Advances in Plastic & Reconstructive Surgery
© All rights are reserved by Dr. Marcos Quispe Jorge Luis, et al.
Research Article ISSN: 2572-6684
Semi-open Rhinoplasty: Getting together the best of both, Open and
Closed Rhinoplasty
Marcos Quispe Jorge Luis1, Marcos Quispe Mirek Fernando2, Marcos Quispe Henri Armando1, Benavides Rubio
Jacqueline1
1Plastic Surgery, Vitalis Clinic.
2Facial Plastic Surgery, Vitalis Clinic.
Abstract
Summary: Rhinoplasty is one of the most common procedures of our surgical practice. According to the approach, it can be open or
closed; however, the semi-open approach has been recently incorporated. Semi-open rhinoplasty allows the dissection and complete
exposure of the alar cartilage, similar to the open approach, but the incision is limited to the nasal vestibule without a transcolumellar
scar, just as in the closed approach.
The objective of this work is to describe the surgical technique and show the outcomes.
Material and Methods: We evaluated 376 patients who underwent primary and secondary rhinoplasty with the semi-open technique,
performed between June 2016 and June 2019.
Results: In this period, we performed 376 rhinoplasties with the semi-open technique; 340 (90.4%) patients underwent primary rhino-
plasty and 36, secondary; most of our patients were women (73.1%), both, in primary (72.4%), as in secondary rhinoplasty (80.6%). To
address the nasal tip, we performed mainly domal suture and columellar graft in 48.9% of the patients, followed by domal suture,
columellar graft, and nasal tip graft in 30.3%, and in 20.8%, we shaped the tip with domal sutures.
Conclusion: The semi-open technique provides a wide exposition of the nose, to successfully address and modify the osteocartilaginous
nasal structure, especially the nasal tip, thus obtaining predictable results.
Keywords: Rhinoplasty; Semi-open rhinoplasty; Primary Rhinoplasty; Septorhinoplasty.
Introduction and length of the incision in the columellar skin. Also, Sevin et al. [4],
Bruschi et al. [5], Cardenas et al. [6], Kamburoglu et al. [7] published
Rhinoplasty is one of the most common procedures of our surgical successful results with the technique described. The term semi-open
practice. According to the approach, it can be open or closed. The rhinoplasty was introduced by Inchingolo et al. [8] in 2012, who
open rhinoplasty provides a wide exposure of the nasal structures, to reported some cases he operated on, using the technique published by
clearly identify defects, and correct them under direct vision. However,
Guerrerosantos.
the transcolumellar scar can alter the final aesthetic results, especially
in non-caucasian patients. On the other hand, the closed rhinoplasty In 2014 we began performing this approach for the primary
limits the incision only to the nasal vestibule without a visible scar. treatment of the nasal tip, instead of the “delivery" technique; soon it
Thus, this narrow exposure of the osteocartilaginous vault, makes became our first surgical option for both, primary and secondary
difficult the handling of the structures, especially those of the nasal rhinoplasty, choosing the closed one with intracartilaginous incision for
tip. some select primary cases, and the open for particular secondaries. The
objective of this work is to present the surgical technique and show our
Semi-open rhinoplasty technique allows wide exposure of the alar
results.
cartilage, as in open technique, with the incision placed in the nasal
vestibule with no transcolumelar scar. This technique, previously Material and Methods
known with another nomination, was published in 1990 by Dr. Gue-
We evaluated 376 Patients who underwent primary and seco-
rrerosantos [1], as a technique of "Open rhinoplasty without skin-
ndary rhinoplasties, with the semi-open approach, from June 2016 to
columella incision," later Holmstron in 1996 [2], and Bravo & Schwarze
June 2019, patients having only closed or open rhinoplasty were
in 2008 [3] published a similar technique with a slight variation in shape
excluded. The database was checked to obtain the list of patients
operated on with the technique described and collected their medical
records and the photographic album.
