Professional Documents
Culture Documents
Immunotherapy and Biomarker Testing in Recurrent and Metastatic Head and Neck Cancers: ASCO Guideline
Uploaded by
DrDeepak MittalCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Immunotherapy and Biomarker Testing in Recurrent and Metastatic Head and Neck Cancers: ASCO Guideline
Uploaded by
DrDeepak MittalCopyright:
Available Formats
ASCO
Immunotherapy and Biomarker Testing in
Recurrent and Metastatic Head and Neck
special articles
Cancers: ASCO Guideline
Emrullah Yilmaz, MD, PhD1; Nofisat Ismaila, MD2; Julie E. Bauman, MPH, MD3; Raetasha Dabney, MD4; Gregory Gan, MD, PhD5;
Richard Jordan, DDS, PhD6; Marnie Kaufman7; Kedar Kirtane, MD8; Sean Matthew McBride, MD, MPH9; Matthew O. Old, MD10;
Lisa Rooper, MD11; Nabil F. Saba, MD12; Siddharth Sheth, DO, MPH13; Rathan M. Subramaniam, MD, PhD, MPH, MBA14,15;
Trisha Michel Wise-Draper, MD, PhD16; Deborah Wong, MD, PhD17; and Loren K. Mell, MD18
abstract
PURPOSE To provide evidence-based recommendations for practicing physicians and other health care pro-
viders on immunotherapy and biomarker testing for head and neck cancers.
METHODS ASCO convened an Expert Panel of medical oncology, surgical oncology, radiation oncology, radi-
ology, pathology, and patient advocacy experts to conduct a literature search, including systematic reviews,
meta-analyses, randomized controlled trials, and prospective and retrospective comparative observational
studies published from 2000 through 2022. Outcomes of interest included survival, overall response, and
locoregional control. Expert Panel members used available evidence and informal consensus to develop
evidence-based guideline recommendations.
RESULTS The literature search identified 28 relevant studies to inform the evidence base for this guideline.
RECOMMENDATIONS When possible, evidence-based recommendations were developed to address biomarker
testing, first-line treatment regimens based on programmed death ligand-1 scores, immunotherapy in platinum-
refractory recurrent or metastatic head and neck squamous cell carcinoma, immunotherapy in nasopharyngeal
carcinoma, and radiation therapy in combination with immunotherapy for treatment of local recurrence.
Additional information is available at www.asco.org/head-neck-cancer-guidelines.
J Clin Oncol 41:1132-1146. © 2022 by American Society of Clinical Oncology
INTRODUCTION treatment with or without chemotherapy.2-4 With the
Head and neck squamous cell carcinoma (HNSCC) advent of ICIs in cancer treatment, biomarkers such as
ASSOCIATED programmed death ligand-1 (PD-L1) and tumor mu-
CONTENT accounts for approximately 4% of all cancers in the
United States, with an estimated 66,470 new diagnoses tational burden (TMB) are gaining importance in
Appendix
selecting treatment options.5,6 Recently, clinical trials
Data Supplement and 15,050 deaths in 2022.1 HNSCC frequently arises
have begun using PD-L1 scoring systems for stratifi-
Author affiliations from the oral cavity, oropharynx, larynx, hypopharynx, or
cation and patient selection.4,7-9
and support nasopharynx, and more rarely from salivary glands or
information (if paranasal sinuses. Patients with HNSCC commonly The purpose of this guideline is to provide recom-
applicable) appear mendations to health care practitioners and patients
at the end of this
present with locoregionally advanced disease and often
article. receive multimodality treatments, including surgery, regarding immunotherapy and biomarker testing for
Accepted on October radiation therapy, and/or chemotherapy. Although this diverse and complex group of diseases.
27, 2022 and cisplatin is the most commonly used chemotherapy, the
published at GUIDELINE QUESTIONS
choice of chemotherapy depends on several factors,
ascopubs.org/journal/
jco on December 15, including prior use of platinum-based chemotherapy This clinical practice guideline addresses six over-
2022: DOI https://doi. and primary tumor site. arching clinical questions: (1) what biomarkers are
org/10.1200/JCO.22.
Recurrent or metastatic HNSCC is typically treated recommended for selecting HNSCC patients for anti–
02328
with systemic therapy involving chemotherapy and/or PD-1 ICI therapy? (2) What is the optimal first-line
Evidence Based
Medicine Committee immunotherapy. Immune-checkpoint inhibitors (ICIs) treatment regimen for recurrent or metastatic HNSCC
approval: were first approved in the treatment of patients with patients based on PD-L1 status? (3) What is the effect
October 12, 2022 platinum-refractory HNSCC and later in first-line of immunotherapy compared to other systemic
1132 Volume 41, Issue 5
Downloaded from ascopubs.org by 125.17.8.42 on February 19, 2023 from 125.017.008.042
Copyright © 2023 American Society of Clinical Oncology. All rights reserved.
Immunotherapy and Biomarker Testing in Head and Neck Cancers
THE BOTTOM LINE
Immunotherapy and Biomarker Testing in Recurrent and Metastatic Head and Neck Cancers: ASCO Guideline
Guideline Question
What is the role of immunotherapy with checkpoint inhibitors and biomarker testing in recurrent and metastatic head and neck
cancers?
Target Population
Patients with head and neck cancers.
Target Audience
Medical oncologists, radiation oncologists, surgical oncologists, clinical oncologists, radiologists, nurses, pathologists,
oncology pharmacists, caregivers, and patients.
Methods
An Expert Panel was convened to develop clinical practice guideline recommendations based on a systematic review of the
medical literature.
Recommendations
Recommendation 1.1. PD-L1 immunohistochemistry testing should be performed in patients with recurrent or metastatic
HNSCC (Type: Evidence based, benefits outweigh harms; Evidence quality: High; Strength of recommendation: Strong).
Recommendation 1.2. PD-L1 combined positive score (CPS) $ 1 should be interpreted as positive and correlates with a
clinical benefit to programmed cell death protein-1 (PD-1) inhibitors (Type: Evidence based, benefits outweigh harms;
Evidence quality: High; Strength of recommendation: Strong).
Recommendation 1.3. TMB testing may be performed in patients with recurrent or metastatic HNSCC when CPS is not
available or in patients with rare tumors (Type: Evidence based, benefits outweigh harms; Evidence quality: High; Strength of
recommendation: Strong).
Recommendation 1.4. TMB $ 10 should be interpreted as high and correlates with a clinical benefit to PD-1 inhibitors (Type:
Evidence based, benefits outweigh harms; Evidence quality: High; Strength of recommendation: Strong).
Recommendation 2.1. Pembrolizumab monotherapy or pembrolizumab, platinum, and fluorouracil should be offered as first-
line treatment for patients with recurrent or metastatic HNSCC with a CPS $ 1 (Type: Evidence based, benefits outweigh
harms; Evidence quality: High; Strength of recommendation: Strong).
Recommendation 2.2. Pembrolizumab, platinum, and fluorouracil may be offered as first-line treatment for patients with
recurrent or metastatic HNSCC with a CPS , 1 (Type: Evidence based, benefits outweigh harms; Evidence quality: Moderate;
Strength of recommendation: Strong).
Recommendation 3.1. Pembrolizumab or nivolumab should be offered to patients with platinum-refractory recurrent or
metastatic HNSCC, regardless of CPS status (Type: Evidence based, benefits outweigh harms; Evidence quality: High;
Strength of recommendation: Strong).
Recommendation 4.1. Toripalimab, camrelizumab, or tislelizumab, with gemcitabine and cisplatin, should be offered as first-
line treatment for patients with recurrent or metastatic nasopharyngeal cancer (Type: Evidence based, benefits outweigh
harms; Evidence quality: High; Strength of recommendation: Strong).
Qualifying statement: Pembrolizumab or nivolumab may be offered with gemcitabine and cisplatin if the ICIs in Recom-
mendation 4.1 are unavailable.
Recommendation 4.2. PD-1 inhibitors may be offered to patients with recurrent or metastatic nasopharyngeal cancer who
have progressed following platinum-based therapy (Type: Informal consensus, benefits outweigh harms; Evidence quality:
Low; Strength of recommendation: Weak).
Recommendation 5.1. For patients with oligometastatic HNSCC, radiation therapy is safe to give concurrently with immu-
notherapy for the purpose of palliation or local control, but should not be given to enhance response to immunotherapy outside
of a clinical trial (Type: Evidence based, no net benefit; Evidence quality: Moderate; Strength of recommendation: Weak).
