You might also like
- Surviving SAP Implementation in A HospitalDocument25 pagesSurviving SAP Implementation in A Hospitalhadia zahoor33% (6)
- Physicians Desk ReferenceDocument4 pagesPhysicians Desk Referenceapi-280857978No ratings yet
- M.pharm SyllabusDocument47 pagesM.pharm SyllabustusharphaleNo ratings yet
- Rayner Et Al., Lercanidipine in TX Naive HPT Patients. Pragmatic and Observational Research 2019Document6 pagesRayner Et Al., Lercanidipine in TX Naive HPT Patients. Pragmatic and Observational Research 2019Ruth RachmawatyNo ratings yet
- Clinical Pharmacology 223-228 26Document6 pagesClinical Pharmacology 223-228 26Ankit AgarwalNo ratings yet
- Treatment of Liver Cirrhosis: Berliba Elina, MDDocument92 pagesTreatment of Liver Cirrhosis: Berliba Elina, MDRadu TuguiNo ratings yet
- Servefile CFMDocument9 pagesServefile CFMLUIS ALFREDO SALGADO FLORESNo ratings yet
- Paper Journal Club 1Document7 pagesPaper Journal Club 1Jikai ZenNo ratings yet
- Guidelines For Severe CapDocument6 pagesGuidelines For Severe CapReynaldoBinsarNo ratings yet
- Barbarino 2014Document7 pagesBarbarino 2014Andrean ZukempotNo ratings yet
- A Review On Epileptic Treatment by LevetiracetamDocument6 pagesA Review On Epileptic Treatment by LevetiracetamEditor IJTSRDNo ratings yet
- Separations 07 00047 PDFDocument11 pagesSeparations 07 00047 PDF5netNo ratings yet
- Rivaroxaban Vs Apixaban Adherence in Real Life 2018Document13 pagesRivaroxaban Vs Apixaban Adherence in Real Life 2018akhilNo ratings yet
- Antiviral TherapyDocument19 pagesAntiviral TherapyMalueth AnguiNo ratings yet
- Antiviral Treatment Failures After TransplantationDocument5 pagesAntiviral Treatment Failures After TransplantationRogelio MoscosoNo ratings yet
- (Abacavir Sulfate) Tablets and Oral Solution: Adult PatientsDocument2 pages(Abacavir Sulfate) Tablets and Oral Solution: Adult PatientsChoco MuchoNo ratings yet
- Case Reports 2Document58 pagesCase Reports 2Tarik PlojovicNo ratings yet
- Drug Interactions in Hiv PatientsDocument86 pagesDrug Interactions in Hiv PatientsmeghaNo ratings yet
- Daftar PustakaDocument16 pagesDaftar PustakaDestrie CindyNo ratings yet
- Puig 2013Document21 pagesPuig 2013Nestor MNo ratings yet
- Nevirapine Drug .Document11 pagesNevirapine Drug .AminaNo ratings yet
- Tohen 2003Document9 pagesTohen 2003Francisco VillalonNo ratings yet
- LA Dosing and Toxicity of Adult Truncal CathetersDocument14 pagesLA Dosing and Toxicity of Adult Truncal CathetersMuhammad Azam Mohd NizaNo ratings yet
- Success of (NS5BNS5A Inhibitors) SofosbuvirVelpatasvir in Management Hepatitis C Studied Tertiary Care Healthcare in Rawalpindi, PakistanDocument6 pagesSuccess of (NS5BNS5A Inhibitors) SofosbuvirVelpatasvir in Management Hepatitis C Studied Tertiary Care Healthcare in Rawalpindi, PakistanInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Molecules: Anti-Inflammatory Action and Mechanisms of ResveratrolDocument15 pagesMolecules: Anti-Inflammatory Action and Mechanisms of ResveratrolDito AnurogoNo ratings yet
- Long-Acting Cabotegravir and Rilpivirine For Maintenance of HIV-1Document9 pagesLong-Acting Cabotegravir and Rilpivirine For Maintenance of HIV-1Alan SantoyoNo ratings yet
- Clinical Worksheet - PortfolioDocument3 pagesClinical Worksheet - Portfolioapi-691262000No ratings yet
- Pityriasis Versicolor: An Update On Pharmacological Treatment OptionsDocument7 pagesPityriasis Versicolor: An Update On Pharmacological Treatment OptionsEva ParamithaNo ratings yet
- Navirapine DrugDocument38 pagesNavirapine DrugAminaNo ratings yet
- 25 30ijpdtDocument7 pages25 30ijpdtSalsa BilaNo ratings yet