*Address for Correspondence: Dr. Marcos Quispe Jorge, Plastic Surgeon, Surgical Technique
Manuel Olguín Street N° 970 – 19, Santiago de Surco, Lima, Perú. Postal
Address: 15023, E-mail: jmarcosq@icloud.com drjorgemarcos@gmail.com With the Patient under intravenous sedation, we block, the infra
and supraorbital nerves with lidocaine and epinephrine1/200000 with
Received: April 24, 2020; Date Accepted: May 29, 2020, Date published:
June 01, 2020. local troncular anesthesia, we continue the tumescent infiltration into
Adv Plast Reconstr Surg, 2020 Page 327 of 330
Marcos Quispe JL, Marcos Quispe MF, Marcos Quispe HA, Benavides Rubio J. Semi-open rhinoplasty: Getting together the best of both, open and closed
rhinoplasty. Adv Plast Reconstr Surg, 2020; 4(2): 327-330.
the submucosal plane of the nasal vault, and xxx the subcutaneously the
nasal tip and base. We wait for the anesthesia effect for 10 minutes
and proceed with the infracartilaginous incision 1 mm from the lower
margin of the alar cartilage: from medial to lateral in the lateral crus,
from top to bottom at the edge of the medial crus along the columella,
and the incision is completed at the level of the domes, carefully to
avoid injuring the area of the soft triangle [Figure 1].
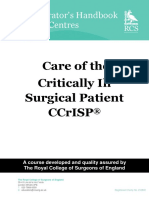
Figure 3: The semi-open technique shows up widely the alar cartilage; to trim
and reshape the nasal tip by placing sutures: ix Interdomal, transdomal,
intercrural, septocolumellar. (left) If needed, we caninterdomal
use a columellar graft; it is
placed between the medial crurato provide support and projection to the nasal
crura to
tip (right).
Figure 1: Semi-open rhinoplasty showing infracartilaginous incision (left). Local
anesthesia with IV sedation, tumescent infiltration of lidocaine with epine-
phrine 1/200000. The procedure with minimal bleeding (right).
With fine-tipped scissors, we dissect the alar cartilage; from the
incision, heading superiorly on the supracartilaginous plane to free
the nasal cartilages from the nasal skin. Then, to perform this step, we
put a traction stitch with non-absorbing 2/0 suture, placed symmetri-
cally at the height of the domes to pull the alar cartilage downwards,
and easily dissect the upper half of the nose [Figure 2]. We proceed to
dissect the alar cartilage, upper lateral cartilage, the caudal edge of the Figure 4: The semiopen approach allows grafting the tip with a shield to
septum, when this is done, we put the Aufritch retractor to visualize improve definition, and dome asymmetry (left). We can place mixed grafts
the osteocartilaginous structure completely, determine the amount of (right), gull wings grafts, transpose lateral crura cephalad, reinforce lateral
resection and proceed using a chisel or scalpel. crura with fixed or articulated laminar graft, and many other options.
Results
In the period studied, 376 rhinoplasties were performed with the
semi-open technique: 340 (90.4%) were primary rhinoplasties and 36
cases secondary, the majority of them in women (73.1%); both:
primary rhinoplasty (72.4%), as secondary (80.6%), as referred in
[Table 1]. To address the nasal tip, we performed mainly domal
sutures and cartilaginous graft (columellar and or nasal tip) in 79.2%
of all our patients. Only in some of them 20.8% we used exclusively
domal sutures.
Table 1:Demographic features and nasal tip procedures performing semi-
Figure 2: To facilitate dissection and handling, we link the domes with black open rhinoplasty. when performing
silk 2/0, to pull them to correct osteocartilaginous defects (Left). Thus, we
Primary Secondary
laterally retract the alar cartilage, and with the double hook, we expose the Rhinoplasty Rhinoplasty
cartilaginous back to inset spreader grafts (right). Total
posterior aspect of the cartilage,and insert spreader grafts Men Women Men Women
Next, we check and do the corrections needed, trim the dorsum,
Cases 94 246 7 29 376
and go back to the nasal tip; according to the surgical plan, we first
place spreader grafts [Figure 2], go on with the resection of the cephalic Age 17 - 52 y 15-53 y 23-62 y 21-57 y
edges of the lateral crus, then we put transdomal sutures with 5/0
prolene, remove the traction stitch from the domes. We evaluate the
Domal Suture 23 51 0 4 78
shape and projection of the domes in their natural position; then we
transfer the markings to the other nostril. In that position, we put a
Domal Suture + 57 117 2 8 184
columellar graft [Figure 3] or a septal extension graft, according to Columellar strut
the individual nose evaluation, it is fixated with stitches. Then, we
Domal Suture + 14 78 5 17 114
proceed with intradomal, transdomal, and or interdomal suture Columellar strut +
[Figure 4], and at the end of this step, xxxxxx
we put nasal tip grafts if needed Nasal Tip Graft
place
[Figure 4]. Finally, we perform internal and or external osteotomy
using 2mm chisel, suture the nasal mucosa with chromic catgut 4/0,
and xxx
we end with splinting.
