You might also like
- Endodonticsurgery - FinalDocument70 pagesEndodonticsurgery - FinalSurya Jayaprakash100% (1)
- School Nurse SlidesDocument13 pagesSchool Nurse Slideseirnkath100% (2)
- Single Visit Endodontic TherapyDocument95 pagesSingle Visit Endodontic TherapyAshish Bhadane100% (2)
- Diseases of Periradicular TissuesDocument122 pagesDiseases of Periradicular TissuesAnas Kallayil100% (4)
- Criteria For The Ideal Treatment Option For Failed Tics Surgical or NonsurgicalDocument8 pagesCriteria For The Ideal Treatment Option For Failed Tics Surgical or NonsurgicalPaRpArOsSaNo ratings yet
- Modern Hospital EquipmentsDocument4 pagesModern Hospital EquipmentsjohnnydflipNo ratings yet
- Fundamentals of Nursing Transes 3Document4 pagesFundamentals of Nursing Transes 3Louise TorresNo ratings yet
- Oral Medicine & Pathology from A-ZFrom EverandOral Medicine & Pathology from A-ZRating: 5 out of 5 stars5/5 (9)
- Endodontics Final ReviewerDocument16 pagesEndodontics Final ReviewerMehdi Moshaveri100% (3)
- Clinical Management of Endodontic CasesDocument91 pagesClinical Management of Endodontic CasesSharlene OngNo ratings yet
- Treating Periapical Granuloma with Root Canal TherapyDocument3 pagesTreating Periapical Granuloma with Root Canal TherapyLina BurduhNo ratings yet
- Endodontics Final ReviewerDocument27 pagesEndodontics Final ReviewerRosette Go100% (5)
- Acute Liver FailureDocument13 pagesAcute Liver FailureDiana YvetteNo ratings yet
- Management of Open ApexDocument28 pagesManagement of Open Apexdiksha sinha100% (4)
- Endodontic SurgeryDocument8 pagesEndodontic SurgeryjoseNo ratings yet
- External Cervical Resorption JC FinalDocument46 pagesExternal Cervical Resorption JC FinalKomal JadhavNo ratings yet
- UNIT4 Endodontics - Best PPDocument37 pagesUNIT4 Endodontics - Best PPAnna PruteanuNo ratings yet
- Retreatment in Persistent Apical PeriodontitisDocument169 pagesRetreatment in Persistent Apical PeriodontitisAnciya NazarNo ratings yet
- Lecture - 6-6 - Acute Apical Periodontitis Diagnosis Clinical Manifestations TreatmentDocument57 pagesLecture - 6-6 - Acute Apical Periodontitis Diagnosis Clinical Manifestations TreatmentA.J. YounesNo ratings yet
- Presented by DR Ekta Garg Mds 1 Year Department of Conservative Dentistry & EndodonticsDocument107 pagesPresented by DR Ekta Garg Mds 1 Year Department of Conservative Dentistry & Endodonticsjibin kareemNo ratings yet
- Basics of Root Canal TreatmentDocument117 pagesBasics of Root Canal TreatmentSameer VinchurkarNo ratings yet
- Lecture - 6-8 - Preparation of The Root Canal. Stages of The Endodontic TreatmentDocument45 pagesLecture - 6-8 - Preparation of The Root Canal. Stages of The Endodontic TreatmentA.J. YounesNo ratings yet
- Endodontic FailuresDocument38 pagesEndodontic FailuresSonam RawatNo ratings yet
- Ob Turati OnDocument84 pagesOb Turati Onwu yuoNo ratings yet
- Pedo - Trauma 3Document27 pagesPedo - Trauma 3Florida ManNo ratings yet
- Principles of Endodontics II: RetreatmentDocument31 pagesPrinciples of Endodontics II: RetreatmentroorayNo ratings yet
- Restoration of RCTed Teeth - Part 1 PDFDocument16 pagesRestoration of RCTed Teeth - Part 1 PDFAshwaq A Bani AtaNo ratings yet
- Sodium Hypochlorite: by DR - Anoop.V.Nair PG, Dept of Cons Dentistry & EndodonticsDocument72 pagesSodium Hypochlorite: by DR - Anoop.V.Nair PG, Dept of Cons Dentistry & Endodonticshasanu88No ratings yet
- Repair of Teeth With Cracks in CrownsDocument52 pagesRepair of Teeth With Cracks in CrownsSandeep PksNo ratings yet
- 13.endodontic Treatment FR YounPermanent TeethDocument31 pages13.endodontic Treatment FR YounPermanent TeethKhan MustafaNo ratings yet
- Endodontics: Oral Surgery Oral Medicine Oral PathologyDocument7 pagesEndodontics: Oral Surgery Oral Medicine Oral PathologyUntuk TugasNo ratings yet
- Etiology and Classification of Periapical Tissue DiseasesDocument5 pagesEtiology and Classification of Periapical Tissue DiseasesPrince AmiryNo ratings yet