- Cabenuva Pi Pil Ifu2 Ifu3Document74 pagesCabenuva Pi Pil Ifu2 Ifu3Zachariah Paul GiovanniNo ratings yet
- Parameters of Fluid Responsiveness Curr Op Crit Care Shi2020Document8 pagesParameters of Fluid Responsiveness Curr Op Crit Care Shi2020Tadeo PradoNo ratings yet
- Cabenuva - The First Long-Acting Regimen For HIV TreatmentDocument13 pagesCabenuva - The First Long-Acting Regimen For HIV TreatmentAlan SantoyoNo ratings yet
- Journal Homepage: - : IntroductionDocument8 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Intravenous Fluid Resuscitation in The ManagementDocument8 pagesIntravenous Fluid Resuscitation in The ManagementRicardo Isique SantillanNo ratings yet
- Materi Narsum I - ARV Dan KloroquinDocument35 pagesMateri Narsum I - ARV Dan KloroquinEndah PurwaningsihNo ratings yet
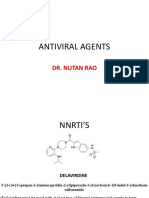
- Antiviral Agents: Dr. Nutan RaoDocument18 pagesAntiviral Agents: Dr. Nutan RaoNutan Desai RaoNo ratings yet
- S 000 LBLDocument54 pagesS 000 LBLNavin GuptaNo ratings yet
- Benign Paroxysmal Positional Vertigo: Comparison of Two Recent International GuidelinesDocument42 pagesBenign Paroxysmal Positional Vertigo: Comparison of Two Recent International GuidelinesFika FathiaNo ratings yet
- 1549 Full-2Document7 pages1549 Full-2balqiswulanNo ratings yet
- Lithium, Carbamazepine and Valproate in Acute ManiaDocument6 pagesLithium, Carbamazepine and Valproate in Acute ManiaGading AuroraNo ratings yet
- Resistance in HCV: Andrew J. Muir, MD MHSDocument33 pagesResistance in HCV: Andrew J. Muir, MD MHSEleni HagosNo ratings yet
- Favipiravir: Pharmacokinetics and Concerns About Clinical Trials For 2019-Ncov InfectionDocument6 pagesFavipiravir: Pharmacokinetics and Concerns About Clinical Trials For 2019-Ncov InfectionJuan Felipe Herrera WilchesNo ratings yet
- Yan and Kreek 2018 Alcohol StressDocument12 pagesYan and Kreek 2018 Alcohol StressChon-wa CheongNo ratings yet
- Rivaroxaban Xarelto Requiring Emergency Surgery or Treatment For HaemorrhageDocument7 pagesRivaroxaban Xarelto Requiring Emergency Surgery or Treatment For HaemorrhageRomeo-Remus RaffaiNo ratings yet
- Savera LiteratureDocument7 pagesSavera LiteratureMusharaf ShahNo ratings yet
- JPNR 2022 S01 216+ (1815 1822)Document8 pagesJPNR 2022 S01 216+ (1815 1822)prabaNo ratings yet
- Lopinavir 9Document9 pagesLopinavir 9นิวนิ่วนิ้ว ศิษย์ปตทNo ratings yet
- NIV Algorithm Final Version Jan 2020Document3 pagesNIV Algorithm Final Version Jan 2020AmalNo ratings yet
- Molecular Pharmacokinetics of Catharanthus (Vinca) AlkaloidsDocument11 pagesMolecular Pharmacokinetics of Catharanthus (Vinca) AlkaloidsLuciana OliveiraNo ratings yet
- Jurnal BE ValsartanDocument10 pagesJurnal BE ValsartanFutisya AlvitaNo ratings yet
- Jurnal Bahasa InggrisDocument8 pagesJurnal Bahasa InggrisChristine Yohana SianturiNo ratings yet
- Ropivacaine Vs Bupivacaine PDFDocument6 pagesRopivacaine Vs Bupivacaine PDFJessica LawrenceNo ratings yet
- What Is The Role of Remdesivir in Patients With.7Document6 pagesWhat Is The Role of Remdesivir in Patients With.7FIA SlotNo ratings yet
- Carba Efavirenz 2008Document10 pagesCarba Efavirenz 2008Dra Carolina Escalante Neurologa de AdultosNo ratings yet
- Review of Levetiracetam With A Focus On The Extended Release Formulation As Adjuvant Therapy in Controlling Partial-Onset SeizuresDocument11 pagesReview of Levetiracetam With A Focus On The Extended Release Formulation As Adjuvant Therapy in Controlling Partial-Onset Seizuresnourdr0No ratings yet
- Ijprs QZN 2014Document13 pagesIjprs QZN 2014Jayshree PatilNo ratings yet