Adv Plast Reconstr Surg, 2020 Page 328 of 330
Marcos Quispe JL, Marcos Quispe MF, Marcos Quispe HA, Benavides Rubio J. Semi-open rhinoplasty: Getting together the best of both, open and closed
rhinoplasty. Adv Plast Reconstr Surg, 2020; 4(2): 327-330.
Above all the patients, 340 underwent primary rhinoplasty, which
represents 90.4%. Note that it was more frequent in women (72.4%).
In this group, the average age was 25.2 years in women and slightly
superior in men (26.1y). The procedures required for reshaping the
nasal tip in all patients were the inset of domal sutures: interdomal,
transdomal, intercrural, and or septocolumellar; and in 78.2% we
insert a cartilaginous graft: in the columella (51.1%) and the nasal tip
(27.0%). Note that 78 patients (21.8%) required only domal sutures.
Secondary rhinoplasties represented 9.6% of total cases, with more
frequency in women (80.6%), and the average age, in both sexes, is
higher than those of primary rhinoplasties. Concerning the treatment
of nasal tip, the domal sutures were used in all patients, associated
with cartilaginous grafting in 88.9% of these cases: in the columella
(27.8%) and de nasal tip (61.1%). Note that the nose tip grafting was
the most frequent procedures used both, in women (58.6%) and men
(71.4%), as shown in [Table 1]. Also, only 11.1% of these cases
required only domal sutures.
Figure 6: Male patient, 26 years old. Primary septorhinoplasty was performed
with semi-open technique: resection of the osteocartilaginous hump, the
resection of the
cephalic edge of the lateral cruraxxxxxxxx
resection, correction of the prominent nasal
spine. Also, septoplasty was performed to correct the septal deviation and
obtain cartilage necessary to perform spreader graft and columellar strut. The
enough
handling of thecartilage
nasal tip was completed with transdomal and interdomal
sutures. Results at six months postoperative: the frontal view shows
correction of the asymmetry in the cartilaginous back and nasal tip (Figure
A); the lateral visa shows an aesthetic back, with adequate rotation and
view
projection of the nasal tip, proper nasolabial angle, and elongation of the
upper lip (Figure B); all reflected too in the oblique view (Figure C).
Figure 5: Female patient, 42 years old. Primary semi-open rhinoplasty: resection
of a dorsal hump, upper border resection of the lateral crura, and caudal edge
of the septum. The nasal tip was reshaped with sutures: projection septocolu-
mellar, intercrural, transdomal, and interdomal. Results at two months
showing shortening of the nose in front view (Figure A), Side (Figure B) and
oblique (Figure C). the
Discussions
xx Discussion
The selection of the best surgical technique in rhinoplasty is
permanently one x discussion because the results depend on factors
concerning both, patient and surgeon. [9]. However, it is possible to Figure 7: Female patient, 34 years old. High dorsal hump, hanging tip, acute
achieve excellent results with open or closed rhinoplasty. Although, nasolabial angle, short columella, and slight alar retraction. Primary rhinoplasty
many authors consider that open rhinoplasty has many advantages for was performed with infracartilaginous incision, xxxx with subperichondrial and
the treatment of patients with delicate nasal tips, the full exposure of subperiosteal dissection of the back, resection of the osteocartilaginous hump,
the cartilages and its correction under direct vision, it is necessary to the cephalic edge of the lateral crura and the caudal edge of the nasal septum.
Septoplasty to harvest cartilage for spreader graft, columellar strut. The
make an incision through the columella that leaves a visible scar.
