You might also like
- Special Procudure (UGIS) : Body Habitus HyposthenicDocument12 pagesSpecial Procudure (UGIS) : Body Habitus HyposthenicJoeriz Bartolome100% (1)
- An Introduction To Insulin TherapyDocument23 pagesAn Introduction To Insulin TherapyOrion JohnNo ratings yet
- A List of Topics Covered in The SMLE Medical ExaminationDocument2 pagesA List of Topics Covered in The SMLE Medical ExaminationCanadaQBankNo ratings yet
- Aspirin OverdoseDocument3 pagesAspirin OverdoseSaputra BismaNo ratings yet
- Case Presentation COPDDocument25 pagesCase Presentation COPDBenfranson Benoza III0% (1)
- StammBerger 1990Document14 pagesStammBerger 1990OtorrinolaringologíaLoayza100% (1)
- OSODROENTDocument82 pagesOSODROENTAvner TolentinoNo ratings yet
- Determinants of Fitness Level Influencing The Morbidity Rate of Palembang's Hajj PilgrimsDocument12 pagesDeterminants of Fitness Level Influencing The Morbidity Rate of Palembang's Hajj PilgrimsSessa MagabeNo ratings yet
- Mass Gathering Medecine Hajj PilgrimageDocument10 pagesMass Gathering Medecine Hajj PilgrimageAmira Moch ZakiNo ratings yet
- Healthcare 10 00105 v2Document13 pagesHealthcare 10 00105 v2Madawi AlotaibiNo ratings yet
- 2.prevalen Mers CovDocument6 pages2.prevalen Mers CovMela Agusti WidyasariNo ratings yet
- The Examination of Sleep Quality For FroDocument9 pagesThe Examination of Sleep Quality For FrowalkensiocsNo ratings yet
- RMV 2225Document18 pagesRMV 2225Iziza LunaskhiNo ratings yet
- Risk Factors For Respiratory Death Among IndonesiaDocument8 pagesRisk Factors For Respiratory Death Among IndonesiasariNo ratings yet
- Surveilans Kesehatan HajiDocument14 pagesSurveilans Kesehatan Hajimeida putriNo ratings yet
- Ijerph 17 04925Document14 pagesIjerph 17 04925Andromax AndroNo ratings yet
- Surveilans Jamaah Haji Di SurabayaDocument14 pagesSurveilans Jamaah Haji Di SurabayaNenik PrayantiNo ratings yet
- JML 2021 0364Document5 pagesJML 2021 0364annafebrinaputriNo ratings yet
- Proporsi Dan Sebaran Faktor Risiko Eksaserbasi Akut HajiDocument10 pagesProporsi Dan Sebaran Faktor Risiko Eksaserbasi Akut HajiRizka NurilhamNo ratings yet
- Implementation of Haji Health Surveillance System in The Health City of SurabayaDocument14 pagesImplementation of Haji Health Surveillance System in The Health City of SurabayaMin YoungNo ratings yet
- Jurnal Seasonal Influenza Vaccination Among Older Adults in Jordan Prevalence Knowledge and AttitudesDocument6 pagesJurnal Seasonal Influenza Vaccination Among Older Adults in Jordan Prevalence Knowledge and AttitudesMusdaliva Tri Riskiani AlminNo ratings yet
- The Prevalence of COVID-19 in Jizan Region-Saudi Arabia A Demographic AnalysisDocument4 pagesThe Prevalence of COVID-19 in Jizan Region-Saudi Arabia A Demographic Analysiseditorial.boardNo ratings yet
- 6MINUTEWALKTESTABERTODocument5 pages6MINUTEWALKTESTABERTOpv7j8j6q5rNo ratings yet
- Contemporary Clinical Trials CommunicationsDocument7 pagesContemporary Clinical Trials CommunicationsSuci ApriliaNo ratings yet
- The Saudi Initiative For Asthma - 2019 Update: Guidelines For The Diagnosis and Management of Asthma in Adults and ChildrenDocument46 pagesThe Saudi Initiative For Asthma - 2019 Update: Guidelines For The Diagnosis and Management of Asthma in Adults and Childrenkhalid alharbiNo ratings yet