Recommendation 6.1. Pembrolizumab may be offered to patients with TMB-high recurrent or metastatic rare head and neck
cancers (Type: Evidence based, benefits outweigh harms; Evidence quality: Moderate; Strength of recommendation: Weak).
Recommendation 6.2. Pembrolizumab may be offered to patients with PD-L1–positive recurrent or metastatic salivary gland
cancer (Type: Evidence based, benefits outweigh harms; Evidence quality: Moderate; Strength of recommendation: Weak).
(continued on following page)
Journal of Clinical Oncology 1133
Downloaded from ascopubs.org by 125.17.8.42 on February 19, 2023 from 125.017.008.042
Copyright © 2023 American Society of Clinical Oncology. All rights reserved.
Yilmaz et al
THE BOTTOM LINE (CONTINUED)
Additional Resources
Definitions for the quality of the evidence and strength of recommendation ratings are available in Appendix Table A1 (online
only). More information, including a supplement with additional evidence tables, slide sets, and clinical tools and resources, is
available at www.asco.org/head-neck-cancer-guidelines. The Methodology Manual (available at www.asco.org/guideline-
methodology) provides additional information about the methods used to develop this guideline. Patient information is
available at www.cancer.net.
ASCO believes that cancer clinical trials are vital to inform medical decisions and improve cancer care, and that all patients
should have the opportunity to participate.
treatments in platinum-refractory recurrent or metastatic inclusion in the systematic review based on the following
HNSCC? (4) What is the role of immunotherapy for patients criteria:
with recurrent or metastatic nasopharyngeal carcinoma
1. Population: patients with HNSCC of the oral cavity,
(NPC)? (5) What is the effect of radiation therapy in
oropharynx, hypopharynx, or larynx, recurrent or
combination with anti–PD-(L)1 immunotherapy compared
metastatic disease, NPC, or rare head and neck
to immunotherapy alone for the treatment of locoregionally
cancers.
recurrent or oligometastatic HNSCC? (6) What is the role of
2. Interventions: immunotherapy, biomarker tests.
immunotherapy for rare head and neck cancers?
3. Comparisons: chemotherapy.
4. Outcomes: survival, response, and locoregional
METHODS control.
Guideline Development Process Articles were excluded from the systematic review if they
This systematic review-based guideline was developed by a were (1) meeting abstracts not subsequently published in
multidisciplinary Expert Panel, which included a patient peer-reviewed journals; (2) editorials, commentaries, let-
representative and an ASCO guidelines staff member with ters, news articles, case reports, and narrative reviews; and
health research methodology expertise (Appendix Table A2, (3) published in a non-English language. The guideline
online only). Three full panel meetings were held and recommendations are crafted, in part, using the Guidelines
members were asked to provide ongoing input on the quality Into Decision Support methodology and accompanying
and assessment of the evidence, generation of recom-
BRIDGE-Wiz software.10 In addition, a guideline imple-
mendations, draft content, and to review and approve drafts
mentability review was conducted. Based on the imple-
during the entire development of the guideline. ASCO staff
met routinely with the Expert Panel co-chairs and corre- mentability review, revisions were made to the draft to
sponded with the panel via e-mail to coordinate the process clarify recommended actions for clinical practice. Ratings
to completion. The guideline recommendations were sent for for type and strength of the recommendation, and evidence
an open comment period of 2 weeks allowing the public to quality are provided with each recommendation. The
review and comment on the recommendations after sub- quality of the evidence for each outcome was assessed
mitting a confidentiality agreement. These comments were using the Cochrane Risk of Bias tool and elements of the
taken into consideration when finalizing the recommenda- GRADE quality assessment and recommendations devel-
tions. Members of the Expert Panel were responsible for opment process.11,12 GRADE quality assessment labels (ie,
reviewing and approving the penultimate version of the high, moderate, low, and very low) were assigned for each
guideline, which was then submitted to the Journal of Clinical outcome by the project methodologist in collaboration with
Oncology for editorial review and consideration for publi- the Expert Panel co-chairs and reviewed by the full Expert
cation. All ASCO guidelines are ultimately reviewed and
Panel.
approved by the Expert Panel and the ASCO Evidence Based
Medicine Committee before publication. All funding for the The ASCO Expert Panel and guidelines staff work with co-
administration of the project was provided by ASCO. chairs to keep abreast of any substantive updates to the
The recommendations were developed through a sys- guideline. Based on formal review of the emerging litera-
tematic review of evidence identified via online searches of ture, ASCO will determine the need to update. The ASCO
PubMed (January 2000-February 2022) and Cochrane Guidelines Methodology Manual (available at
Library (January 2000-February 2022) of phase III ran- www.asco.org/guideline-methodology) provides additional
domized clinical trials (RCTs), selected observational information about the guideline update process. This is the
studies, and clinical experience. Articles were selected for most recent information as of the publication date.
1134 © 2022 by American Society of Clinical Oncology Volume 41, Issue 5
Downloaded from ascopubs.org by 125.17.8.42 on February 19, 2023 from 125.017.008.042
Copyright © 2023 American Society of Clinical Oncology. All rights reserved.
Immunotherapy and Biomarker Testing in Head and Neck Cancers
Guideline Disclaimer accordance with the Policy, the majority of the members of
The Clinical Practice Guidelines and other guidance the Expert Panel did not disclose any relationships con-
published herein are provided by the American Society of stituting a conflict under the Policy.
Clinical Oncology, Inc (ASCO) to assist providers in clinical
decision making. The information herein should not be RESULTS
relied upon as being complete or accurate, nor should it be Characteristics of Studies Identified in the
considered as inclusive of all proper treatments or methods Literature Search
of care or as a statement of the standard of care. With the
A total of 1,167 citations after duplicate removal were
rapid development of scientific knowledge, new evidence
identified in the literature search. After applying the eligi-
may emerge between the time information is developed
bility criteria, 28 references remained, forming the evi-
and when it is published or read. The information is not
dentiary basis for the guideline recommendations.2-4,13-37
continually updated and may not reflect the most recent
evidence. The information addresses only the topics spe- The identified trials were published between 2016 and
cifically identified therein and is not applicable to other 2022, and included one systematic review,13 eight phase III
interventions, diseases, or stages of diseases. This infor- RCTs2,14-18 with one study having eight publications3,19-25
mation does not mandate any particular course of medical and another having two publications,4,26 seven phase II
care. Further, the information is not intended to substitute RCTs,27-33 one phase Ib,34 and three cohort studies.35-37
for the independent professional judgment of the treating These studies focused on biomarker testing, first-line
provider, as the information does not account for individual treatment regimens based on PD-L1 scores, immuno-
variation among patients. Recommendations specify the therapy in platinum-refractory recurrent or metastatic
level of confidence that the recommendation reflects the HNSCC, immunotherapy in NPC, and radiation therapy in
net effect of a given course of action. The use of words like combination with immunotherapy for treatment of local
“must,” “must not,” “should,” and “should not” indicates recurrence. Primary outcomes reported include overall
that a course of action is recommended or not recom- survival (OS), progression-free survival (PFS), objective
mended for either most or many patients, but there is response rate, and overall response rate (ORR).
latitude for the treating physician to select other courses of Details on the study characteristics are included in the Data
action in individual cases. In all cases, the selected course Supplement (online only). The systematic review flow di-
of action should be considered by the treating provider in agram is shown in the Data Supplement.
the context of treating the individual patient. Use of the
Evidence Quality Assessment
information is voluntary. ASCO does not endorse third party
drugs, devices, services, or therapies used to diagnose, The quality of evidence was assessed for each outcome of
treat, monitor, manage, or alleviate health conditions. Any interest. This rating includes factors such as study design,
use of a brand or trade name is for identification purposes consistency of results, directness of evidence, precision,
only. ASCO provides this information on an “as is” basis and publication bias, and magnitude of effect, assessed by one
makes no warranty, express or implied, regarding the in- reviewer. Evidence quality ratings for the outcomes of in-
formation. ASCO specifically disclaims any warranties of terest are provided in the Data Supplement. Refer to Ap-
merchantability or fitness for a particular use or purpose. pendix Table A1, for definitions for the quality of the
ASCO assumes no responsibility for any injury or damage to evidence, and the Methodology Manual for more
persons or property arising out of or related to any use of this information.
information, or for any errors or omissions.