- Endodontic RetreatmentDocument59 pagesEndodontic RetreatmentOmar MustafaNo ratings yet
- Calcium Hydroxide Induced Healing of Periapical RaDocument4 pagesCalcium Hydroxide Induced Healing of Periapical RaMaría José VanegasNo ratings yet
- Apiko 1Document5 pagesApiko 1Asri DamayantiNo ratings yet
- Pulp Therapy For Young Permanent TeethDocument35 pagesPulp Therapy For Young Permanent Teethpayeldeb51997No ratings yet
- Causes of RCT FailureDocument19 pagesCauses of RCT Failureحمأد ہادیNo ratings yet
- Sodium HypochloriteDocument19 pagesSodium HypochloriteSayak GuptaNo ratings yet
- Ricucci 2014Document7 pagesRicucci 2014leiliromualdoNo ratings yet
- Intra Canal Medication PDFDocument34 pagesIntra Canal Medication PDFKhalil El HalimyNo ratings yet
- Retrograde PreparationDocument16 pagesRetrograde Preparationwhussien7376100% (1)
- Endodontic Clinical Manual: RES 542 (Endo For Semester 10)Document35 pagesEndodontic Clinical Manual: RES 542 (Endo For Semester 10)Mustafa SaßerNo ratings yet
- Rajas Dental College Seminar on Abscess of the PeriodontiumDocument19 pagesRajas Dental College Seminar on Abscess of the PeriodontiumSharonNo ratings yet
- 14 Endodontic Surgery-seminarDocument39 pages14 Endodontic Surgery-seminarRiya JainNo ratings yet
- Errors in Root Canal PreparationDocument9 pagesErrors in Root Canal PreparationPhúc Hồ Văn TâmNo ratings yet
- L3. Apexogenesis - ApexificationDocument44 pagesL3. Apexogenesis - ApexificationAGENG RAHMA HIJAHANIS ILMASTITI 1No ratings yet
- Int Endodontic J - 2006 - Nair - On The Causes of Persistent Apical Periodontitis A ReviewDocument33 pagesInt Endodontic J - 2006 - Nair - On The Causes of Persistent Apical Periodontitis A ReviewJairo AndrésNo ratings yet
- Garcia 2010Document6 pagesGarcia 2010VivianColoradoGomezNo ratings yet
- Aquatine Endodontic Cleanser Effectiveness Against Smear LayerDocument6 pagesAquatine Endodontic Cleanser Effectiveness Against Smear Layeraulia lubisNo ratings yet
- Kuliah Endodontik Pada AnakDocument41 pagesKuliah Endodontik Pada AnakAbiyyu WidyaNo ratings yet
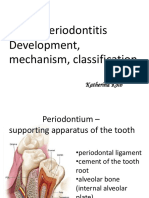
- Lecture - 6-5 - Apical Periodontitis. The Development Mechanism, ClassificationDocument27 pagesLecture - 6-5 - Apical Periodontitis. The Development Mechanism, ClassificationA.J. YounesNo ratings yet
- Apexogenesis of A Symptomatic MolarDocument5 pagesApexogenesis of A Symptomatic MolarFoysal SirazeeNo ratings yet
- Coronal Microleakage of Restorative MaterialsDocument9 pagesCoronal Microleakage of Restorative Materialsjhon HanselNo ratings yet
- OOOO Ricucci 2000Document6 pagesOOOO Ricucci 2000karlaNo ratings yet
- Pediatric Pulp Therapy Materials EvaluationDocument49 pagesPediatric Pulp Therapy Materials EvaluationAnonymous 2h5lIeNo ratings yet
- Apexification: A comprehensive review of inducing root apex closureDocument5 pagesApexification: A comprehensive review of inducing root apex closurefatimahNo ratings yet
- AR Histobacteriologic ConditionsDocument9 pagesAR Histobacteriologic ConditionsCARLA PATRICIA JORDAN SALAZARNo ratings yet
- Intracanal MedicationDocument34 pagesIntracanal MedicationdentistdentistdentisNo ratings yet
- Periodontal AbscessDocument40 pagesPeriodontal AbscessDrDebasish Mishra100% (1)
- Traditional and Contemporary Techniques For Optimizing Root Canal IrrigationDocument9 pagesTraditional and Contemporary Techniques For Optimizing Root Canal IrrigationrintanfsNo ratings yet
- Treatment of Chronic Apical Periodontitis. Principles. Indications and ContraindicationsDocument24 pagesTreatment of Chronic Apical Periodontitis. Principles. Indications and ContraindicationsShany SchwarzwaldNo ratings yet
- Maxillarysinus 170705134531 PDFDocument93 pagesMaxillarysinus 170705134531 PDFmelaniaNo ratings yet
- Article 1677562130Document4 pagesArticle 1677562130mariaiugaespadaNo ratings yet