management of the nasal tip was completed with transdomal and interdomal
The semi-open rhinoplasty technique, in our concern, is an sutures, sheens and pecks graft, finally we did alar contour graft. Postoperative
excellent surgical option because it gets together the best of both results after six months, front view (Figure A), side view (Figure B), and
"classic" techniques: open and closed. Thus, it allows us to deliver the inferior view (Figure C). Sheen and Peck grafts
alar cartilage similar to the open technique, but with only a single scar The infracartilaginous incision used in this technique, allows
limited to the nasal vestibule, just as in the closed approach, avoiding adequate exposure of the alar cartilage through the nostrils, their
the disruption of the columella. Although the term semi-open features are completely visible, and precise surgical corrections are
rhinoplasty was introduced by Inchingolo et in 2012 [8], who operated proposed, using sutures and graft techniques. If greater exposure is
few cases of rhinoplasty using the surgical technique, it was published necessary, this original incision can be extended to the base of the
by Guerrerosantos [1] in 1990 and named "semiopen rhinoplasty." columella, as referred by Holstrom [2] and Kamburologlu [7], and
Adv Plast Reconstr Surg, 2020 Page 329 of 330
Marcos Quispe JL, Marcos Quispe MF, Marcos Quispe HA, Benavides Rubio J. Semi-open rhinoplasty: Getting together the best of both, open and closed
rhinoplasty. Adv Plast Reconstr Surg, 2020; 4(2): 327-330.
even extend it to the upper lip, as proposed by Bravo & Shcwaze [3]. • Authors' contributions: All authors have contributed to this work.
However, we believe that it is not necessary to make such extensive
incisions, except in patients with small or constricted nostrils. In • Ethics approval and consent to participate: Not applicable.
addition, as this incision goes through the inferior aspect of the • Consent for publication: Not applicable.
nostril, we can address the deformities of the lower area of the medial
crura, simultaneously with the dome and lateral crura [1]. On the • Competing interests: We have not conflicts of interest.
other hand, the incision and dissection must be carefully executed so
as not to damage the soft triangle [10], nor tear the mucosa or References
cartilage, especially at the level of the domes or medial crura.
1. Guerrerosantos J. Open rhinoplasty without skin-columella incision. Plast. Reconstr.
As referred by Guerrerosantos [1], Bravo & Schware [3] and Surg. 85:955-�960, 1990. [Crossref]
Brushi et al. [5], we use this technique in primary and secondary 2. Holmstrom H, Luzi F. Open Rhinoplasty without transcolumellar incision. Plast
rhinoplasties, that requires handling of back and nasal tip; and, we Reconstr Surg. 97: 321-326,1996. [Crossref]
prefer the open technique in secondary rhinoplasties with significant 3. Bravo FG, Schwarze HP. Closed-Open rhinoplasty with extended lip dissection: A
new concept and classification of rhinoplasty. Plast Reconstr Surg.122: 944-950,
deformity and for the treatment of cleft nose. However, Sevin et al. [4]
2008. [Crossref]
and Holstrom [2] have also used it in cases of nasal crush. Likewise,
4. Sevin A, Sevin K, Erdogan B, Deren O, Adanali G. Open Rhinoplasty Without
just as Kamburoglu et al. [7] and Holstrom [2], we have operated on Transcolumellar Incision. Ann Plast Surg. 2006;57. 252-254. [Crossref]
patients who require additional procedures such as septoplasty and
5. Bruschi S, Bocchiotti MA, Verga M, Kefalas N, Fraccalvieri M. Closed Rhinoplasty
turbinectomy, in such patients, we prefer to perform septoplasty by with Marginal Incision: Our Experience and Results. Aesth. Plast. Surg. 30:155�-
septocolumellar incision separated from the columellar incision. 158, 2006. [Crossref]
6. Cardenas-Camarena L, Guerrero MT: Improving nasal tip projection and definition
We agree with the findings described by Zeid et al. [11] who using interdomal sutures and open approach without transcolumellar incision. Aesth
conducted a comparative study of closed rhinoplasty vs. semiopen Plast Surg 26:161�-166, 2002. [Crossref]
rhinoplasty. This work confirms that the semi-open technique offers 7. Kamburog l̆ u HO, Kayıkc ̧ıog ̆lu AU. Closed Rhinoplasty with Open Approach
greater accessibility to the osteocartilaginous framework. However, it Advantages: Extended Intranasal Incisions and Tip Rearrangement Sutures. Aesth
is a fact that the extended operative time increase edema in the Plast Surg (2014) 38:653–661. [Crossref]
immediate and late postoperative findings not only observed in our 8. Inchingolo et al.: Semi-open rhinoplasty: a new Maxillofacial technique. Head &
cases but mentioned by Dr. Guerrerosantos [1] in his original article, Face Medicine, 2012, 8:13. [Crossref]
this edema lasts approximately six months. It is mainly observed in 9. Tebbetts JB. Open and Closed Rhinoplasty (Minus the “Versus”): Analyzing
Processes. Aesthetic Surg J. 2006;26:456–459. [Crossref]
thick and mestizo skin. Another disadvantage of this technique is, that
it requires an extended learning curve, to avoid misplacing the 10. Campbell CF, Pezeshk RA, Basci DS, Scheuer JF, Sieber DA, Rohrich RJ.
