Tahapary SPPD PhD-Hyperglycemic Crises IMELS PDFDocument38 pagesDR Dicky L Tahapary SPPD PhD-Hyperglycemic Crises IMELS PDFDemograf27No ratings yet
- 4 Oet Reading Summary 2.0Document19 pages4 Oet Reading Summary 2.0Vijayalakshmi Narayanaswami0% (3)
- Colostomy CareDocument8 pagesColostomy CareAhmed Hamed100% (2)
- Medicine Long CaseDocument26 pagesMedicine Long Casewhee182No ratings yet
- Cheat Sheet - EAU NMIBC V 2.0Document1 pageCheat Sheet - EAU NMIBC V 2.0Eduardo5671No ratings yet
- NMIBC Guide: Diagnosis and Management of Non-Muscle Invasive Bladder CancerDocument20 pagesNMIBC Guide: Diagnosis and Management of Non-Muscle Invasive Bladder CancerMade Moniaga PrawiraNo ratings yet
- Radiologi Edit-1Document50 pagesRadiologi Edit-1Resi OfzanNo ratings yet
- RadiologiDocument54 pagesRadiologiresi silviaNo ratings yet
- 1 s2.0 S105342962200056X MainDocument9 pages1 s2.0 S105342962200056X MainFatimah AssagafNo ratings yet
- UTUCDocument39 pagesUTUCShalini shreeNo ratings yet
- Med2 1.06FDocument5 pagesMed2 1.06FMaikka IlaganNo ratings yet
- Cystic Neoplasms of The PancreasDocument9 pagesCystic Neoplasms of The PancreasSanjaya SenevirathneNo ratings yet
- Positron Emission Tomography.: Biopsy TechniquesDocument6 pagesPositron Emission Tomography.: Biopsy TechniquesAnonymous UTUWFODCEYNo ratings yet
- Diagnosis of Soft Tissue MassDocument11 pagesDiagnosis of Soft Tissue MassMalcolm BaringNo ratings yet
- Oral Cancer and ManagementDocument148 pagesOral Cancer and ManagementFadilaNo ratings yet
- Paper ERIKA Core BXDocument8 pagesPaper ERIKA Core BXHarlley SenaNo ratings yet
- CancerDocument29 pagesCancerakbar akbarNo ratings yet
- EAU Guideline 2021Document20 pagesEAU Guideline 2021G WNo ratings yet
- Manejo Ca Cervical BMJDocument5 pagesManejo Ca Cervical BMJNathalia M.No ratings yet
- Ariana Ya GamDocument5 pagesAriana Ya GamdrelvNo ratings yet
- CancerDocument8 pagesCancerChrisMerellNo ratings yet
- Development of Electrochemical Biosensor For Breast Cancer Detection Using Gold Nanoparticle Doped CA 15-3 Antibody and Antigen InteractionDocument7 pagesDevelopment of Electrochemical Biosensor For Breast Cancer Detection Using Gold Nanoparticle Doped CA 15-3 Antibody and Antigen InteractionwardaninurindahNo ratings yet
- Bladder Tumor Markers Beyond Cytology in PDFDocument29 pagesBladder Tumor Markers Beyond Cytology in PDFMariana CreciunNo ratings yet
- 71) Cancer of The EsophagusDocument29 pages71) Cancer of The EsophagusANNA CarausNo ratings yet
- Report Adil'12Document6 pagesReport Adil'12adilhusain1710465482No ratings yet
- Comprehensive Surgical Treatment Strategy For Spinal MetastasesDocument11 pagesComprehensive Surgical Treatment Strategy For Spinal MetastasessukiyantoNo ratings yet
- Mucinous Cystic Neoplasm of Liver - Peeling Sign Mitigates A Diagnostic ConundrumDocument8 pagesMucinous Cystic Neoplasm of Liver - Peeling Sign Mitigates A Diagnostic ConundrumIJAR JOURNALNo ratings yet
- Cancer Screening GuidelinesDocument3 pagesCancer Screening GuidelinesAra DiocosNo ratings yet
- Tumor Markers: Understanding Their Clinical ApplicationsDocument18 pagesTumor Markers: Understanding Their Clinical Applicationsintanridr_742395171No ratings yet
- Principles of Surgical OncologyDocument34 pagesPrinciples of Surgical Oncologykaukab azim100% (1)