Guideline and Conflicts of Interest RECOMMENDATIONS
The Expert Panel was assembled in accordance with Clinical Question 1
ASCO’s Conflict of Interest Policy Implementation for What biomarkers are recommended for selecting HNSCC
Clinical Practice Guidelines (“Policy,” found at https:// patients for anti–PD-1 ICI therapy?
www.asco.org/guideline-methodology). All members of
Recommendation 1.1. PD-L1 immunohistochemistry test-
the expert panel completed ASCO’s disclosure form, which
ing should be performed in patients with recurrent or
requires disclosure of financial and other interests, in-
metastatic HNSCC (Type: Evidence based, benefits out-
cluding relationships with commercial entities that are
weigh harms; Evidence quality: High; Strength of recom-
reasonably likely to experience direct regulatory or com-
mendation: Strong).
mercial impact as a result of promulgation of the guideline.
Categories for disclosure include employment; leadership; Recommendation 1.2. PD-L1 CPS $ 1 should be inter-
stock or other ownership; honoraria, consulting or advisory preted as positive and correlates with a clinical benefit to
role; speaker’s bureau; research funding; patents, royalties, PD-1 inhibitors (Type: Evidence based, benefits outweigh
other intellectual property; expert testimony; travel, ac- harms; Evidence quality: High; Strength of recommenda-
commodations, expenses; and other relationships. In tion: Strong).
Journal of Clinical Oncology 1135
Downloaded from ascopubs.org by 125.17.8.42 on February 19, 2023 from 125.017.008.042
Copyright © 2023 American Society of Clinical Oncology. All rights reserved.
Yilmaz et al
Literature review and clinical interpretation. Expression of performed and received PD-1 inhibitors. The total number
PD-L1 as determined by immunohistochemistry correlates of somatic nonsynonymous mutations was normalized to
with clinical response to ICI among multiple tumor types, the total number of megabases sequenced. Those with
including HNSCC. Pathologists can assess PD-L1 positivity increased TMB were found to have significantly improved
using either CPS, defined as the number of tumor cells, OS. The top 20th percentile for HNSCC for TMB was above
lymphocytes, and macrophages that express PD-L1 di- 10.3 MB, which significantly correlated with improved OS
vided by the total number of tumor cells and multiplied by with PD-1 inhibitors.39 Therefore, HNSCC patients with
100, or tumor proportion score (TPS), defined as the TMB of $ 10 MB should be considered high, and testing
percentage of tumor cells that express PD-L1, at various may be performed in patients for whom CPS is not avail-
cutoff points. Meta-analysis of 11 clinical trials indicated able, as those with high TMB may benefit from PD-1 in-
that PD-L1–positive head and neck cancer treated with ICI hibitors. In addition, retrospective analysis of biomarkers in
had improved OS at 6 and 12 months compared to tumors 192 patients in the KEYNOTE-012 study confirmed an
that did not express PD-L1, regardless of either CPS or TPS association between TMB and ICI response and demon-
scoring or numerical cutoffs used for defining PD-L1 strated no correlation between TMB and PD-L1.40
positivity.13 Nevertheless, CPS has emerged as the supe-
Clinical Question 2
rior marker. In post hoc receiver operating characteristic
curve analysis of KEYNOTE-040 data, CPS and TPS What is the optimal first-line treatment regimen for recur-
appeared to show equivalent performance at a cutoff rent or metastatic HNSCC patients based on PD-L1 status?
of $ 50; however, CPS was more sensitive than TPS at a Recommendation 2.1. Pembrolizumab monotherapy or
lower cutoff of $ 1.14 As such, CPS scoring is preferred for pembrolizumab, platinum, and fluorouracil (5-FU) should
maximum sensitivity, although a TPS score be offered as first-line treatment for patients with recurrent
indicating $ 1% positivity is correlated with benefit to ICI or metastatic HNSCC with a CPS $ 1 (Type: Evidence
and may be interpreted as positive if available. A lower based, benefits outweigh harms; Evidence quality: High;
threshold for defining CPS positivity of $ 1 is also preferred. Strength of recommendation: Strong).
In KEYNOTE-048 and subgroup analysis, CPS cutoffs of
both $ 20 and $ 1 were associated with superior OS,4,26 Literature review and clinical interpretation. This recom-
leading to adoption of the lower cutoff to maximize sensi- mendation is based on findings from KEYNOTE-048,4
tivity. Some additional variables, including intratumoral which was a randomized, open-label, phase III clinical
heterogeneity, temporal heterogeneity, size of sample trial comparing the EXTREME regimen consisting of che-
stained, and type of sample stained, may impact assess- motherapy (platinum, 5-FU) and cetuximab versus pem-
ment of PD-L1 expression, although variable use of CPS brolizumab monotherapy or pembrolizumab and
and TPS and divergent definitions of positivity makes it chemotherapy in recurrent or metastatic HNSCC. Patients
challenging to draw definitive conclusions from existing with a CPS $ 1 had improved OS with pembrolizumab
literature. The relationship between human papillomavirus monotherapy compared to chemotherapy and cetuximab
(HPV) and P16 status and response to ICI also is not yet (hazard ratio [HR], 0.78; 95% CI, 0.64 to 0.96; P 5 .0086).
fully established, although a pooled analysis of six clinical Median OS was 12.3 months (95% CI, 10.8 to 14.9) in
trials recently did not demonstrate a link between HPV patients receiving pembrolizumab monotherapy compared
(P16) positivity and PD-L1 expression.38 to 10.3 months (95% CI, 9.0 to 11.5) in patients receiving
cetuximab with chemotherapy. However, patients with
Recommendation 1.3. TMB testing may be performed in CPS $ 20 derived the greatest benefit with pembrolizumab
patients with recurrent or metastatic HNSCC when CPS is monotherapy compared to chemotherapy and cetuximab
not available or in patients with rare tumors (Type: Evidence (HR, 0.61; 95% CI, 0.45 to 0.83; P 5 .0007). Median
based, benefits outweigh harms; Evidence quality: High; OS was 14.9 months (95% CI, 11.6 to 21.5) with
Strength of recommendation: Strong). pembrolizumab monotherapy compared to 10.7 months
(95% CI, 8.8 to 12.8) in the cetuximab with chemotherapy
Recommendation 1.4. TMB $ 10 should be interpreted as group.
high and correlates with a clinical benefit to PD-1 inhibitors
Deciding on the plausibility of chemoimmunotherapy ver-
(Type: Evidence based, benefits outweigh harms; Evidence
sus immunotherapy in patients with previously untreated
quality: High; benefits outweighs harms; Strength of rec-
recurrent or metastatic HNSCC must take into consider-
ommendation: Strong).
ation the clinical presentation and urgency for achieving a
Literature review and clinical interpretation. TMB was response. Chemoimmunotherapy may therefore be a
shown to correlate with clinical response to ICI among plausible option even in biomarker-positive disease in case
multiple tumor types including HNSCC. Although no ran- a rapid reduction in tumor burden is deemed clinically
domized trials have been performed in HNSCC, using necessary. Response rates to single-agent pembrolizumab
patients sequenced on MSK-IMPACT, 138 HNSCC patients remain close to 20%, regardless of prior exposure to
were identified who had nonsynonymous somatic TMB therapy or PD-L1 expression,41,42 supporting the
1136 © 2022 by American Society of Clinical Oncology Volume 41, Issue 5
Downloaded from ascopubs.org by 125.17.8.42 on February 19, 2023 from 125.017.008.042
Copyright © 2023 American Society of Clinical Oncology. All rights reserved.
Immunotherapy and Biomarker Testing in Head and Neck Cancers
chemoimmunotherapy paradigm in situations where early care single-agent therapy (methotrexate, docetaxel, or
response is a primary objective. cetuximab).2,3 Both studies enrolled HNSCC patients with
HPV status may influence response to anti–PD-1 therapy, disease progression within 6 months after platinum-based
with a large meta-analysis reporting greater efficacy of PD-1 chemotherapy. A key difference was KEYNOTE-040 ex-
inhibitors in smokers and HPV-negative patients.43 How- cluded patients with disease progression within 0-3 months.
