You might also like
- First Aid For The USMLE Step1 2023Document849 pagesFirst Aid For The USMLE Step1 2023Nawal Phongtiko95% (19)
- KLS - InST - ALL - Surgical Instrument Catalog 2nd EditionDocument722 pagesKLS - InST - ALL - Surgical Instrument Catalog 2nd EditionSuryaAtmajaya25% (4)
- Internship ReportDocument39 pagesInternship ReportOdongo Isaac100% (4)
- Checking The EquipmentDocument6 pagesChecking The Equipmentapi-142637023100% (1)
- CDP ENR Management PlanDocument40 pagesCDP ENR Management PlanJacirJapsNo ratings yet
- Anaesthetic Circuits NotesDocument10 pagesAnaesthetic Circuits NotesMikemikemikeNo ratings yet
- Anaesthesia Breathing CircuitsDocument8 pagesAnaesthesia Breathing CircuitsSuresh KumarNo ratings yet
- Trach CareDocument9 pagesTrach CareserahjayneNo ratings yet
- Addis Ababa Institute of Technology: Center of Biomedical EngineeringDocument6 pagesAddis Ababa Institute of Technology: Center of Biomedical EngineeringYabNo ratings yet
- Terapi OksigenDocument33 pagesTerapi OksigenMirzaNo ratings yet
- Anaesthesia Breathing SystemsDocument15 pagesAnaesthesia Breathing SystemsSuresh KumarNo ratings yet
- Oxygen Therapy: From Wikipedia, The Free EncyclopediaDocument11 pagesOxygen Therapy: From Wikipedia, The Free EncyclopediaDadi ArdiansyahNo ratings yet
- Sistemas Respiratorios AnestesiaDocument5 pagesSistemas Respiratorios AnestesiaAiled CastroNo ratings yet
- Oxygen TherapyDocument83 pagesOxygen Therapymahmod omerNo ratings yet
- Oxygen TherapyDocument83 pagesOxygen Therapymahmod omerNo ratings yet
- Principals of AnestheticDocument13 pagesPrincipals of AnestheticRamu AryanNo ratings yet
- Lesson 5 - Oxygen TherapyDocument16 pagesLesson 5 - Oxygen TherapyDewi PrasetiaNo ratings yet
- Oxygen Therapy PDFDocument28 pagesOxygen Therapy PDFS01164503No ratings yet
- Oxygen Delivery DevicesDocument7 pagesOxygen Delivery DevicesPleural Effusion0% (1)
- Lesson 5 - Oxygen TherapyDocument16 pagesLesson 5 - Oxygen Therapygech yayeh0% (1)
- Oxygen Delivery Devices: Getting Inspired AboutDocument4 pagesOxygen Delivery Devices: Getting Inspired AboutTubagus HidayatullahNo ratings yet
- Oxygen TherapyDocument14 pagesOxygen TherapyELISION OFFICIALNo ratings yet
- Dimensionamiento Sistemas Fuentes Gases COVID19Document8 pagesDimensionamiento Sistemas Fuentes Gases COVID19Naibelly Morales EspinalNo ratings yet
- MorganDocument14 pagesMorganAdi WijayantoNo ratings yet
- Oxygen TherapyDocument33 pagesOxygen Therapyالغائب الحاضرNo ratings yet
- Low Flow AnesthesiaDocument92 pagesLow Flow Anesthesiaeliezer_89100% (1)
- Oxygen TherapyDocument40 pagesOxygen TherapySerah Ann ShajiNo ratings yet
- Chapter 5 The Patient Circuit PDFDocument8 pagesChapter 5 The Patient Circuit PDFhoan leNo ratings yet
- Low Flow AnaesthesiaDocument16 pagesLow Flow AnaesthesiaSuresh Kumar100% (1)
- O2 TherapyDocument6 pagesO2 TherapyBelle SaundersNo ratings yet
- Oxygen Therapy: Prepared By: Moza Sulaiman Rashid Al-KaldiDocument31 pagesOxygen Therapy: Prepared By: Moza Sulaiman Rashid Al-Kaldimoza92sNo ratings yet
- Oxygen DeliveryDocument6 pagesOxygen Deliveryyourdirtysocks100% (1)
- AAGBI APnoea and PreoxygenationDocument7 pagesAAGBI APnoea and PreoxygenationYee YeowNo ratings yet
- Oxygen PresentationDocument26 pagesOxygen PresentationPennyStevana100% (1)
- Oxygen Delivery SystemsDocument9 pagesOxygen Delivery Systemsanon_784834955No ratings yet
- Breathing CircuitDocument6 pagesBreathing CircuitFrits Dede SinagaNo ratings yet
- Oxygen TherapyDocument4 pagesOxygen Therapyharold smithNo ratings yet
- Anesthesia Machine1Document9 pagesAnesthesia Machine1shoibyNo ratings yet