- CtDNA-Based Liquid Biopsy of Cerebrospinal Fluid in Brain CancerDocument15 pagesCtDNA-Based Liquid Biopsy of Cerebrospinal Fluid in Brain CancerAnyaNo ratings yet
- Cervical Cancer Screening - AHS GuidelineDocument9 pagesCervical Cancer Screening - AHS GuidelineBasil al-hashaikehNo ratings yet
- Tumor Marker GUPERDocument15 pagesTumor Marker GUPERyessiNo ratings yet
- Carcinoma of UnknownDocument31 pagesCarcinoma of Unknownsamer falconNo ratings yet
- Oncology 1Document50 pagesOncology 1Syahmi YahyaNo ratings yet
- Ovarian Masses: Surgery or Surveillance?Document9 pagesOvarian Masses: Surgery or Surveillance?MutianbllNo ratings yet
- Cancers of The Female Genital TractDocument31 pagesCancers of The Female Genital TractTresor MbuyiNo ratings yet
- Inflammatory Myofibroblastic TumourDocument4 pagesInflammatory Myofibroblastic TumourThiruNo ratings yet
- Cancer CareDocument84 pagesCancer Careakoeljames8543No ratings yet
- Ovarian Cancer Notes - G7 3BSN1Document52 pagesOvarian Cancer Notes - G7 3BSN1Shyne HazyNo ratings yet
- Retro Peritoneal TumorDocument37 pagesRetro Peritoneal TumorHafizur RashidNo ratings yet
- Unusual Discovery Incidental Diagnosis of Adrenal Myelol 2024 InternationalDocument4 pagesUnusual Discovery Incidental Diagnosis of Adrenal Myelol 2024 InternationalRonald QuezadaNo ratings yet
- Borderline Tumors of The OvaryDocument6 pagesBorderline Tumors of The OvaryIJAR JOURNALNo ratings yet
- Epidemiology: Oncology NursingDocument23 pagesEpidemiology: Oncology NursingMiden AlbanoNo ratings yet
- Mizuno Et Al 2021Document20 pagesMizuno Et Al 2021Abner PortilhoNo ratings yet
- Parotidectomia - UpToDate 2022Document2 pagesParotidectomia - UpToDate 2022juanrangoneNo ratings yet
- SEOC CASE PRESENTATION AND MANAGEMENTDocument22 pagesSEOC CASE PRESENTATION AND MANAGEMENTAddis Hiwot General HospitalNo ratings yet
- Care For Women: With Ovarian, Cerviacl, Vulvar and Endometrial CancerDocument26 pagesCare For Women: With Ovarian, Cerviacl, Vulvar and Endometrial CancerAhmad JradeenNo ratings yet
- Biopsy Techniques for Musculoskeletal TumorsDocument9 pagesBiopsy Techniques for Musculoskeletal TumorsAidil NurshalNo ratings yet
- Clinical Practice GuidelinesDocument6 pagesClinical Practice GuidelinesCarlos Rodolfo SinibaldiNo ratings yet
- computed tomographyDocument12 pagescomputed tomographyYessi PerlitasariNo ratings yet
- Oncology OverviewDocument42 pagesOncology OverviewХина КападиаNo ratings yet
- A Review of The Diagnosis and Management of Premalignant Pancreatic Cystic LesionsDocument23 pagesA Review of The Diagnosis and Management of Premalignant Pancreatic Cystic Lesionssanti lestariNo ratings yet
- Urinary Tract CancerDocument53 pagesUrinary Tract CancerandikaisnaeniNo ratings yet
- Bladder Cancer Diagnosis and Management of Bladder Cancer 2017Document11 pagesBladder Cancer Diagnosis and Management of Bladder Cancer 2017drelvNo ratings yet
- Oncology Nursing Part 1 2Document51 pagesOncology Nursing Part 1 2fleur harrisonNo ratings yet
- urine exosomeDocument8 pagesurine exosomeBoutaina AddoumNo ratings yet
- Cc2 - MidtermDocument3 pagesCc2 - MidtermMika SusadaNo ratings yet
- Beal 2020Document17 pagesBeal 2020Nikos SerifisNo ratings yet