- Attitude Anxiety and Behavior Practices Regarding COVID 19 Among University Students in Jordan.a Cross Sectional StudyDocument7 pagesAttitude Anxiety and Behavior Practices Regarding COVID 19 Among University Students in Jordan.a Cross Sectional StudydauntlessNo ratings yet
- RSPR - Volume 21 - Issue 1 - Pages 96-103Document8 pagesRSPR - Volume 21 - Issue 1 - Pages 96-103jinsi georgeNo ratings yet
- Original ArticleDocument8 pagesOriginal ArticleRania T.No ratings yet
- All Articles Certs 27 Aug UpdatedDocument42 pagesAll Articles Certs 27 Aug Updatedmohammadrezahajian12191No ratings yet
- Smoking 2Document7 pagesSmoking 2fatimahNo ratings yet
- Pab MS 2112 225Document10 pagesPab MS 2112 225Ali KhanNo ratings yet
- A Preventive Role of Exercise Across The Coronavirus 2 (SARS-CoV-2) PandemicDocument8 pagesA Preventive Role of Exercise Across The Coronavirus 2 (SARS-CoV-2) PandemicHansCristopherSaegerPizarroNo ratings yet
- Jurnal HajiDocument7 pagesJurnal HajiRezka Gustya SariNo ratings yet
- Jarelnape Et Al (2016)Document7 pagesJarelnape Et Al (2016)Tengku EltrikanawatiNo ratings yet
- Exploring Knowledge and Attitude Toward Middle Eas PDFDocument8 pagesExploring Knowledge and Attitude Toward Middle Eas PDFbalqeesNo ratings yet
- Cecep Eli Kosasih Tetti Solehati Tetti Solehati Mamat LukmanDocument8 pagesCecep Eli Kosasih Tetti Solehati Tetti Solehati Mamat LukmanYARNI NABUASANo ratings yet
- Early Therapy Improves Outcomes of Exacerbations of Chronic Obstructive Pulmonary DiseaseDocument6 pagesEarly Therapy Improves Outcomes of Exacerbations of Chronic Obstructive Pulmonary DiseasenarykNo ratings yet
- Outpatient Pulmonary RehabilitDocument10 pagesOutpatient Pulmonary Rehabilitelieser toding mendilaNo ratings yet
- New 2Document5 pagesNew 2AMELIA ULMNo ratings yet
- Panitchote2019 Article FactorsAssociatedWithAcuteKidnDocument10 pagesPanitchote2019 Article FactorsAssociatedWithAcuteKidnBernard NazaraNo ratings yet
- 1 PBDocument6 pages1 PBakbarsepadanNo ratings yet
- BMC Public Health: Which Preventive Measures Might Protect Health Care Workers From SARS?Document8 pagesBMC Public Health: Which Preventive Measures Might Protect Health Care Workers From SARS?Rahel YaserNo ratings yet
- Reabilitação Nas Doenças IntersticiaisDocument13 pagesReabilitação Nas Doenças IntersticiaisBruno AlmeidaNo ratings yet
- Practice On Pulmonary Hygiene and Associated Factors Among Health Professionals Working in Two Government Hospitals at Amhara, EthiopiaDocument4 pagesPractice On Pulmonary Hygiene and Associated Factors Among Health Professionals Working in Two Government Hospitals at Amhara, EthiopiaayuNo ratings yet
- Public Knowledge of Pulmonary Tuberculosis.: Annals of Thoracic Medicine July 2011Document7 pagesPublic Knowledge of Pulmonary Tuberculosis.: Annals of Thoracic Medicine July 2011hidayatus solihinNo ratings yet
- Assessment of The Awareness, Perception, Attitudes, and Preparedness of Health-Care Professionals Potentially Exposed To COVID-19 in The United Arab EmiratesDocument12 pagesAssessment of The Awareness, Perception, Attitudes, and Preparedness of Health-Care Professionals Potentially Exposed To COVID-19 in The United Arab EmiratesSarah SanadNo ratings yet
- 4 Jurnal Alotaibi 2019Document16 pages4 Jurnal Alotaibi 2019Charis MurwadiNo ratings yet
- 2019-Enfermeria Clinica (Scopus Q-3)Document6 pages2019-Enfermeria Clinica (Scopus Q-3)Muhamad Jauhar S.Kep., Ners, M.KepNo ratings yet