ever, current data do not support changing recommen- Major findings from these trials include a statistically sig-
dations for the addition or exclusion of anti–PD-1 therapies nificant OS benefit (8.4 and 7.5 months, respectively)
in the recurrent and/or metastatic setting with regard to the compared to the control arm. Additionally, lower rates of
HPV status. grade 3 and 4 treatment-related adverse events (AEs) were
observed in patients treated with anti–PD-1 therapies
Recommendation 2.2. Pembrolizumab, platinum, and 5-FU compared to standard of care. Importantly, the OS benefit
may be offered as first-line treatment for patients with re- was independent of HPV status or PD-L1 expression, which
current or metastatic HNSCC with a CPS , 1 (Type: has been confirmed in a long-term follow up study.21 These
Evidence based, benefits outweigh harms; Evidence quality: findings supported the US Food and Drug Administration
Moderate; Strength of recommendation: Strong). approval of both pembrolizumab and nivolumab in the
Literature review and clinical interpretation. Recurrent or advanced-line setting after progression on or following
metastatic HNSCC is a heterogeneous disease presenting platinum-containing therapies, regardless of PD-L1 ex-
many different possible clinical scenarios. Based on the pression. Therefore, we recommend single-agent pem-
results of the KEYNOTE-048 phase III trial, the combination brolizumab or nivolumab for patients with recurrent or
of pembrolizumab, platinum, and 5-FU has been approved metastatic HNSCC with disease progression within 6 months
as a therapeutic option for patients with recurrent or of platinum-based chemotherapy.
metastatic HNSCC regardless of PD-L1 status or CPS The combination of anti–PD-1 inhibitors with other sys-
score.4 Patients in the overall population had prolonged temic treatments has been investigated in platinum-
survival with pembrolizumab and chemotherapy compared refractory disease; however, no combination has become
to cetuximab with chemotherapy group (HR, 0.77; 95% CI, standard of care to date. The anti–epidermal growth factor
0.70 to 0.99; P 5 .0034). Median OS was 13 months in the receptor has been one potential target, with data from
pembrolizumab with chemotherapy group compared to multiple single-arm, phase II studies.44-46 A study of
10.7 months in the cetuximab with chemotherapy group in pembrolizumab and cetuximab showed 45% response rate
the total population regardless of PD-L1 status. Subgroup with a median PFS of 6.5 months and a median OS of
analysis was performed by PD-L1 CPS subgroups in 18.4 months in recurrent or metastatic HNSCC.44 This trial
KEYNOTE 048 study.26 Median OS was 11.3 months in the included a high percentage (64%) of patients with
pembrolizumab with chemotherapy group compared to platinum-refractory disease. A study of nivolumab and
10.7 months in the cetuximab with chemotherapy group cetuximab enrolled patients with recurrent or metastatic
(HR, 1.12; 95% CI, 0.76 to 1.94; P 5 .78932). Although a HNSCC with a median PFS of 7.8 months and a median OS
small number of patients were in the PD-L1 CPS , 1 of 14.5 months. In the 12 patients with platinum-refractory
subgroup (39 and 43 respectively) and the study was not disease, the response rate was 42%.45,46 Additional data
powered to evaluate efficacy of pembrolizumab with che- from randomized trials evaluating anti–PD-1 and cetux-
motherapy in this subgroup, cetuximab with chemotherapy imab combinations in the platinum-refractory, recurrent or
may also be considered for these patients.41,42 metastatic HNSCC setting are needed prior to incorporation
Clinical Question 3 into standard clinical practice.
What is the effect of immunotherapy compared to other The evaluation of an anti–PD-1 inhibitor and cytotoxic T-cell
systemic treatments in platinum-refractory recurrent or lymphocyte-4 inhibitor combination in platinum-refractory
metastatic HNSCC? HNSCC was conducted in the EAGLE trial.17 Durvalumab
with or without tremelimumab was evaluated versus
Recommendation 3.1. Pembrolizumab or nivolumab standard-of-care therapy.17 There was no significant dif-
should be offered to patients with platinum-refractory re- ference in OS by treatment arm, indicating the lack of
current or metastatic HNSCC, regardless of CPS status benefit of adding cytotoxic T-cell lymphocyte-4 inhibition to
(Type: Evidence based, benefits outweigh harms; Evidence this patient population.
quality: High; Strength of recommendation: Strong).
Clinical Question 4
Literature review and clinical interpretation. Systemic
What is the role of immunotherapy for patients with re-
therapy with palliative intent is indicated for patients with
current or metastatic NPC?
platinum-refractory, recurrent or metastatic HNSCC. Two
phase III trials, KEYNOTE-040 and CheckMate 141, eval- Recommendation 4.1. Toripalimab, camrelizumab, or
uated anti–PD-1 therapies, pembrolizumab (KEYNOTE-040) tislelizumab, with gemcitabine and cisplatin, should be
and nivolumab (CheckMate 141), compared to standard-of- offered as first-line treatment for patients with recurrent or
Journal of Clinical Oncology 1137
Downloaded from ascopubs.org by 125.17.8.42 on February 19, 2023 from 125.017.008.042
Copyright © 2023 American Society of Clinical Oncology. All rights reserved.
Yilmaz et al
metastatic NPC (Type: Evidence based, benefits outweigh PFS (9.7 v 6.9 months; HR, 0.54; 95% CI, 0.39 to 0.76),
harms; Evidence quality: High; Strength of recommenda- with a longer median DOR (9 v 6 months), was seen for the
tion: Strong). camrelizumab arm compared to placebo. Median OS had
Qualifying statement: Pembrolizumab or nivolumab may be not been reached at the time of the data cutoff. Given the
offered with gemcitabine and cisplatin if the ICIs in Rec- strength of the evidence from both JUPITER-02 and
ommendation 4.1 are unavailable. CAPTAIN-1st, where available, toripalimab or camreli-
zumab may be offered in combination with GC for frontline
Literature review and clinical interpretation. The benefit of treatment of recurrent or metastatic NPC, irrespective of
adding anti–PD-1 immunotherapy to gemcitabine- PD-L1 expression levels.16
platinum for recurrent or metastatic NPC as a first-line
treatment has been evaluated. The phase III trial The RATIONALE-309 trial, presented as an abstract at
ASCO 2022,47 was of similar design to JUPITER-02 and
JUPITER-02 randomized 289 patients 1:1 to gemcitabine
CAPTAIN-1st. In this trial, 263 subjects with recurrent or
and cisplatin (GC) with either toripalimab, a humanized
metastatic NPC were randomly assigned 1:1 to six cycles of
IgG4K monoclonal PD-1 antibody, or placebo.15 Patients
GC with either tislelizumab or placebo administered for 4-6
with recurrent or metastatic NPC who had not previously
cycles, followed by tislelizumab or placebo once every
received systemic therapy in the recurrent or metastatic
3 weeks. In contrast to the aforementioned studies, wherein
setting were eligible. Notably, subjects were eligible for
up to 2 years of maintenance anti–PD-1 immunotherapy
enrollment irrespective of the level of tumor PD-L1 posi-
was administered, treatment with tislelizumab continued
tivity. Patients received up to six cycles of GC (gemcitabine
until disease progression, unacceptable toxicity, or subject
1,000 mg/m2 days 1 and 8, cisplatin 80 mg/m2 day 1) with
withdrawal. Furthermore, crossover to tislelizumab mono-
toripalimab 240 mg or placebo once every 21 days, fol- therapy was allowed for patients allocated to placebo at the
lowed by up to 2 years of toripalimab or placebo. The time of independent review committee–assessed disease
primary end point was PFS by blinded independent review progression. With a median follow up of 15.5 months, PFS
committee. Secondary end points were investigator- was improved in the tislelizumab arm (HR, 0.50; 95% CI,
assessed PFS, OS, ORR, duration of response (DOR), 0.37 to 0.68). Median PFS was 9.6 months (95% CI, 7.6 to
disease control rate, and 1- and 2-year PFS and OS rates. 11.7) versus 7.4 months (95% CI, 5.7 to 7.6) in the
The addition of toripalimab to GC resulted in significantly tislelizumab versus placebo arm, respectively. This evi-
improved PFS compared to placebo with GC (11.7 v dence from three different phase III trials of similar size and
8.0 months; HR, 0.52; 95% CI, 0.36 to 0.74). Improved design shows improved PFS with the combination of ICI
PFS with toripalimab was seen in both PD-L1–negative and GC, with similar effect sizes. Notably, toxicity seems to
(tumor cell and immune cell PD-L1 immunohistochem- be manageable, and the clinical benefit appears to be
istry , 1%) and PD-L1–positive (tumor cell or immune cell independent of tumor PD-L1 status. Further evaluation of
PD-L1 immunohistochemistry $ 1%) subgroups. While such regimens is needed in Epstein-Barr virus (EBV)–
median OS had not yet been reached for either arm at the negative disease.
time of the data cutoff, a 40% reduction in risk of death
Given the strength of the evidence from JUPITER-02,
was observed in the toripalimab arm compared to the
CAPTAIN-1st, and RATIONALE-309, where available,
placebo arm, with a stratified HR for mortality of 0.603 toripalimab, camrelizumab, or tislelizumab may be offered
(95% CI, 0.364 to 0.997; P 5 .0462) favoring toripalimab. in combination with GC for frontline treatment of recurrent
While most toxicities were comparable, and the incidence or metastatic NPC, irrespective of PD-L1 expression levels.
