You might also like
- Experience Certificate Format Letter PDFDocument2 pagesExperience Certificate Format Letter PDFDenise0% (2)
- Mixing TipsDocument10 pagesMixing TipsyebaimNo ratings yet
- Intraoperative PhaseDocument173 pagesIntraoperative PhaseEbi100% (1)
- Environmental and Safety EnggDocument425 pagesEnvironmental and Safety Enggjustine andrei mapanaoNo ratings yet
- Medical Malpractice and Compensation in The UKDocument33 pagesMedical Malpractice and Compensation in The UKgun rayNo ratings yet
- Comparative Study of Oral Swab and Saliva Flora in Patients With Oral Cancer During Chemo - RadiotherapyDocument6 pagesComparative Study of Oral Swab and Saliva Flora in Patients With Oral Cancer During Chemo - RadiotherapyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Management of Paget Disease of The Breast With RadiotherapyDocument8 pagesManagement of Paget Disease of The Breast With RadiotherapyAndreas Ronald100% (1)
- Esophageal CancerDocument34 pagesEsophageal CancerEzequiel GarciaNo ratings yet
- Ghid Anestezie Locala PDFDocument19 pagesGhid Anestezie Locala PDFanaNo ratings yet
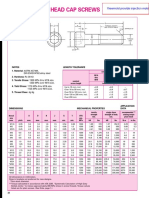
- Metric Socket Head Cap ScrewsDocument2 pagesMetric Socket Head Cap ScrewsImam MulyonoNo ratings yet
- Lab Man ProposalDocument2 pagesLab Man ProposalAbdon Delfin Jr.No ratings yet
- CA Prostate by Dr. Musaib MushtaqDocument71 pagesCA Prostate by Dr. Musaib MushtaqDr. Musaib MushtaqNo ratings yet
- BP1800 D Extended Rock Spare Parts Manual Edition - Aug '08Document162 pagesBP1800 D Extended Rock Spare Parts Manual Edition - Aug '08komalinternational5No ratings yet
- Yeung H Et Al 2012. Patient Reported Reasons For The Discontinuation of Commonly Used Treatments For Moderate To Severe PsoriasisDocument9 pagesYeung H Et Al 2012. Patient Reported Reasons For The Discontinuation of Commonly Used Treatments For Moderate To Severe PsoriasisAndi MarsaliNo ratings yet
- BWM ProjectDocument26 pagesBWM ProjectAnil singh baisNo ratings yet
- Antimicrobial Resistance in Libya - 1970-2011Document8 pagesAntimicrobial Resistance in Libya - 1970-2011Khalifa Sifaw Ghenghesh100% (2)
- 2011 Nosocomial Infections - Knowledge and Source of Information Among Clinical Health Care Students in GhanaDocument4 pages2011 Nosocomial Infections - Knowledge and Source of Information Among Clinical Health Care Students in GhanaMostafa AbdelrahmanNo ratings yet
- Hemophilia: Presented By, Mrs. Arifa T N Child Health Nursing Second Year M.SC Nursing Mims ConDocument43 pagesHemophilia: Presented By, Mrs. Arifa T N Child Health Nursing Second Year M.SC Nursing Mims ConSilpa Jose T100% (1)
- Skintox Practiceguidelines EGFR SCCDocument17 pagesSkintox Practiceguidelines EGFR SCCFelpnilNo ratings yet
- Who Patient SafetyDocument14 pagesWho Patient SafetyJuwita Valen RamadhanniaNo ratings yet
- Determination of Social Impact and Public PurposeDocument14 pagesDetermination of Social Impact and Public PurposeDr. Jaspreet Kaur MajithiaNo ratings yet
- Anesthesia For Hysteroscopy: A Comparison of General and Spinal AnesthesiaDocument7 pagesAnesthesia For Hysteroscopy: A Comparison of General and Spinal AnesthesiaIJAR JOURNALNo ratings yet
- Complications of Diabetes Mellitus-UpdateDocument48 pagesComplications of Diabetes Mellitus-UpdateAnditha Namira RS100% (1)
- Communicable Diseases 1Document75 pagesCommunicable Diseases 1victorNo ratings yet
- Pathology of Female Genital System, 2024Document63 pagesPathology of Female Genital System, 2024Eslam HamadaNo ratings yet