Preventing Soft-Tissue Triangle Collapse in Modern Rhinoplasty. Plast. Reconstr.
incision and careful dissection of the flaps to prevent damaging the Surg. 140: 33e, 2017. [Crossref]
alar cartilage or the soft triangle [10] Holstrom [2]. Also, we must 11. Zeid NG, El Fouly MS, Kamel A, Wahba BM, Behman RN, Elmottaleb Sabaa MA.
consider that potential damage such as necrosis of the mucosa could Rhinoplasty approaches, closed versus semiopen: a comparative study. Pan Arab J
occur by superficial dissection, tight taping, infection or hematoma; Rhinol. 2016, 06:39-44. [Crossref]
also, in cases of significant reductions of the nasal tip, the redundant 12. Rui Xavier. Nasal Tip Plasty: The Delivery Approach Revisited. Aesth Plast Surg
skin can produce hanging columella [2], that must be agreed with (2013) 37:16–21. [Crossref]
various maneuvers described.
Within this group, we can include the technique "delivery,"
considered a closed technique. This present technique characteristics
are similar to that described in the present work, since it exposes the
alar cartilage without an external incision. However, unlike what, it
was made through two parallel intranasal incisions, marginal and
intercartilaginous, which extend to the columella and nasal septum.
This double incision can easily develop abnormal scarring, disruption
of the internal nasal valve, due to the poorly executed
intercartilaginous incision [12] and defects at the soft triangle, due to
an inadequate incision and careless dissection [10]; All these reasons
support our preference for the semi-open technique, described in this
work.
In conclusion, the semi-open rhinoplasty provides the benefits of
both techniques: closed, because the incisions are limited only to the
nasal vestibule, without an external scar; and open, because the
technique widely exposes the nasal vault, in order to make all the
changes needed to the osteocartilaginous frame.
Declarations
• Acknowledgments: Not applicable.
• Funding: We have not received support funds.
• Availability of data and materials: The data and materials of this
study are available to interested parties.
Adv Plast Reconstr Surg, 2020 Page 330 of 330
You might also like
- Laparoscopic Appendectomy Discharge SummaryDocument2 pagesLaparoscopic Appendectomy Discharge SummaryJaslynn WhiteNo ratings yet
- Maxillectomy A ReviewDocument17 pagesMaxillectomy A ReviewDr. T. Balasubramanian100% (3)
- 2010 Facial Degloving Approach To The MidfaceDocument4 pages2010 Facial Degloving Approach To The MidfaceAFJimenezONo ratings yet
- Robotic Heart SurgeryDocument3 pagesRobotic Heart SurgeryLea ManingdingNo ratings yet
- Masseter Muscle Reattachment After Mandibular Angle SurgeryDocument4 pagesMasseter Muscle Reattachment After Mandibular Angle Surgery洪侊增No ratings yet
- 4 Oral Cavity ProceduresDocument10 pages4 Oral Cavity ProceduresAnne MarieNo ratings yet
- Orbitozygomatic Approach To Skull Base Lesions: Kafatabani Lezyonlarina Orbitozigomatik YaklasimDocument5 pagesOrbitozygomatic Approach To Skull Base Lesions: Kafatabani Lezyonlarina Orbitozigomatik YaklasimGaurav MedikeriNo ratings yet
- Midcheek Lift Using Facial Soft-Tissue Spaces of The MidcheekDocument11 pagesMidcheek Lift Using Facial Soft-Tissue Spaces of The MidcheekЩербакова ЛенаNo ratings yet
- Open SeptorhinoplastyDocument6 pagesOpen SeptorhinoplastybarbiemeNo ratings yet
- Review FrenectomyDocument6 pagesReview FrenectomyNyitnyit KunyitNo ratings yet
- Retromandibular Approach for Mandibular Condylar FracturesDocument4 pagesRetromandibular Approach for Mandibular Condylar FracturesAldo AguilarNo ratings yet