- 1 s2.0 S1939455121001174 MainDocument11 pages1 s2.0 S1939455121001174 MainNafiza SyarafinaNo ratings yet
- 10 11648 J CCR 20200403 15Document7 pages10 11648 J CCR 20200403 15NjeodoNo ratings yet
- Travel-Related Respiratory Symptoms and InfectionDocument5 pagesTravel-Related Respiratory Symptoms and InfectionStavia BluntNo ratings yet
- 1 s2.0 S2049080121000595 Main1Document6 pages1 s2.0 S2049080121000595 Main1Devina ArrandhikasariNo ratings yet
- Assessing Preventive Health Behaviors From COVID-1Document19 pagesAssessing Preventive Health Behaviors From COVID-1Nur Melizza, S.Kep., NsNo ratings yet
- Yezli S, Yassin Y, Mushi A Et Al. Knowledge, Attitude and Practice (KAP) Survey Regarding Antibiotic Use Among HAJJDocument7 pagesYezli S, Yassin Y, Mushi A Et Al. Knowledge, Attitude and Practice (KAP) Survey Regarding Antibiotic Use Among HAJJnadiahumaira2019No ratings yet
- 2015 - Health-Promoting Lifestyle Behaviors Among NursesDocument6 pages2015 - Health-Promoting Lifestyle Behaviors Among NursesSubhan AnsariNo ratings yet
- Pi Is 0099176720304220Document10 pagesPi Is 0099176720304220yasintameganabilaNo ratings yet
- Final Research Paper (Aniket Neemkar)Document11 pagesFinal Research Paper (Aniket Neemkar)niyutns3005No ratings yet
- The Association of Smell and Taste Dysfunction With COVID19, and Their Functional ImpactsDocument6 pagesThe Association of Smell and Taste Dysfunction With COVID19, and Their Functional ImpactsKhaled DabourNo ratings yet
- 1 s2.0 S2405457721000358 MainDocument6 pages1 s2.0 S2405457721000358 MainYosephine SantosoNo ratings yet
- International Journal of Surgery OpenDocument6 pagesInternational Journal of Surgery Openeman mamdohNo ratings yet
- Proposed Protocol For Improving Staff Nurses' Awareness and Self - Efficacy With Novel Coronavirus SARS Cov 2 OutbreakDocument8 pagesProposed Protocol For Improving Staff Nurses' Awareness and Self - Efficacy With Novel Coronavirus SARS Cov 2 OutbreakEditor IJTSRDNo ratings yet
- 1 s2.0 S0264410X1930163X MainDocument7 pages1 s2.0 S0264410X1930163X Mainzezo.3kxNo ratings yet
- Travel Medicine and Infectious DiseaseDocument7 pagesTravel Medicine and Infectious DiseaseGhadah AlyousifNo ratings yet
- Pi Is 0003999321003269Document12 pagesPi Is 0003999321003269Amanda SchaefferNo ratings yet
- COVID - Risk of Hospitaization IF-1.6Document20 pagesCOVID - Risk of Hospitaization IF-1.6Manal Haj HamadNo ratings yet
- National Health ProgramDocument7 pagesNational Health ProgramJyoti singhNo ratings yet
- COVID-19 Viral Sepsis: Impact on Disparities, Disability, and Health OutcomesFrom EverandCOVID-19 Viral Sepsis: Impact on Disparities, Disability, and Health OutcomesUzma SyedNo ratings yet
- JEM Guideline For Writers 2023Document4 pagesJEM Guideline For Writers 2023nuvitaNo ratings yet
- Outcome Research, Nutrition, and Reverse Epidemiology in Maintenance Dialysis PatientsDocument9 pagesOutcome Research, Nutrition, and Reverse Epidemiology in Maintenance Dialysis PatientsnuvitaNo ratings yet
- Study Comparatif Kualitas Hidup Antara Pasien Hemodialisis Dengan Pasien Continuous Ambulatory Peritoneal DialysisDocument6 pagesStudy Comparatif Kualitas Hidup Antara Pasien Hemodialisis Dengan Pasien Continuous Ambulatory Peritoneal DialysisnuvitaNo ratings yet