- 7.1 Pasmeth, Pamet, Laws, Specimen Collection And: Handling, Clinical MicrosDocument24 pages7.1 Pasmeth, Pamet, Laws, Specimen Collection And: Handling, Clinical MicrosMarcoNo ratings yet
- Auditory Brainstem Response (ABR) Testing: How Is The Test Done?Document3 pagesAuditory Brainstem Response (ABR) Testing: How Is The Test Done?John Paul PrestonNo ratings yet
- Remote Health Atlas Resuscitation Trolley: 1. General InformationDocument3 pagesRemote Health Atlas Resuscitation Trolley: 1. General InformationSusanti ShantyNo ratings yet
- Speech Recognition in Noise Test (Sprint) For H-3 ProfileDocument8 pagesSpeech Recognition in Noise Test (Sprint) For H-3 ProfileshivfifaNo ratings yet
- Mariano Marcos Memorial Hospital & MC, Batac, Ilocos Norte Batac, Ilocos NorteDocument10 pagesMariano Marcos Memorial Hospital & MC, Batac, Ilocos Norte Batac, Ilocos NorteglairievyNo ratings yet
- DR Ward ClassDocument36 pagesDR Ward ClassChristy Mutia AlumbroNo ratings yet
- Critical Care Nursing BurnoutDocument7 pagesCritical Care Nursing Burnoutcallyope4No ratings yet
- 3rd Lesson Assessing Child Bearing WomenDocument6 pages3rd Lesson Assessing Child Bearing WomendaningdubouzetNo ratings yet
- JHS Students' Knowledge of Healthy Food and Their Actual Eating HabitsDocument78 pagesJHS Students' Knowledge of Healthy Food and Their Actual Eating HabitsDessirea FurigayNo ratings yet
- Side-Effects Quinolone Antibiotics Toxicity. July 2005QUINOLONE ANTIBIOTICS TOXICITY. July 2005Document82 pagesSide-Effects Quinolone Antibiotics Toxicity. July 2005QUINOLONE ANTIBIOTICS TOXICITY. July 2005Avelox FloxNo ratings yet
- BMS291 Practice ExamDocument26 pagesBMS291 Practice Examsopheeyuh100% (1)
- CV Tudorache Andrei ActualizatDocument3 pagesCV Tudorache Andrei ActualizatAndrei TudoracheNo ratings yet
- CephalgiaDocument24 pagesCephalgiaNurlita Ranti YulistyaNo ratings yet
- COVID Origin and Global SpreadDocument12 pagesCOVID Origin and Global SpreadChaitanya BhardwajNo ratings yet
- Review of Influenza as a Seasonal and Pandemic DiseaseDocument12 pagesReview of Influenza as a Seasonal and Pandemic DiseaseFreddy SueroNo ratings yet
- Clinical Trial Protocol Iranian Registry of Clinical TrialsDocument10 pagesClinical Trial Protocol Iranian Registry of Clinical TrialsAnupNo ratings yet
- CBT TestQ5Document3 pagesCBT TestQ5Roxane de Jesus100% (1)
- Food Deterioration and Its CausesDocument10 pagesFood Deterioration and Its CausesM ZAHID SADIQNo ratings yet
- CCA206 - Assessment - 2 - Brief - Case Study Analysis and Developing A Care Plan - Module 4.2 - AO - 13102021Document11 pagesCCA206 - Assessment - 2 - Brief - Case Study Analysis and Developing A Care Plan - Module 4.2 - AO - 13102021Akriti DangolNo ratings yet
- Mental Health Among Generation Z.Document3 pagesMental Health Among Generation Z.kevine atienoNo ratings yet
- Medical Technology Education, Career Opportunities and Licensure ExaminationsDocument49 pagesMedical Technology Education, Career Opportunities and Licensure Examinationsfrancis dimakilingNo ratings yet
- IdiPAZ 2017 - Instituto de Investigación, Hospital Universitario La Paz - MadridDocument167 pagesIdiPAZ 2017 - Instituto de Investigación, Hospital Universitario La Paz - MadridMagdalena Alejandra PIERA50% (2)
- Managing Abnormal Uterine BleedingDocument6 pagesManaging Abnormal Uterine Bleedingyousef ibrahimNo ratings yet
- Daftar Pustaka Fix GbsDocument2 pagesDaftar Pustaka Fix GbsElizabeth IvanaNo ratings yet
- Blom 2012, The Effect of Mouthrinses On Oral Malodor: A Systematic ReviewDocument14 pagesBlom 2012, The Effect of Mouthrinses On Oral Malodor: A Systematic ReviewPhuong ThaoNo ratings yet
- Pearl Zanker School: Shangrila Mia-Ramzan, Principal Recep Iscan, Assistant PrincipalDocument4 pagesPearl Zanker School: Shangrila Mia-Ramzan, Principal Recep Iscan, Assistant PrincipalsirishaNo ratings yet