- Modalities of Oxygen Therapy in PICU: DR Suresh Kumar. MBBS, MD, FIAP (PCC), DNB, PGDS, DM (Fellow, PCC)Document75 pagesModalities of Oxygen Therapy in PICU: DR Suresh Kumar. MBBS, MD, FIAP (PCC), DNB, PGDS, DM (Fellow, PCC)Anonymous z0QfbwY3d8No ratings yet
- Oxygen Therapy: Adel Alrihili BSN-RNDocument36 pagesOxygen Therapy: Adel Alrihili BSN-RNmacmohitNo ratings yet
- Breathing Systems: Moderator: Dr. Vinay Presenter: Dr. Rajesh KVDocument62 pagesBreathing Systems: Moderator: Dr. Vinay Presenter: Dr. Rajesh KVrajeshNo ratings yet
- Oxygen Concentrators For District Hospitals: Michael B Dobson, John Radcliffe Hospital, Oxford, UKDocument3 pagesOxygen Concentrators For District Hospitals: Michael B Dobson, John Radcliffe Hospital, Oxford, UKAwadhNo ratings yet
- Rebreathing Anesthetic Systems in Small Animal PracticeDocument8 pagesRebreathing Anesthetic Systems in Small Animal PracticeAkın SeverNo ratings yet
- DR D. Suvankar Seth G.S.MC and Kem Hospital, MumbaiDocument124 pagesDR D. Suvankar Seth G.S.MC and Kem Hospital, MumbaiAli SohailNo ratings yet
- Oxygen Therapy: Dr. Richard D. Pascua InstructorDocument91 pagesOxygen Therapy: Dr. Richard D. Pascua InstructorFranz goNo ratings yet
- Oxygen and Oxygen DeliveryDocument9 pagesOxygen and Oxygen Deliveryapi-98304344No ratings yet
- 03 Anaesthesia Machine PDFDocument0 pages03 Anaesthesia Machine PDFjuniorebindaNo ratings yet
- Anesthetics and Anesthesiology: Apneic Oxygenation and High FlowDocument7 pagesAnesthetics and Anesthesiology: Apneic Oxygenation and High FlowMuhammad SyamaniNo ratings yet
- Oxygen TherapyDocument8 pagesOxygen TherapysumNo ratings yet
- Oxygen TherapyDocument85 pagesOxygen Therapyvictoria.nickola3404No ratings yet
- The Circuit of The Typical ICU Ventilator: Skip To Main ContentDocument23 pagesThe Circuit of The Typical ICU Ventilator: Skip To Main ContentChrisNo ratings yet
- Oxygen Delivery Systems: Under Guidance of Dr. Shraddha Patel by - Dr. Dhwani PatelDocument68 pagesOxygen Delivery Systems: Under Guidance of Dr. Shraddha Patel by - Dr. Dhwani PatelDeep ShahNo ratings yet
- 13th & 14th WK - Oxygen Therapy With VideoDocument89 pages13th & 14th WK - Oxygen Therapy With VideoJesus Mario Lopez100% (1)
- Oxygen Delivery Methods ENG PRINTDocument2 pagesOxygen Delivery Methods ENG PRINTandi11No ratings yet
- Oxygen TherapyDocument25 pagesOxygen Therapypolosan123No ratings yet
- Are Those Aerosol Masks, Tracheostomy Collars, T-Tube Adapters, and Face Tents Can BeDocument1 pageAre Those Aerosol Masks, Tracheostomy Collars, T-Tube Adapters, and Face Tents Can BeJanah PagayNo ratings yet
- Oxygen TherapyDocument14 pagesOxygen TherapyEdward NewgateNo ratings yet
- CH 17Document20 pagesCH 17Maria BoccaNo ratings yet
- M8 - Investigations and Monitoring in The ICUDocument68 pagesM8 - Investigations and Monitoring in The ICUVishal KumarNo ratings yet
- OXYGENATIONISMDocument20 pagesOXYGENATIONISMChristine EmanNo ratings yet
- MedSurg Laboratory CompilationDocument141 pagesMedSurg Laboratory CompilationChristine ParrillaNo ratings yet
- Oxygen TherapyDocument8 pagesOxygen TherapyElmoi DoguilesNo ratings yet
- Respiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsFrom EverandRespiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsJian-Xin ZhouNo ratings yet
- Year 6 Clerkship - Welcome & Curriculum Class 2020 (Revised 25.04.2019)Document190 pagesYear 6 Clerkship - Welcome & Curriculum Class 2020 (Revised 25.04.2019)Ali SemajNo ratings yet
- WFTF Chamber Quantification Summary Doc Final July 18Document18 pagesWFTF Chamber Quantification Summary Doc Final July 18Saloum Muhammed IslamNo ratings yet
- Stress Ischaemic AseDocument49 pagesStress Ischaemic AseAnonymous oQtve4oNo ratings yet