- European Association of Urology Guidelines On Muscle-Invasive and Metastatic Bladder Cancer: of The 2020 GuidelinesDocument23 pagesEuropean Association of Urology Guidelines On Muscle-Invasive and Metastatic Bladder Cancer: of The 2020 GuidelinesBalqist Asyawa Andra PutriNo ratings yet
- Oncology ArticleDocument3 pagesOncology ArticleSaundarya RaiNo ratings yet
- Management of Salivary Gland Tumours: United Kingdom National Multidisciplinary GuidelinesDocument8 pagesManagement of Salivary Gland Tumours: United Kingdom National Multidisciplinary GuidelinesCeriaindriasariNo ratings yet
- Articulo CientificoDocument15 pagesArticulo CientificoDouglas RecinosNo ratings yet
- Salivary Gland Cancer: From Diagnosis to Tailored TreatmentFrom EverandSalivary Gland Cancer: From Diagnosis to Tailored TreatmentLisa LicitraNo ratings yet
- GBS 2Document179 pagesGBS 2m3510No ratings yet
- Coek - Info The Carcinosin Drug PictureDocument12 pagesCoek - Info The Carcinosin Drug Picturesayeed.bcs30100% (1)
- Pathology of AppendixDocument26 pagesPathology of Appendixnovitafitri123No ratings yet
- Algoritmo Diagnostico en SdraDocument8 pagesAlgoritmo Diagnostico en SdraPierina VeramatosNo ratings yet
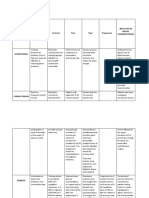
- Medical Conditions Frequency Intensity Time Type Progression Red Flags or Special ConsideratrionsDocument4 pagesMedical Conditions Frequency Intensity Time Type Progression Red Flags or Special ConsideratrionsClaire Madriaga GidoNo ratings yet
- Flucloxacillin AFTcapssolnDocument6 pagesFlucloxacillin AFTcapssolnEliza ArmanNo ratings yet
- Anesthetic Management of Non-Fasted Patients Requiring Emergency SurgeryDocument17 pagesAnesthetic Management of Non-Fasted Patients Requiring Emergency SurgeryBhi-An BatobalonosNo ratings yet
- School Nurse Investigates Classroom Mold ProblemDocument2 pagesSchool Nurse Investigates Classroom Mold ProblemMohammed Fakhouri50% (4)
- GastroschisisDocument19 pagesGastroschisiskunaidongNo ratings yet
- Mangaoang Assignment in NCM 116 LEC Perception and CoordinationDocument12 pagesMangaoang Assignment in NCM 116 LEC Perception and CoordinationDeinielle Magdangal RomeroNo ratings yet
- CNH Construction Health DeclarationDocument1 pageCNH Construction Health DeclarationEna Ahmad PieNo ratings yet
- CHARTINGDocument7 pagesCHARTINGGEN COLLANTESNo ratings yet
- Ferrous Sulfate Essential MineralDocument2 pagesFerrous Sulfate Essential MineralJoesineNo ratings yet
- Patient - Carpal Tunnel ReleaseDocument2 pagesPatient - Carpal Tunnel Releaseapi-277825138No ratings yet
- Tentorial Subdural Hematoma Following Hypertension - A Case StudyDocument3 pagesTentorial Subdural Hematoma Following Hypertension - A Case StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- PReS 2022 Final Programme Vscreen2Document88 pagesPReS 2022 Final Programme Vscreen2Mike KrikNo ratings yet
- Patel 2013Document8 pagesPatel 2013joantyy 1No ratings yet
- pGALS: A Guide to Pediatric Musculoskeletal AssessmentDocument27 pagespGALS: A Guide to Pediatric Musculoskeletal AssessmentRizqi AmaliaNo ratings yet
- JaundiceDocument30 pagesJaundiceNorakmal Andika YusriNo ratings yet
- Liver CancerDocument233 pagesLiver CancerandikhgNo ratings yet
- Clinical-Professional-Reasoning-Exam UON 2017Document17 pagesClinical-Professional-Reasoning-Exam UON 2017nathanNo ratings yet
- StressDocument128 pagesStressJulie Rose CastanedaNo ratings yet