of AEs leading to discontinuation were similar, for tor-
ipalimab and placebo arms (7.5% v 4.9%), immune- Recommendation 4.2. PD-1 inhibitors may be offered to
related AEs were significantly higher in the toripalimab patients with recurrent or metastatic nasopharyngeal
arm.15 cancer who have progressed following platinum-based
therapy (Type: Informal consensus, benefits outweigh
A parallel study, CAPTAIN-1st, was a double-blinded,
harms; Evidence quality: Low; Strength of recommenda-
placebo-controlled phase III trial evaluating the addition
tion: Weak).
of camrelizumab, an anti–PD-1 IgG4 monoclonal anti-
body, versus placebo, in combination with GC. The trial Literature review and clinical interpretation. The benefit of
randomly assigned 263 subjects 1:1 to camrelizumab anti–PD-1 immunotherapy in patients with recurrent or
200 mg IV or placebo plus GC (gemcitabine 1,000 mg/m2 metastatic NPC who have progressed on frontline platinum-
day 1, 8; cisplatin 80 mg/m2 day 1) once every 21 days for based chemotherapy has been evaluated in several
4-6 cycles followed by up to 2 years of camrelizumab or studies.18,27,48,49 KEYNOTE-122 randomly assigned 233
placebo. Similar to JUPITER-02, eligible subjects had patients with recurrent or metastatic NPC who had pro-
treatment-naive recurrent or metastatic NPC with any level gressed on frontline platinum-based chemotherapy 1:1 to
of PD-L1 expression. The primary end point was either pembrolizumab 200 mg IV once every 3 weeks up to
investigator-assessed PFS. An improvement in median 35 cycles or investigator’s choice chemotherapy
1138 © 2022 by American Society of Clinical Oncology Volume 41, Issue 5
Downloaded from ascopubs.org by 125.17.8.42 on February 19, 2023 from 125.017.008.042
Copyright © 2023 American Society of Clinical Oncology. All rights reserved.
Immunotherapy and Biomarker Testing in Head and Neck Cancers
(capecitabine, gemcitabine, or docetaxel). The primary end Recommendation 5.1. For patients with oligometastatic
point was OS. Secondary end points were PFS, ORR, and HNSCC, radiation therapy is safe to give concurrently with
DOR. With a median follow-up of 45 months, median OS immunotherapy for the purpose of palliation or local control,
was not statistically different between the two arms: but should not be given to enhance response to immu-
17.2 months for pembrolizumab versus 15.3 months for notherapy outside of a clinical trial (Type: Evidence based,
chemotherapy (HR, 0.90; 95% CI, 0.67 to 1.19; P 5 .226). no net benefit; Evidence quality: Moderate; Strength of
Median OS for patients with PD-L1 CPS $ 1 was also similar recommendation: Weak).
in the two arms (17.2 months for pembrolizumab v
Literature review and clinical interpretation. To date, a lone
18.0 months for chemotherapy); however, the incidence of
randomized phase II trial has evaluated the benefit of
treatment-related AEs was lower for the pembrolizumab
adding radiation therapy to anti–PD-(L)1 immunotherapy in
group compared to the chemotherapy group (61.2% v
patients with locoregionally recurrent or oligometastatic
87.5%, respectively), as was the incidence of grade 3 to 5
HNSCC. McBride et al32 randomly assigned 62 patients
toxicity (10.3% for pembrolizumab v 43.8% for
with metastatic HNSCC or WHO grade 1 to 3 NPC—without
chemotherapy).18
restriction according to number of metastases or HPV or
Two phase II studies of nivolumab for recurrent or metastatic EBV status—to either nivolumab alone or nivolumab with
NPC have been reported.48,49 In NCI-4792, 44 recurrent or stereotactic body radiation therapy (SBRT). SBRT was
metastatic NPC patients previously treated with platinum- delivered as 27 Gy in three fractions, was initiated between
based chemotherapy received nivolumab 3 mg/kg once the first and second doses of nivolumab, and was directed
every 2 weeks. Nine objective responses were seen (21%; at a single metastatic lesion. The primary outcome was
one complete and eight partial responses). 1-Year PFS and ORR using RECIST 1.1 criteria; PFS and OS were sec-
OS were 19% and 59%.48 CheckMate-358 was a multi- ondary end points. In brief, there was no significant
cohort study of nivolumab in five virally associated cancers, difference in ORR (34.5% v 29%, P 5 .86), median PFS
including recurrent or metastatic NPC. Twenty-four patients (1.9 v 2.6 months, P 5 .79), or median OS (14.2 v
with nonkeratinizing disease who had received no more than 13.6 months) between the nivolumab alone versus
nivolumab 1 SBRT arms. The 1-year OS was 50.2% with
two prior lines of therapy in the recurrent or metastatic setting
nivolumab alone versus 54.4% with nivolumab 1 SBRT. In
were treated with nivolumab 240 mg IV once every 2 weeks
a preplanned subgroup analysis, a test for interaction
until progression or unacceptable toxicity. Primary end
between HPV- or EBV-positive status and treatment arm
points were ORR and safety. At a median follow-up of
was nonsignificant. There was no significant difference in
26 weeks, ORR was 20.8%; responses were irrespective of any AEs or grade 3 to 5 AEs between the two arms.
PD-L1 positivity.49
The CHEERS trial evaluated the addition of SBRT to im-
In POLARIS-02, 190 patients with recurrent or metastatic munotherapy in metastatic solid tumors and included a
NPC who had progressed on prior platinum-based che- small subgroup (n 5 20) of HNSCC patients.50 There were
motherapy were treated with toripalimab 3 mg/kg once no restrictions on number of metastases. Investigators
every 2 weeks until disease progression or unacceptable selected the anti–PD-(L)1 immunotherapy, with the timing
toxicity. The primary end point (ORR) was 20.5% (95% CI, and SBRT schema like McBride et al32 (24 Gy in three
15.0 to 27.0) in the total cohort. Median PFS was fractions, treating up to a maximum of three lesions started
1.9 months (95% CI, 1.8 to 3.5) and median OS was after completion of cycle 1 of immunotherapy). Again, the
17.4 months (95% CI, 11.7 to 22.9). For the 92 patients authors found no benefit in ORR, PFS, or OS with the
who had failed at least two lines of prior therapy, ORR was addition of SBRT to anti–PD-(L)1 immunotherapy.
23.9% (95% CI, 31.1 to 52.1). ORR was similar in PD-L1–
positive (tumor cells . 1) and PD-L1–negative patients There are at least eight ongoing randomized phase II trials
(27.1% and 19.1%, respectively; P 5 .31).27 evaluating anti–PD-(L)1 ICIs plus SBRT in locoregionally
recurrent or metastatic HNSCC.51 To date, however,
Although there are no phase III studies showing the ef- evidence indicates that, while safe to deliver concur-
fectiveness of anti–PD-1 immunotherapies in patients with rently, there is no role for SBRT either in inducing an
recurrent metastatic NPC who have progressed on abscopal response or otherwise augmenting the effects of
platinum-based chemotherapy, phase II studies suggest a immunotherapy in patients with recurrent or metastatic
clinical benefit with lower toxicity rates when compared to HNSCC.
chemotherapy.48,49
Clinical Question 6
Clinical Question 5
What is the role of immunotherapy for rare head and neck
What is the effect of radiation therapy in combination with cancers?
anti–PD-(L)1 immunotherapy compared to immunotherapy
alone for the treatment of locoregionally recurrent or oli- Recommendation 6.1. Pembrolizumab may be offered to
gometastatic HNSCC? patients with TMB-high recurrent or metastatic rare head
Journal of Clinical Oncology 1139
Downloaded from ascopubs.org by 125.17.8.42 on February 19, 2023 from 125.017.008.042
Copyright © 2023 American Society of Clinical Oncology. All rights reserved.
Yilmaz et al
and neck cancers (Type: Evidence based, benefits out- immune-related AEs. Therefore, pembrolizumab may be
weigh harms; Evidence quality: Moderate; Strength of offered to patients with recurrent or metastatic salivary
recommendation: Weak). gland cancers with PD-L1 expression $ 1%.