- Prevalence of Chronic Kidney Disease in Patients With or at A High Risk of Cardiovascular DiseaseDocument4 pagesPrevalence of Chronic Kidney Disease in Patients With or at A High Risk of Cardiovascular DiseasenuvitaNo ratings yet
- Evaluation of Protein-Energy Wasting and Inflammation On Patients Undergoing Continuous Ambulatory Peritoneal Dialysis and Its CorrelationsDocument8 pagesEvaluation of Protein-Energy Wasting and Inflammation On Patients Undergoing Continuous Ambulatory Peritoneal Dialysis and Its CorrelationsnuvitaNo ratings yet
- Clinical Practice Guideline Undernutrition in Chronic Kidney DiseaseDocument27 pagesClinical Practice Guideline Undernutrition in Chronic Kidney DiseasenuvitaNo ratings yet
- Enteric Fever (Typhoid and Paratyphoid) in Adult Treatment Guidelines (UHL)Document3 pagesEnteric Fever (Typhoid and Paratyphoid) in Adult Treatment Guidelines (UHL)fildzah amalyaNo ratings yet
- STS100 - That SugarDocument3 pagesSTS100 - That Sugarbjornebol01No ratings yet
- Complications of Intravenous TherapyDocument29 pagesComplications of Intravenous TherapyKrizia BonillaNo ratings yet
- Care For Your Heart While You SleepDocument6 pagesCare For Your Heart While You SleepkrishnaNo ratings yet
- Carpal Tunnel SyndromeDocument43 pagesCarpal Tunnel SyndromePra YudhaNo ratings yet
- Alison Cooper QuestionDocument3 pagesAlison Cooper QuestionSathiyaseelan Velayutham89% (18)
- More Simply Human - On The Universality of Madness (Nancy McWilliams)Document11 pagesMore Simply Human - On The Universality of Madness (Nancy McWilliams)Anastasiya PlohihNo ratings yet
- Report Writing ProjectDocument14 pagesReport Writing ProjectAan JuttNo ratings yet
- Nursing Care Plan (Pedia)Document5 pagesNursing Care Plan (Pedia)JA BerzabalNo ratings yet
- Food PoisoningDocument20 pagesFood PoisoningNgọcNo ratings yet
- NCMB312 RLE-Burn Injuries-Group 3Document56 pagesNCMB312 RLE-Burn Injuries-Group 3Maica LectanaNo ratings yet
- Biology ProjectDocument23 pagesBiology ProjectSahil AhmadNo ratings yet
- Alves Celina, Ra Early DetectionDocument124 pagesAlves Celina, Ra Early DetectionAmela SelimicNo ratings yet
- Children Part I Continuation TABLEDocument5 pagesChildren Part I Continuation TABLEMaikka IlaganNo ratings yet
- Dr. Rosario R. Trifiletti M.D. PH.D.: Date of Preparation May 1, 2010 Personal DataDocument15 pagesDr. Rosario R. Trifiletti M.D. PH.D.: Date of Preparation May 1, 2010 Personal Dataapi-28616529No ratings yet
- Pathophysiology AKI in Covid ACKD JournalDocument30 pagesPathophysiology AKI in Covid ACKD JournalChucksters79No ratings yet
- Edema: Ahammed Naseem Roll No: 3 Second Year BSC Nursing Al-Mas College of NursingDocument24 pagesEdema: Ahammed Naseem Roll No: 3 Second Year BSC Nursing Al-Mas College of NursingNaseem Bin YoosafNo ratings yet
- Notes From Beynon LectureDocument6 pagesNotes From Beynon LecturearianNo ratings yet
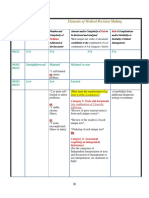
- 3-Level of MDMDocument3 pages3-Level of MDMmedical codingNo ratings yet
- I Summary Family MedicineDocument185 pagesI Summary Family MedicineModa ModyNo ratings yet
- Heart Failure - ReferatDocument10 pagesHeart Failure - ReferatAlbert ShantoNo ratings yet
- 2018 - Dr. Mahatma - Syndrome MetabolikDocument79 pages2018 - Dr. Mahatma - Syndrome MetabolikDEWI MULYANINo ratings yet
- WCPD 2016 CP Diagnosis Treatment Infographic WORLDDocument1 pageWCPD 2016 CP Diagnosis Treatment Infographic WORLDvinicius_vrrNo ratings yet