- CCrISP Administrator Handbook 20Document16 pagesCCrISP Administrator Handbook 20ash208750% (2)
- Semi-Open Rhinoplasty: Getting Together The Best of Both, Open and Closed RhinoplastyDocument5 pagesSemi-Open Rhinoplasty: Getting Together The Best of Both, Open and Closed RhinoplastyJorge Luis MarcosNo ratings yet
- Cers Cadwell LucDocument3 pagesCers Cadwell LucVictorioStokNo ratings yet
- Open Vs Closed VIP3Document10 pagesOpen Vs Closed VIP3Ahmad FareedNo ratings yet
- The Advantages of External DR PDFDocument13 pagesThe Advantages of External DR PDFalitNo ratings yet
- The TRICK-TIP Rhinoplasty: Tip of The Nose Preservation Using The Combined Synergy of Open and Closed ApproachesDocument11 pagesThe TRICK-TIP Rhinoplasty: Tip of The Nose Preservation Using The Combined Synergy of Open and Closed Approachesx5xxgpkhxfNo ratings yet
- Expanded Endonasal Approach - The Rostrocaudal Axis Part I PDFDocument12 pagesExpanded Endonasal Approach - The Rostrocaudal Axis Part I PDFIvonne PerezNo ratings yet
- Open Vs Closed VIP4Document6 pagesOpen Vs Closed VIP4Ahmad FareedNo ratings yet
- Beyond The Middle EarDocument12 pagesBeyond The Middle Earjay gauNo ratings yet
- Condilectomia Intra OralDocument7 pagesCondilectomia Intra OralJuan Carlos MeloNo ratings yet
- Caldwell Luc IncisionDocument3 pagesCaldwell Luc IncisionabdullahNo ratings yet
- Top of Page Patients and Methods Results Discussion Conclusion BibliographyDocument16 pagesTop of Page Patients and Methods Results Discussion Conclusion BibliographyentsrmcNo ratings yet
- Perichondrium Graft: Harvesting and Indications in Nasal SurgeryDocument5 pagesPerichondrium Graft: Harvesting and Indications in Nasal SurgerySyahnidel FitaNo ratings yet
- An Alternative Alar Cinch Suture PDFDocument11 pagesAn Alternative Alar Cinch Suture PDFmatias112No ratings yet
- Rhinology: Vol. 29 - No. 2 June 1991Document8 pagesRhinology: Vol. 29 - No. 2 June 1991Luis MartinezNo ratings yet
- Combined Transnasal and Transoral Endoscopic Approaches To The Craniovertebral JunctionDocument6 pagesCombined Transnasal and Transoral Endoscopic Approaches To The Craniovertebral JunctionRathavishwarajNo ratings yet
- Endonasal Dacryocystorhinostomy, About 52 CasesDocument5 pagesEndonasal Dacryocystorhinostomy, About 52 CasesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Endoscopic Myringoplasty and Tympanoplasty TechniquesDocument14 pagesEndoscopic Myringoplasty and Tympanoplasty TechniquesLuis De jesus SolanoNo ratings yet
- Double Mandibular Osteotomy With Coronoidectomy For Tumours in The Parapharyngeal SpaceDocument5 pagesDouble Mandibular Osteotomy With Coronoidectomy For Tumours in The Parapharyngeal SpaceSree BanNo ratings yet
- Pisa Tower Concept: A New Paradigm in Crooked Nose TreatmentDocument5 pagesPisa Tower Concept: A New Paradigm in Crooked Nose TreatmentImran AdeelNo ratings yet
- Four Cases of Preauricular Fistula Based On Systematic Review Resulted New AlgorithmDocument10 pagesFour Cases of Preauricular Fistula Based On Systematic Review Resulted New AlgorithmMuhammad Dody HermawanNo ratings yet
- Primary Rhinoplasty in Cleft Patients: Limited Open ApproachDocument7 pagesPrimary Rhinoplasty in Cleft Patients: Limited Open Approachsmansa123No ratings yet
- DownloadDocument6 pagesDownloadWita Eka Mardhiyahna AdzraNo ratings yet
- Maxilectomia TotalDocument18 pagesMaxilectomia TotalmonitosmaxilosNo ratings yet