Literature review and clinical interpretation. TMB-high and See the algorithm in Figure 1 for biomarkers and recom-
microsatellite instability-high/deficient mismatch repair mendations by PD-L1 status, and the algorithm in Figure 2
(MSI-H/dMMR) have emerged as biomarkers for response for recommendations by subtype.
to pembrolizumab immunotherapy, irrespective of tissue
of origin. These biomarkers can be used to select patients PATIENT AND CLINICIAN COMMUNICATION
with rare head and neck cancers for immunotherapy. The As the advancement of science continues, controversies
phase II study, KEYNOTE-158, evaluated the response of around old and new practices continue to arise. Improving
patients with advanced, incurable solid tumors to pem- outcomes requires careful consideration in the continuous
brolizumab.33 Twenty-seven tumor types were enrolled, balance of literature. With the advancement of science and
including salivary gland carcinomas. In a prespecified technology, additional screening techniques are available
analysis, the association between response to pem- to better treat patients.
brolizumab and tissue TMB (tTMB) was assessed. Re-
Strategies to manage cancer in the head and neck, oral
sponse rates were higher in tTMB-high group (defined
cavity, and oropharynx naturally vary according to a sur-
as $ 10 mutations per megabase) when compared to
geon’s experience and the availability of different tech-
non-tTMB high group (29% v 6%, respectively). Based on
nologies. As surgical techniques and the understanding of
these data, pembrolizumab is US Food and Drug
disease pathogenesis improve, patients are given even
Administration–approved and may be offered as systemic
more options. However, head and neck cancer clinicians
treatment for TMB-high advanced rare head and neck
face a unique set of challenges, given the potential adverse
cancers (eg, salivary, sinonasal, etc).
impacts many of these treatments have on a patient’s
MSI-H due to deficient DNA mismatch repair (dMMR) leads quality of life. The clinician needs to consider how treat-
to increased somatic mutations and neoantigens, which ment might affect many areas for the patient, such as
increases response to anti–PD-1 inhibitors. KEYNOTE-158 speech, taste, saliva, chewing, swallowing, lymphatic
prospectively evaluated response to pembrolizumab in processes, nerve damage, teeth, facial bone structure, and
patients with noncolorectal MSI-H/dMMR cancers who physical appearance. The clinician needs to discuss these
progressed on or were intolerant to prior standard treat- potential impacts with the patient to balance the most ef-
ment.52 Response to pembrolizumab in MSI-H/dMMR fective treatment with the patient’s quality-of-life objectives.
cancers was 34.3% and OS was 23.5 months. However, Fortunately, many of the screening techniques described in
this cohort did not include any patients with head and neck the guidelines do not place additional burdens on patients.
cancers, and MSI-H alterations in head and neck cancer
By recommending which patients would most benefit from
have not been reported to date. Therefore, although
immunotherapy and biomarker testing, the Expert Panel
pembrolizumab is approved for any MSI-H tumors, further
hopes to give clearer guidelines to treating clinicians. The
studies are needed to establish the incidence of MSI-H al-
goal of these recommendations is so patients will receive
terations in rare head and neck cancers, and confirm the role
more specific, targeted treatments to manage their cancer,
of pembrolizumab in this setting.
resulting in higher success rates. This guideline does not
Recommendation 6.2. Pembrolizumab may be offered to seek to encompass all approaches, but serves as a helpful
patients with PD-L1–positive recurrent or metastatic sali- framework for discussions among the multidisciplinary
vary gland cancer (Type: Evidence based, benefits out- treatment team, the patient, and their families. These
weigh harms; Evidence quality: Moderate; Strength of discussions are critical for optimal modern care.
recommendation: Weak). ASCO has always believed that strong and clear commu-
Literature review and clinical interpretation. High-grade nication between physicians, patients, caregivers, and
salivary gland cancers have been found to express PD-L1, families is paramount for delivering the best quality care.
with 22.8% of samples expressing $ 1% PD-L1 in a ret- For recommendations and strategies to optimize patient-
rospective tissue analysis.37 PD-L1 expression was asso- clinician communication, see Patient-Clinician Communi-
ciated with poor disease-free survival in this study. The cation: American Society of Clinical Oncology Consensus
phase Ib study, KEYNOTE-028, evaluated the effectiveness Guideline.
of pembrolizumab in patients with advanced solid tumors
expressing 1% or greater PD-L1.34 Of 142 patients with HEALTH DISPARITIES
advanced salivary gland cancers who were screened, 33 Although ASCO clinical practice guidelines represent ex-
had PD-L1–positive tumors (23%), consistent with other pert recommendations on the best practices in disease
reports. Of the 26 patients treated with pembrolizumab, management to provide the highest level of cancer care, it is
three (12%) had a partial response without unexpected important to note that many patients have limited access to
1140 © 2022 by American Society of Clinical Oncology Volume 41, Issue 5
Downloaded from ascopubs.org by 125.17.8.42 on February 19, 2023 from 125.017.008.042
Copyright © 2023 American Society of Clinical Oncology. All rights reserved.
Immunotherapy and Biomarker Testing in Head and Neck Cancers
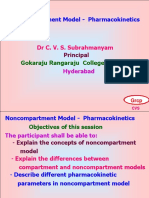
First-line therapy
Pembrolizumab monotherapy
PD-L1 CPS ≥ 1
(positive)
Pembrolizumab, platinum, and
5-FU
Pembrolizumab
Patients with any PD-L1 CPS
Patients with recurrent
PD-L1 IHC testing status and platinum-refractory
or metastatic HNSCC
recurrent or metastatic HNSCC
Nivolumab
Pembrolizumab, platinum, and
PD-L1 CPS < 1
5-FU
TMB testing if CPS is
Intepret as high; correlating
not available or in
TMB ≥ 10 with a clinical benefit to
patients with rare
PD-1 inhibitors
tumors
FIG 1. Algorithm for biomarkers and recommendations by PD-L1 status. 5-FU, fluorouracil; CPS, combined positive score; HNSCC, head and
neck squamous cell carcinoma; IHC, immunohistochemistry; PD-1, programmed cell death protein-1; PD-L1, programmed death ligand-1;
TMB, tumor mutational burden.
Toripalimab, camrelizumab, or
Nasopharyngeal
tislelizumab, with gemcitabine
cancer
and cisplatin as first-line therapy
Pembrolizumab or nivolumab
Patients with recurrent
with gemcitabine and cisplatin if
or metastatic head and
toripalimab, camrelizumab, or
neck cancer
tislelizumab not available
Salivary gland cancer PD-L1–positive
Pembrolizumab
Rare head and neck
cancers TMB-high
Salivary gland cancer
Radiation therapy is safe to give concurrently with immunotherapy for the
Oligometastatic
purpose of palliation or local control, but should not be given to enhance
HNSCC
response to immunotherapy outside of a clinical trial
FIG 2. Recommendations by cancer subtype. HNSCC, head and neck squamous cell carcinoma; PD-L1, programmed death ligand-1; TMB, tumor
mutational burden.
Journal of Clinical Oncology 1141
Downloaded from ascopubs.org by 125.17.8.42 on February 19, 2023 from 125.017.008.042
Copyright © 2023 American Society of Clinical Oncology. All rights reserved.
Yilmaz et al
medical care or receive fragmented care. Factors such as recommended care. This may mean that some or all of the
race and ethnicity, age, socioeconomic status, sexual ori- recommended care options are modified or not applied, as
entation and gender identity, geographic location, and determined by best practice in consideration of any MCC.
insurance access are known to impact cancer care out-
comes.53 Racial and ethnic disparities in health care COST IMPLICATIONS
contribute significantly to this problem in the United States.