- CDC HCTB Technical Webinar Long Acting March 2023Document21 pagesCDC HCTB Technical Webinar Long Acting March 2023drfathurrizkyNo ratings yet
- LENACAPAVIRDocument11 pagesLENACAPAVIRAhmed ElgenaidyNo ratings yet
- Role of Vitamin A in The Immune SystemDocument16 pagesRole of Vitamin A in The Immune SystemAmaliyah RohmahNo ratings yet
- WJD 5 57Document9 pagesWJD 5 57Fifit SiePutry BintaNgnya KudaciNo ratings yet
- Pharmacology for Student and Pupil Nurses and Students in Associated ProfessionsFrom EverandPharmacology for Student and Pupil Nurses and Students in Associated ProfessionsNo ratings yet
- LyophilizationDocument19 pagesLyophilizationSulastari CahyaniNo ratings yet
- List of Participants - Refresher Course - ARCP - October 2021Document16 pagesList of Participants - Refresher Course - ARCP - October 2021PRATIK CHAUHAN100% (1)
- Fentanyl Fact Sheet 508c 1Document2 pagesFentanyl Fact Sheet 508c 1api-160935984No ratings yet
- Evaluation of Parenterals PDFDocument2 pagesEvaluation of Parenterals PDFSarahNo ratings yet
- Medication Use Policy - AMHCDocument21 pagesMedication Use Policy - AMHCeliasNo ratings yet
- Chikitsa ChatuspadDocument2 pagesChikitsa ChatuspadAnand YadavNo ratings yet
- Dosage Based On Body WeightDocument8 pagesDosage Based On Body WeightPhoebe GandaNo ratings yet
- Simple Magazine #17Document5 pagesSimple Magazine #17tôn thất minh khangNo ratings yet
- Pharmacovigilance Directive English 2020Document26 pagesPharmacovigilance Directive English 2020Zelalem KetemaNo ratings yet
- CRO CompaniesDocument195 pagesCRO CompaniesRakesh KottaNo ratings yet
- Narcotics InvestigationDocument77 pagesNarcotics Investigationkaren100% (2)
- Must Undergraduate Call 2024-2025 - 240310 - 151757Document4 pagesMust Undergraduate Call 2024-2025 - 240310 - 151757ckamusiime2No ratings yet
- The Potential Risks of Carcinogens, Mutagens and Substances Toxic To Reproduction When These Substances Are Used As Excipients of Medicinal Products For Human UseDocument12 pagesThe Potential Risks of Carcinogens, Mutagens and Substances Toxic To Reproduction When These Substances Are Used As Excipients of Medicinal Products For Human UseGaoussou TimitéNo ratings yet
- Off Label DrugsDocument3 pagesOff Label DrugsMADEINTHEEAST KeNo ratings yet
- Daftar Kebutuhan Obat MTQDocument2 pagesDaftar Kebutuhan Obat MTQDian hariyantiNo ratings yet
- Consumer SurveyDocument18 pagesConsumer SurveyJahnvi DoshiNo ratings yet
- Quick Reference To Psychotropic Medications: AntidepressantsDocument2 pagesQuick Reference To Psychotropic Medications: AntidepressantsNaiana PaulaNo ratings yet
- Medication Routes and FormsDocument7 pagesMedication Routes and FormsEdwin Emir Silva MartinezNo ratings yet
- Emergence of MDR-TBDocument18 pagesEmergence of MDR-TBAmor SantiagoNo ratings yet
- Excel Civil Engineering EstimatesDocument29 pagesExcel Civil Engineering EstimatesrohitNo ratings yet
- Hand Out Ppavd.Document4 pagesHand Out Ppavd.Hæłíę SikuarieNo ratings yet
- One View by AKTU SDC TeamDocument3 pagesOne View by AKTU SDC TeamBrijwasi Rohit jiNo ratings yet
- Module 1 IcamDocument2 pagesModule 1 IcamGE SalenNo ratings yet
- Ilam Hospital ProfileDocument29 pagesIlam Hospital ProfileADITYANo ratings yet
- Gastro Recommendation DCGI SecDocument3 pagesGastro Recommendation DCGI SecDipan KadiaNo ratings yet
- Ebook Pharmacotherapy Casa Patient Focused Approach 11Th Edition PDF Full Chapter PDFDocument67 pagesEbook Pharmacotherapy Casa Patient Focused Approach 11Th Edition PDF Full Chapter PDFmerlin.mitchell336100% (31)
- Lecture 01 PDFDocument71 pagesLecture 01 PDFKimNo ratings yet