- JC - Endoscopic Techniques in OralDocument33 pagesJC - Endoscopic Techniques in OralNarla SusheelNo ratings yet
- 2017 Article 1147 PDFDocument6 pages2017 Article 1147 PDFajaymanvikar007No ratings yet
- Lateral RhinotomyDocument11 pagesLateral RhinotomyDiaz RandanilNo ratings yet
- Transcranial Endoscopy: A Less Invasive AlternativeDocument4 pagesTranscranial Endoscopy: A Less Invasive AlternativebenedettoNo ratings yet
- Ceo 6 263Document3 pagesCeo 6 263Yusa Has JulianaNo ratings yet
- 05 CastelnuovoDocument7 pages05 Castelnuovogabriele1977No ratings yet
- 10.1007@s10006 019 00771 4Document5 pages10.1007@s10006 019 00771 4Karol Y. Wilson LondoñoNo ratings yet
- 10 1016@j Jclinane 2018 12 031Document2 pages10 1016@j Jclinane 2018 12 031mlnunezNo ratings yet
- Endoscopic Sinus Surgery: Indications and Complications: February 2020Document7 pagesEndoscopic Sinus Surgery: Indications and Complications: February 2020husnul khatimahNo ratings yet
- Applsci 10 08580 v2Document9 pagesApplsci 10 08580 v2rachmadyNo ratings yet
- Original Research Article: Amitkumar Rathi, Vinod Gite, Sameer Bhargava, Neeraj ShettyDocument8 pagesOriginal Research Article: Amitkumar Rathi, Vinod Gite, Sameer Bhargava, Neeraj ShettyAkanshaNo ratings yet
- The Management of Sinonasal Inverted Papilloma: Our ExperienceDocument7 pagesThe Management of Sinonasal Inverted Papilloma: Our Experiencesri ayu lestari wulandariNo ratings yet
- Jurnal THTDocument5 pagesJurnal THTSamuelRexyNo ratings yet
- Lateral Rhinotomy and Medial Maxillectomy ApproachDocument5 pagesLateral Rhinotomy and Medial Maxillectomy ApproachNuhu Bankwhot100% (1)
- Saddle Nose: Classification and Therapeutic Management: SciencedirectDocument8 pagesSaddle Nose: Classification and Therapeutic Management: Sciencedirectsmansa123No ratings yet
- FESSDocument5 pagesFESSMarco Antonio FigueroaNo ratings yet
- Carcinoma Maxillary Sinus : of TheDocument6 pagesCarcinoma Maxillary Sinus : of TheInesNo ratings yet
- Guidelines for endoscopic repair of cerebrospinal fluid leaksDocument8 pagesGuidelines for endoscopic repair of cerebrospinal fluid leaksMoustafa Amin AlyNo ratings yet
- A Novel Technique of Asian Tip Plasty by Dr. Man Koon, Suh From JW Plastic SurgeryDocument9 pagesA Novel Technique of Asian Tip Plasty by Dr. Man Koon, Suh From JW Plastic SurgeryJWPlasticsurgeryNo ratings yet
- Makiguchi 2014Document3 pagesMakiguchi 2014José Cunha CoutinhoNo ratings yet
- JC TopicDocument6 pagesJC Topicवाधूलं कण्णन् कुमारस्वामिNo ratings yet
- Editorial A Tailor Made Approach To Endoscopic Sinus Surgery ForDocument3 pagesEditorial A Tailor Made Approach To Endoscopic Sinus Surgery ForDR K C MALLIKNo ratings yet
- Nasal Hump Treatment With Cartilaginous Push-DownDocument46 pagesNasal Hump Treatment With Cartilaginous Push-Downdiego suescunNo ratings yet
- Lá ch0002Document15 pagesLá ch0002DiegoNo ratings yet
- A Comparative Study of Endoscopic Versus Conventional Septoplasty An Analysis of 50 CasesDocument6 pagesA Comparative Study of Endoscopic Versus Conventional Septoplasty An Analysis of 50 CasesDay LightNo ratings yet
- NOTES SINUS LIFT PP PresentationDocument3 pagesNOTES SINUS LIFT PP PresentationTuan NguyenNo ratings yet
- Open Rhinoplasty Techniques Compared to Closed ApproachesDocument3 pagesOpen Rhinoplasty Techniques Compared to Closed ApproachesmiadexxNo ratings yet
- Endoscopic Approach For Management of Septal Perforation: Isam AlobidDocument9 pagesEndoscopic Approach For Management of Septal Perforation: Isam AlobidLeslie Lindsay AlvarezNo ratings yet