- Gui322cpg1504e2 PDFDocument15 pagesGui322cpg1504e2 PDFieo100% (1)
- Handhygiene Azzapresentation1final 131028093002 Phpapp02Document34 pagesHandhygiene Azzapresentation1final 131028093002 Phpapp02Rahul100% (1)
- 11 Uterine CancerDocument43 pages11 Uterine Cancerclaire yowsNo ratings yet
- Endometrial Malignancies 1Document41 pagesEndometrial Malignancies 1jerrydanfordfxNo ratings yet
- DC HCCDocument12 pagesDC HCCSamah Abd ElhamidNo ratings yet
- Enhanced Recovery After Elective Caesarean A RapidDocument11 pagesEnhanced Recovery After Elective Caesarean A Rapidselfie rijalNo ratings yet
- Chemotherapy Administration in Pediatric: An OverviewDocument76 pagesChemotherapy Administration in Pediatric: An OverviewMiftaa HurrahmiNo ratings yet
- GYNE Endometrial Hyperplasia Dr. Ahyong Reyes Sleepy CrammersDocument3 pagesGYNE Endometrial Hyperplasia Dr. Ahyong Reyes Sleepy CrammersMiguel Luis NavarreteNo ratings yet
- Otitis Externa: Straight To The Point of CareDocument45 pagesOtitis Externa: Straight To The Point of CareNana OkujavaNo ratings yet
- Medicolegal NSGDocument45 pagesMedicolegal NSGIvy Nelly100% (1)
- Biosafety and Regulations Presentation On BioterrorismDocument32 pagesBiosafety and Regulations Presentation On BioterrorismGagan KhuranaNo ratings yet
- Knowledge, Attitude and Practice Toward Cervical Cancer and Cervical Cancer Screening and Its Associated Factors Among Women in The City of Bamenda, CameroonDocument17 pagesKnowledge, Attitude and Practice Toward Cervical Cancer and Cervical Cancer Screening and Its Associated Factors Among Women in The City of Bamenda, CameroonEditor IJTSRDNo ratings yet
- ExudateDocument19 pagesExudateFaiq Nadiatul Mardia AsaNo ratings yet
- BIRADS Lexicon and Its Histopathological Corroboration in The Diagnosis of Breast LesionsDocument7 pagesBIRADS Lexicon and Its Histopathological Corroboration in The Diagnosis of Breast LesionsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- WEEK 13 Alterations With Infectious Inflammatory and Immunologic Responses Pedia OncoDocument105 pagesWEEK 13 Alterations With Infectious Inflammatory and Immunologic Responses Pedia Oncorising starNo ratings yet
- Ijms 22 08167 v3Document10 pagesIjms 22 08167 v3pilyoungg1994No ratings yet
- A Review of Novel Technologies and Techniques Associated With Identification of Bloodstream Infection Etiologies PDFDocument14 pagesA Review of Novel Technologies and Techniques Associated With Identification of Bloodstream Infection Etiologies PDFGRAÇAS PERFUMARIANo ratings yet
- Therapeutic Management of Clinical Mastitis in Goat: A Case StudyDocument5 pagesTherapeutic Management of Clinical Mastitis in Goat: A Case StudyIJAR JOURNALNo ratings yet
- Surgical Access IncisionsDocument7 pagesSurgical Access IncisionsFiliberto RiosNo ratings yet
- PHD Seminar (Oral Cancer) (Prasad Rathod)Document31 pagesPHD Seminar (Oral Cancer) (Prasad Rathod)Apurv SoniNo ratings yet
- Stochastic Blockmodels Meet Graph Neural NetworksDocument17 pagesStochastic Blockmodels Meet Graph Neural NetworksSoniya RangnaniNo ratings yet
- Impact of Applying Artificial Intelligence: Healthcare Professionals Insight (A Qualitative Survey Study in Hafr-Elbatin, Saudi Arabia)Document8 pagesImpact of Applying Artificial Intelligence: Healthcare Professionals Insight (A Qualitative Survey Study in Hafr-Elbatin, Saudi Arabia)IJAR JOURNALNo ratings yet
- Journal 4Document5 pagesJournal 4dr. Nadia Salsabila100% (1)
- Pharmacological Management of Pulmonary EmbolismDocument49 pagesPharmacological Management of Pulmonary EmbolismDaniela Rojas CorreaNo ratings yet