- Pleural Disease (2010)Document81 pagesPleural Disease (2010)Ale EpigmenioNo ratings yet
- MDH State Rapid Response Investigative Public Report The Waters On MayowoodDocument13 pagesMDH State Rapid Response Investigative Public Report The Waters On MayowoodinforumdocsNo ratings yet
- Isotretinoin Oral Uses, Side Effects, Interactions, Pictures, Warnings & Dosing - WebMDDocument1 pageIsotretinoin Oral Uses, Side Effects, Interactions, Pictures, Warnings & Dosing - WebMDLynn Abou TayehNo ratings yet
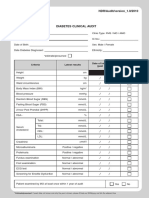
- Borang Diabetes Clinical AuditDocument2 pagesBorang Diabetes Clinical AuditHafizzah Mohd FirdausNo ratings yet
- Cerebellar Purkinje Cell ActivDocument15 pagesCerebellar Purkinje Cell ActivSergio PereleteguiNo ratings yet
- Unit 2: MBH402 Mba 4 SemesterDocument6 pagesUnit 2: MBH402 Mba 4 SemesterSáas JainNo ratings yet
- Risk List TemplateDocument3 pagesRisk List Templatemanjunathaug3No ratings yet
- Improvement in Quality MetricsDocument10 pagesImprovement in Quality MetricsGodFather xNo ratings yet
- Investigation The Effective of The Hazard Identification, Risk Assessment and Determining Control (HIRADC) in Manufacturing ProcessDocument6 pagesInvestigation The Effective of The Hazard Identification, Risk Assessment and Determining Control (HIRADC) in Manufacturing ProcessJames Laurence RavizNo ratings yet
- Medical School Pediatric Department Chairs, Inc.: Notes From The Association ofDocument4 pagesMedical School Pediatric Department Chairs, Inc.: Notes From The Association ofChristian NaranjoNo ratings yet
- Text Information and MediaDocument41 pagesText Information and MediaRegine GuavezNo ratings yet
- Doghouse BluesDocument6 pagesDoghouse Bluesnno067959No ratings yet
- Eurofit Provisional Handbook Leger Beep Test 1983Document18 pagesEurofit Provisional Handbook Leger Beep Test 1983Haisan Angel-AlexNo ratings yet
- WS00Q563 02gbDocument6 pagesWS00Q563 02gbRuwan Susantha PelawattaNo ratings yet
- G11 HOPE Module 6Document16 pagesG11 HOPE Module 6Unk NownNo ratings yet
- Shutter IslandDocument2 pagesShutter IslandMinh KhuêNo ratings yet
- Newmicrosoftofficepowerpointpresentation 160410175058 PDFDocument37 pagesNewmicrosoftofficepowerpointpresentation 160410175058 PDFDevrathNo ratings yet
- Peripheral Vascular SystemDocument3 pagesPeripheral Vascular SystemCzayanne Belle AdreceNo ratings yet
- 2022 Tribal HHAP Application - 22Document7 pages2022 Tribal HHAP Application - 22LakeCoNewsNo ratings yet
- Cues Nursing Diagnosis Scientific Basis Objectives Nursing Intervention Rationale EvaluationDocument11 pagesCues Nursing Diagnosis Scientific Basis Objectives Nursing Intervention Rationale Evaluationjoyrena ochondraNo ratings yet
- LF2F Parental Consent and Waiver FormDocument6 pagesLF2F Parental Consent and Waiver FormDreSznNo ratings yet
- Activity 2 Finals Histo Lab - EDLAY2ADocument2 pagesActivity 2 Finals Histo Lab - EDLAY2ATom Anthony TonguiaNo ratings yet
- Lesson 1 Nature of PsychologyDocument4 pagesLesson 1 Nature of PsychologyMariah A.No ratings yet
- Penggunaan Obat Farmasi 2018 FinalDocument106 pagesPenggunaan Obat Farmasi 2018 FinalSintha DewiNo ratings yet
- Module 3 Organizational Structure, Job Description and Job EvaluationDocument21 pagesModule 3 Organizational Structure, Job Description and Job EvaluationJasper Mina GerminoNo ratings yet
- PCM AssignmentDocument3 pagesPCM AssignmentRUTUJA DILIP GADENo ratings yet
- Milk Testing and QualityDocument12 pagesMilk Testing and Qualitykheng chanbormeiNo ratings yet
- Sushrut Dental Clinic: Dr. Bhagyashree Ramesh Khedkar BDS (Reg No. A-45644)Document1 pageSushrut Dental Clinic: Dr. Bhagyashree Ramesh Khedkar BDS (Reg No. A-45644)Ganesh ganiNo ratings yet