Increasingly, individuals with cancer are required to pay a
Patients with cancer who are members of racial or ethnic
larger proportion of their treatment costs through deduct-
minorities suffer disproportionately from comorbidities,
ibles and coinsurance.58,59 Higher patient out-of-pocket
experience more substantial obstacles to receiving care,
costs have been shown to be a barrier to initiating and
are more likely to be uninsured, and are at greater risk of
adhering to recommended cancer treatments.60,61
receiving fragmented care or poor-quality care than other
Americans.54-57 Many other patients lack access to care Discussion of cost can be an important part of shared
because of their geographic location and distance from decision making.62 Clinicians should discuss with patients
appropriate treatment facilities. Lack of access to care the use of less expensive alternatives when it is practical
increases timelines to diagnoses and often results in an and feasible for treatment of the patient’s disease and there
advanced disease state at the time of diagnosis. Awareness are two or more treatment options that are comparable in
of these disparities in access to care should be considered terms of benefits and harms.62
in the context of this clinical practice guideline, and health Patient out-of-pocket costs may vary depending on in-
care providers should strive to deliver the highest level of surance coverage. Coverage may originate in the medical or
cancer care to these vulnerable populations. Additionally, pharmacy benefit, which may have different cost-sharing
stakeholders should work toward achieving health equity by arrangements. Patients should be aware that different
ensuring equitable access to both high-quality cancer care products may be preferred or covered by their particular
and research and addressing the structural barriers that insurance plan. Even with the same insurance plan, the
preserve health inequities.53 price may vary between different pharmacies. When dis-
cussing financial issues and concerns, patients should be
MULTIPLE CHRONIC CONDITIONS made aware of any financial counseling services available
Creating evidence-based recommendations to inform to address this complex and heterogeneous landscape.62
treatment of patients with additional chronic conditions, a As part of the guideline development process, ASCO may
situation in which the patient may have two or more such opt to search the literature for published cost-
conditions—referred to as multiple chronic conditions effectiveness analyses that might inform the relative
(MCCs)—is challenging. Patients with MCC are a complex value of available treatment options. Excluded from
and heterogeneous population, making it difficult to ac- consideration are cost-effective analyses that lack con-
count for all of the possible permutations to develop specific temporary cost data; agents that are not currently avail-
recommendations for care. In addition, the best available able in either the United States or Canada; or are industry-
evidence for treating index conditions, such as cancer, is sponsored. Three cost-effectiveness analyses were
often from clinical trials whose study selection criteria may identified to inform the topic.63-65 Each analysis similarly
exclude these patients to avoid potential interaction effects dealt with the particular case of nivolumab monotherapy
or confounding of results associated with MCC. As a result, for recurrent or metastatic HNSCC. Both Haddad et al63
the reliability of outcome data from these studies may be and Ward et al65 found that nivolumab was cost-effective
limited, thereby creating constraints for expert groups to up to a willingness-to-pay threshold of $150,000 in US
make recommendations for care in this heterogeneous dollars (USD) per quality-adjusted life-year (QALY);63
patient population. however, Tringale et al64 concluded nivolumab was not
As many patients for whom guideline recommendations cost-effective if a threshold of $100,000 (USD) per
apply present with MCC, any treatment plan needs to take quality-adjusted life-year was used.
into account the complexity and uncertainty created by the
presence of MCC and highlights the importance of shared EXTERNAL REVIEW AND OPEN COMMENT
decision making regarding guideline use and imple- The draft recommendations were released to the public for
mentation. Therefore, in consideration of recommended open comment from June 6 to 21, 2022. Response cat-
care for the target index condition, clinicians should review egories of “Agree as written,” “Agree with suggested
all other chronic conditions present in the patient and take modifications” and “Disagree. See comments” were cap-
those conditions into account when formulating the treat- tured for every proposed recommendation with 53 written
ment and follow-up plan. comments received. A total of 97% of the 29 respondents
In light of these considerations, practice guidelines should either agreed or agreed with slight modifications to the
provide information on how to apply the recommendations recommendations and 3% of the respondents disagreed.
for patients with MCC, perhaps as a qualifying statement for Expert Panel members reviewed comments from all
1142 © 2022 by American Society of Clinical Oncology Volume 41, Issue 5
Downloaded from ascopubs.org by 125.17.8.42 on February 19, 2023 from 125.017.008.042
Copyright © 2023 American Society of Clinical Oncology. All rights reserved.
Immunotherapy and Biomarker Testing in Head and Neck Cancers
sources and determined whether to maintain original draft GENDER-INCLUSIVE LANGUAGE
recommendations, revise with minor language changes, or ASCO is committed to promoting the health and well-being of
consider major recommendation revisions. All changes individuals regardless of sexual orientation or gender iden-
were incorporated prior to ASCO Evidence Based Medicine tity.82 Transgender and nonbinary people, in particular, may
Committee review and approval. face multiple barriers to oncology care including stigmatiza-
tion, invisibility, and exclusiveness. One-way exclusiveness or
GUIDELINE IMPLEMENTATION lack of accessibility may be communicated through gendered
ASCO guidelines are developed for implementation across language that makes presumptive links between gender and
health settings. Each ASCO guideline includes a member anatomy.83-86 With the acknowledgment that ASCO guidelines
from ASCO’s Practice Guideline Implementation Network may impact the language used in clinical and research set-
(PGIN) on the panel. The additional role of this PGIN tings, ASCO is committed to creating gender-inclusive
representative on the guideline panel is to assess the guidelines. For this reason, guideline authors use gender-
suitability of the recommendations to implementation in the inclusive language whenever possible throughout the
community setting, but also to identify any other barrier to guidelines. In instances in which the guideline draws upon
implementation a reader should be aware of. Barriers to data based on gendered research (eg, studies regarding
implementation include the need to increase awareness of women with ovarian cancer), the guideline authors describe
the guideline recommendations among frontline practi- the characteristics and results of the research as reported.
tioners and survivors of cancer and caregivers, and also to ASCO believes that cancer clinical trials are vital to inform
provide adequate services in the face of limited resources. medical decisions and improve cancer care, and that all
The guideline Bottom Line Box was designed to facilitate patients should have the opportunity to participate.
implementation of recommendations. This guideline will be
distributed widely through the ASCO PGIN. ASCO guide- ADDITIONAL RESOURCES
lines are posted on the ASCO website and most often
published in the Journal of Clinical Oncology. More information, including a supplement with additional
evidence tables, slide sets, and clinical tools and resources,
LIMITATIONS OF THE RESEARCH AND FUTURE RESEARCH is available at www.asco.org/head-neck-cancer-guidelines.
Patient information is available at www.cancer.net.
Routine use of immunotherapy in HNSCC is currently limited
to the recurrent or metastatic setting. The role of ICIs in
locoregionally advanced disease is not yet established, with
several randomized trials finding no benefit to the addition of RELATED ASCO GUIDELINES
ICIs in combination with definitive (chemo)radiotherapy.66,67
• Integration of Palliative Care Into Standard On-
The phase III JAVELIN trial tested the addition of the PD-L1 cology Care75 (http://ascopubs.org/doi/10.1200/
inhibitor avelumab to standard cisplatin and radiation JCO.2016.70.1474).
therapy for definitive treatment of locally advanced • Patient-Clinician Communication76 (http://
HNSCC.67 This trial found no benefit to the addition of ascopubs.org/doi/10.1200/JCO.2017.75.2311).
avelumab to standard chemoradiation. However, this trial • Management of the Neck in Squamous Cell
was not restricted on the basis of PD-L1 status, and the Carcinoma of the Oral Cavity and Oropharynx77
optimal sequencing of (chemo)radiation with immunother- (http://ascopubs.org/doi/10.1200/
apy is not yet defined. A phase II trial of neoadjuvant and JCO.18.01921).
adjuvant pembrolizumab in resectable locally advanced • Human Papillomavirus Testing in Head and
HNSCC patients indicated that pathologic response could Neck Carcinomas78 (http://ascopubs.org/doi/
serve as a potential marker for subsequent response to ICIs 10.1200/JCO.18.00684).
and improved disease-free survival.68 Multiple other recently • Diagnosis and Management of Squamous Cell
completed and ongoing randomized trials are evaluating the Carcinoma of Unknown Primary in the Head
role of immunotherapy in combination with definitive or and Neck79 (http://ascopubs.org/doi/10.1200/
adjuvant (chemo)radiation. These include KEYNOTE-412, JCO.20.00275).
GORTEC-REACH, GORTEC 2015-01, NRG HN004 (Clin- • Chemotherapy in Combination with Radiotherapy
icalTrials.gov identifier: NCT03258554), NRG HN005 for Definitive-Intent Treatment of Stage II-IVA Na-
(ClinicalTrials.gov identifier: NCT03952585), Imvoke010, sopharyngeal Carcinoma80 (http://ascopubs.org/
RTOG 1216, ECOG-ACRIN EA3161 (ClinicalTrials.gov doi/10.1200/JCO.20.03237).
identifier: NCT03811015), KEYCHAIN (ClinicalTrials.gov • Management of Salivary Gland Malignancy81
identifier: NCT03383094), and CCTG HN.9.66,69-74 To date, (http://ascopubs.org/doi/10.1200/
however, the role of immunotherapy, if any, in the treatment JCO.21.00449).
of previously untreated locoregionally advanced HNSCC
remains to be determined.
Journal of Clinical Oncology 1143
Downloaded from ascopubs.org by 125.17.8.42 on February 19, 2023 from 125.017.008.042
Copyright © 2023 American Society of Clinical Oncology. All rights reserved.