- LYMPHOGRAPHY-WPS OfficeDocument11 pagesLYMPHOGRAPHY-WPS OfficePax Giuseppe0% (1)
- Cleidocranial Dysplasia A Review of Clinical Radiological Genetic Implications and Guidelines ProposalDocument8 pagesCleidocranial Dysplasia A Review of Clinical Radiological Genetic Implications and Guidelines ProposalGina Alexandra Aldana PortelaNo ratings yet
- NoThing Left Behind Policy v5 PDFDocument54 pagesNoThing Left Behind Policy v5 PDFO.r. Cadz100% (1)
- GS1 Anti-Counterfeiting White PaperDocument24 pagesGS1 Anti-Counterfeiting White PaperRashed MohammadNo ratings yet
- Hand Hygiene Journal HelminaDocument12 pagesHand Hygiene Journal Helminajoko samudro100% (1)
- Endometrial Cancer ESMO Clinical Practice GuidelinesDocument5 pagesEndometrial Cancer ESMO Clinical Practice Guidelinesjhon heriansyahNo ratings yet
- Obesity Core Curriculum 2020Document9 pagesObesity Core Curriculum 2020Adina BrahaNo ratings yet
- Ibi JurnalDocument9 pagesIbi JurnalRiski Pradika 2017No ratings yet
- Ethics Unit 2Document22 pagesEthics Unit 2SaniNo ratings yet
- 1 Role of Ultrasound in The Evaluation of Acute Pelvic PainDocument11 pages1 Role of Ultrasound in The Evaluation of Acute Pelvic PainGhofran Ibrahim HassanNo ratings yet
- Communicating in Public Health Emergencies EnglishDocument32 pagesCommunicating in Public Health Emergencies EnglishGail HoadNo ratings yet
- Knowledge and Practices of Radiographers Regarding Infection Control in Radiology Departments in MalawiDocument5 pagesKnowledge and Practices of Radiographers Regarding Infection Control in Radiology Departments in MalawiAna ResendesNo ratings yet
- Otomycosis in Western Iran: Clinical and Mycological AspectsDocument5 pagesOtomycosis in Western Iran: Clinical and Mycological AspectsLiz TorresNo ratings yet
- Review of New Antibiotics For Multidrug Resistant Bacterial StrainsDocument7 pagesReview of New Antibiotics For Multidrug Resistant Bacterial StrainsIJRASETPublicationsNo ratings yet
- Prevalence of Schizophrenia Among Patients Admitted Into Neuro-Psychiatric Hospital, Rumuigbo, Port Harcourt, Rivers State, NigeriaDocument9 pagesPrevalence of Schizophrenia Among Patients Admitted Into Neuro-Psychiatric Hospital, Rumuigbo, Port Harcourt, Rivers State, NigeriaSteven JonesNo ratings yet
- Non-Diagnostic CT-Guided Percutaneous Needle BiopsyDocument12 pagesNon-Diagnostic CT-Guided Percutaneous Needle BiopsyHeru SigitNo ratings yet
- 14 BaruDocument18 pages14 BaruAnditha Namira RSNo ratings yet
- 13 BaruDocument9 pages13 BaruAnditha Namira RSNo ratings yet
- 4 BaruDocument4 pages4 BaruAnditha Namira RSNo ratings yet
- 11 BaruDocument3 pages11 BaruAnditha Namira RSNo ratings yet
- Enhanced Recovery After Surgery in Gynecology: A Review of The LiteratureDocument17 pagesEnhanced Recovery After Surgery in Gynecology: A Review of The LiteratureAnditha Namira RSNo ratings yet
- Enhanced Recovery After Surgery: It's Time To Change Practice!Document12 pagesEnhanced Recovery After Surgery: It's Time To Change Practice!Anditha Namira RSNo ratings yet
- 2 BaruDocument28 pages2 BaruAnditha Namira RSNo ratings yet
- Reproductive Biology and EndocrinologyDocument4 pagesReproductive Biology and EndocrinologyAnditha Namira RSNo ratings yet
- Daley JMDocument9 pagesDaley JMAnditha Namira RSNo ratings yet
- 3 BaruDocument17 pages3 BaruAnditha Namira RSNo ratings yet
- Daftar Pustaka Oma UsuDocument4 pagesDaftar Pustaka Oma UsuAnditha Namira RSNo ratings yet