- Advances in Vestibular Schwannoma Microneurosurgery: Improving Results with New TechnologiesFrom EverandAdvances in Vestibular Schwannoma Microneurosurgery: Improving Results with New TechnologiesLuciano MastronardiNo ratings yet
- APIC ImplementationPreventionGuide Web FIN03Document95 pagesAPIC ImplementationPreventionGuide Web FIN03t merchantNo ratings yet
- Zimmer Tapered Swiss Plus Implant System CatalogueDocument8 pagesZimmer Tapered Swiss Plus Implant System CatalogueGretaSmidtNo ratings yet
- The "Reality" of Health: Reality Television and The Public HealthDocument19 pagesThe "Reality" of Health: Reality Television and The Public HealthpatelchetakNo ratings yet
- ARAVIND EYE CARE SYSTEM: PROVIDING QUALITY EYE CARE FOR ALLDocument3 pagesARAVIND EYE CARE SYSTEM: PROVIDING QUALITY EYE CARE FOR ALLShruti MohapatraNo ratings yet
- Guias AsraDocument47 pagesGuias AsraAna Karen Rodriguez AldamaNo ratings yet
- Dental Surgery Degree Course OverviewDocument15 pagesDental Surgery Degree Course OverviewJANARDHAN H PNo ratings yet
- Allowed Amount Balance Billing Coinsurance Copayment Deductible Provider WWW - Healthcare.gov/sbc-GlossaryDocument7 pagesAllowed Amount Balance Billing Coinsurance Copayment Deductible Provider WWW - Healthcare.gov/sbc-GlossaryEmilyNo ratings yet
- Distal Extremities AnchorsDocument4 pagesDistal Extremities AnchorsCarolina Velasco de CampoverdeNo ratings yet
- History of Oral SurgeryDocument17 pagesHistory of Oral SurgeryAnupama NagrajNo ratings yet
- Enneking Stadializare OS MSKDocument15 pagesEnneking Stadializare OS MSKVlad RakoczyNo ratings yet
- DR - Madhav - Organ Preservation Treatment of CA PenisDocument31 pagesDR - Madhav - Organ Preservation Treatment of CA PenisDinesh .SNo ratings yet
- ASQ Sep 2019 PDFDocument76 pagesASQ Sep 2019 PDFJuan BarronNo ratings yet
- LASER IN CONSERVATIVE DENTISTRY -NHDocument39 pagesLASER IN CONSERVATIVE DENTISTRY -NHAiluul AlmaaNo ratings yet
- Xavier University-Ateneo de Cagayan College of Nursing: in Partial Fulfillment of The Requirements in NCM 112 (RLE)Document3 pagesXavier University-Ateneo de Cagayan College of Nursing: in Partial Fulfillment of The Requirements in NCM 112 (RLE)Ashley Jane MacapayadNo ratings yet
- Ultrasound Guided Clavipectoral Fascial Plane.23Document8 pagesUltrasound Guided Clavipectoral Fascial Plane.23Çağdaş BaytarNo ratings yet
- Steven JohnsonDocument3 pagesSteven JohnsonJuwandi RahmanNo ratings yet
- Test Bank For Olds Maternal Newborn Nursing and Womens Health Across The Lifespan 11th Edition by DavidsonDocument31 pagesTest Bank For Olds Maternal Newborn Nursing and Womens Health Across The Lifespan 11th Edition by DavidsonMartin Courser100% (31)
- Georgina Tracey Veterinary Nursing, Fetac Level 6Document8 pagesGeorgina Tracey Veterinary Nursing, Fetac Level 6Georgie TraceyNo ratings yet
- DePuy ASR Hip Recall Revision SurgeryDocument2 pagesDePuy ASR Hip Recall Revision SurgerydepuyhiprecallNo ratings yet
- Thesis ReportDocument96 pagesThesis ReportJenefa RubavathiNo ratings yet
- SinusitisDocument6 pagesSinusitisRae Marie AquinoNo ratings yet
- Ambulatory Surgery Center CodingDocument13 pagesAmbulatory Surgery Center CodingSundarajan ManiNo ratings yet
- Panduan Intermediate CycleDocument17 pagesPanduan Intermediate CyclemuhammadridhwanNo ratings yet
- Shouldice HospitalDocument10 pagesShouldice HospitalMuhammad SunnyNo ratings yet
- Courtney Braithwaites Appendectomy BrochureDocument2 pagesCourtney Braithwaites Appendectomy Brochureapi-246811319No ratings yet
- Consent FormDocument1 pageConsent FormNinan ThomasNo ratings yet