- Introduction To Metabolism: Departemen Fisiologi Fakultas Kedokteran USUDocument22 pagesIntroduction To Metabolism: Departemen Fisiologi Fakultas Kedokteran USUAnditha Namira RSNo ratings yet
- Daftar Pustaka Oma UsuDocument4 pagesDaftar Pustaka Oma UsuAnditha Namira RSNo ratings yet
- AcsDocument57 pagesAcsAnditha Namira RSNo ratings yet
- LYMPHOMADocument32 pagesLYMPHOMAAnditha Namira RSNo ratings yet
- CHM 101 Exams 20182019 Type B-1Document4 pagesCHM 101 Exams 20182019 Type B-1balikisolayemi2005No ratings yet
- Test Bank For Human Resource Management 13th Edition MathisDocument13 pagesTest Bank For Human Resource Management 13th Edition Mathisporkwood.separate.kumtf100% (46)
- Department of Education: Schools Division of Nueva EcijaDocument6 pagesDepartment of Education: Schools Division of Nueva EcijaRyan AlapNo ratings yet
- Sociol 2z03, Spring 2022, Z. LuoDocument6 pagesSociol 2z03, Spring 2022, Z. LuoGarcía MarlinhoNo ratings yet
- (2009) B. H. GebreslassieDocument10 pages(2009) B. H. GebreslassieHusnain AliNo ratings yet
- Me-101 Tutorial 04 SolutionsDocument8 pagesMe-101 Tutorial 04 SolutionsVasanthi ChitturiNo ratings yet
- Data Grid ViewDocument68 pagesData Grid ViewdflyNo ratings yet
- Understanding ASEAN: Its Systems & StructuresDocument59 pagesUnderstanding ASEAN: Its Systems & StructureskaiaceegeesNo ratings yet
- Iron Through The Ages: Alan W. PenseDocument11 pagesIron Through The Ages: Alan W. PenseMohamed IsmailNo ratings yet
- Decorative Metals (r1)Document23 pagesDecorative Metals (r1)irshad khanNo ratings yet
- MAF603 2016 June SolutionDocument8 pagesMAF603 2016 June Solutionanis izzati100% (1)
- Shamsuddin Et Al., 2008 - Demand Analyses of Rice in MalaysiaDocument21 pagesShamsuddin Et Al., 2008 - Demand Analyses of Rice in MalaysiaHannah LeeNo ratings yet
- Capital Market and Intermediaries NotesDocument62 pagesCapital Market and Intermediaries NoteslavanyaNo ratings yet
- Operation INVERTRONIC Compact 1.5-22.5kVA: Operating InstructionsDocument101 pagesOperation INVERTRONIC Compact 1.5-22.5kVA: Operating InstructionsAlejandro Garcia MNo ratings yet
- Schema de Instalare Sitem Presurizare 1Document1 pageSchema de Instalare Sitem Presurizare 1Cujba CodrinNo ratings yet
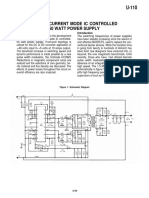
- Slua 053Document13 pagesSlua 053carlosibaNo ratings yet
- Hvac QuestionDocument12 pagesHvac QuestionMuhamed Elsayed - ZalatNo ratings yet
- Karl Liebknecht - in Spite of Everything! (1919)Document4 pagesKarl Liebknecht - in Spite of Everything! (1919)Luka ENo ratings yet
- Essay Class 03-NotesDocument2 pagesEssay Class 03-NotesDurga SinghNo ratings yet
- A Study of Performance Appraisal and Employee S Performance by Measuring The Latest Role of Motivation in An OrganizationDocument6 pagesA Study of Performance Appraisal and Employee S Performance by Measuring The Latest Role of Motivation in An Organizationrakesh kumarNo ratings yet
- SD Modul 9-10 Hash TableDocument12 pagesSD Modul 9-10 Hash TableEdi FaizalNo ratings yet
- Learn SQL - Aggregate Functions Cheatsheet - CodecademyDocument2 pagesLearn SQL - Aggregate Functions Cheatsheet - CodecademyOptimus PrimeNo ratings yet
- Answer The Following Questions Very CarefullyDocument2 pagesAnswer The Following Questions Very CarefullyMaham ImtiazNo ratings yet
- Reinforced and Prestressed Concrete II - CEDocument3 pagesReinforced and Prestressed Concrete II - CEAlina OpreanNo ratings yet
- Deniable Encryption : Email: Ema L: Ema LDocument15 pagesDeniable Encryption : Email: Ema L: Ema LlanaNo ratings yet