Yilmaz et al
EDITOR’S NOTE
AFFILIATIONS
1 This American Society of Clinical Oncology (ASCO) Clinical Practice
Cleveland Clinic, Cleveland, OH
2
Guideline provides recommendations, with comprehensive review and
American Society of Clinical Oncology, Alexandria, VA
3
analyses of the relevant literature for each recommendation. Additional
George Washington University, Washington, DC
4 information, including a supplement with additional evidence tables,
The Center for Cancer and Blood Disorder, Southlake, TX
5
slide sets, clinical tools and resources, and links to patient information at
Kansas University Medical Center, Kansas City, KS
6
www.cancer.net, is available at www.asco.org/head-neck-cancer-
University of California San Francisco, San Francisco, CA
7 guidelines.
Patient Representative, Needham Heights, MA
8
Moffitt Cancer Center, Tampa, FL
9
Memorial Sloan Kettering Cancer Center, New York, NY EQUAL CONTRIBUTION
10
Ohio State University, Columbus, OH E.Y. and L.K.M were Expert Panel co-chairs.
11
Johns Hopkins Medicine, Baltimore, MD
12
Emory University, Atlanta, GA
13
AUTHORS’ DISCLOSURES OF POTENTIAL CONFLICTS OF
University of North Carolina, Chapel Hill, Chapel Hill, NC
14
Otago Medical School, University of Otago, Dunedin, New Zealand
INTEREST
15
Duke University, Durham, NC Disclosures provided by the authors are available with this article at DOI
16
University of Cincinnati, Cincinnati, OH https://doi.org/10.1200/JCO.22.02328.
17
University of California Los Angeles, Los Angeles, CA
18
University of California San Diego, La Jolla, CA AUTHOR CONTRIBUTIONS
Conception and design: All authors
CORRESPONDING AUTHOR Collection and assembly of data: All authors
American Society of Clinical Oncology, 2318 Mill Rd, Suite 800, Data analysis and interpretation: All authors
Alexandria, VA 22314; e-mail: guidelines@asco.org. Manuscript writing: All authors
Final approval of manuscript: All authors
Accountable for all aspects of the work: All authors
ACKNOWLEDGMENT
The Expert Panel wishes to thank Drs Rohan Garje and Shilpi Gupta, and
the Evidence Based Medicine Committee for their thoughtful reviews and
insightful comments on this guideline.
REFERENCES
1. Siegel RL, Miller KD, Fuchs HE, et al: Cancer statistics, 2022. CA: Cancer J Clin 72:7-33, 2022
2. Cohen EEW, Soulières D, Tourneau CL, et al: Pembrolizumab versus methotrexate, docetaxel, or cetuximab for recurrent or metastatic head-and-neck
squamous cell carcinoma (KEYNOTE-040): A randomised, open-label, phase 3 study. Lancet 393:156-167, 2019
3. Ferris RL, Blumenschein G, Fayette J, et al: Nivolumab for recurrent squamous-cell carcinoma of the head and neck. N Engl J Med 375:1856-1867, 2016
4. Burtness B, Harrington KJ, Greil R, et al: Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic
squamous cell carcinoma of the head and neck (KEYNOTE-048): A randomised, open-label, phase 3 study. Lancet 394:1915-1928, 2019
5. Chan TA, Yarchoan M, Jaffee E, et al: Development of tumor mutation burden as an immunotherapy biomarker: Utility for the oncology clinic. Ann Oncol 30:
44-56, 2019
6. Doroshow DB, Bhalla S, Beasley MB, et al: PD-L1 as a biomarker of response to immune-checkpoint inhibitors. Nat Rev Clin Oncol 18:345-362, 2021
7. Herbst RS, Giaccone G, de Marinis F, et al: Atezolizumab for first-line treatment of PD-L1-selected patients with NSCLC. N Engl J Med 383:1328-1339, 2020
8. Sharma P, Retz M, Siefker-Radtke A, et al: Nivolumab in metastatic urothelial carcinoma after platinum therapy (CheckMate 275): A multicentre, single-arm,
phase 2 trial. Lancet Oncol 18:312-322, 2017
9. Reck M, Rodriguez-Abreu D, Robinson AG, et al: Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N Engl J Med 375:
1823-1833, 2016
10. Shiffman RN, Michel G, Rosenfeld RM, et al: Building better guidelines with BRIDGE-Wiz: Development and evaluation of a software assistant to promote clarity,
transparency, and implementability. J Am Med Inform Assoc 19:94-101, 2012
11. Balshem H, Helfand M, Schünemann HJ, et al: GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol 64:401-406, 2011
12. Higgins JPT, Thomas J, Chandler J, et al (eds): Cochrane Handbook for Systematic Reviews of Interventions version 6.3 (updated February 2022). Cochrane,
2022. www.training.cochrane.org/handbook.
13. Huang Z, Zheng S, Ding S, et al: Prognostic role of programmed cell death ligand-1 expression in head and neck cancer treated with programmed cell death
protein-1/programmed cell death ligand-1 inhibitors: A meta-analysis based on clinical trials. J Cancer Res Ther 17:676-687, 2021
14. Emancipator K, Huang L, Aurora-Garg D, et al: Comparing programmed death ligand 1 scores for predicting pembrolizumab efficacy in head and neck cancer,
Mod Pathol 34:532-541, 2021
15. Mai HQ, Chen QY, Chen D, et al: Toripalimab or placebo plus chemotherapy as first-line treatment in advanced nasopharyngeal carcinoma: A multicenter
randomized phase 3 trial. Nat Med 27:1536-1543, 2021
16. Yang Y, Qu S, Li J, et al: Camrelizumab versus placebo in combination with gemcitabine and cisplatin as first-line treatment for recurrent or metastatic
nasopharyngeal carcinoma (CAPTAIN-1st): A multicentre, randomised, double-blind, phase 3 trial. Lancet Oncol 22:1162-1174, 2021
17. Ferris RL, Haddad R, Even C, et al: Durvalumab with or without tremelimumab in patients with recurrent or metastatic head and neck squamous cell carcinoma:
EAGLE, a randomized, open-label phase III study. Ann Oncol 31:942-950, 2020
18. Chan AT, Lee VHF, Hong RL, et al: 858O Results of KEYNOTE-122: A phase III study of pembrolizumab (pembro) monotherapy vs chemotherapy (chemo) for
platinum-pretreated, recurrent or metastatic (R/M) nasopharyngeal carcinoma (NPC). Ann Oncol 32:S7862021, 2021
1144 © 2022 by American Society of Clinical Oncology Volume 41, Issue 5
Downloaded from ascopubs.org by 125.17.8.42 on February 19, 2023 from 125.017.008.042
Copyright © 2023 American Society of Clinical Oncology. All rights reserved.
Immunotherapy and Biomarker Testing in Head and Neck Cancers
19. Kiyota N, Hasegawa Y, Takahashi S, et al: A randomized, open-label, phase III clinical trial of nivolumab vs. therapy of investigator’s choice in recurrent
squamous cell carcinoma of the head and neck: A subanalysis of Asian patients versus the global population in checkmate 141. Oral Oncol 73:138-146, 2017
20. Gillison ML, Blumenschein G, Fayette J, et al: CheckMate 141: 1-Year update and subgroup analysis of nivolumab as first-line therapy in patients with
recurrent/metastatic head and neck cancer. Oncologist 23:1079-1082, 2018
21. Ferris RL, Blumenschein G, Fayette J, et al: Nivolumab vs investigator’s choice in recurrent or metastatic squamous cell carcinoma of the head and neck: 2-Year
long-term survival update of CheckMate 141 with analyses by tumor PD-L1 expression. Oral Oncol 81:45-51, 2018
22. Ferris RL, Licitra L, Fayette J, et al: Nivolumab in patients with recurrent or metastatic squamous cell carcinoma of the head and neck: Efficacy and safety in
CheckMate 141 by prior cetuximab use. Clin Cancer Res 25:5221-5230, 2019
23. Haddad R, Concha-Benavente F, Blumenschein G, et al: Nivolumab treatment beyond RECIST-defined progression in recurrent or metastatic squamous cell
carcinoma of the head and neck in CheckMate 141: A subgroup analysis of a randomized phase 3 clinical trial. Cancer 125:3208-3218, 2019
24. Saba NF, Blumenschein G, Guigay J, et al: Nivolumab versus investigator’s choice in patients with recurrent or metastatic squamous cell carcinoma of the head
and neck: Efficacy and safety in CheckMate 141 by age. Oral Oncol 96:7-14, 2019
25. Yen CJ, Kiyota N, Hanai N, et al: Two-year follow-up of a randomized phase III clinical trial of nivolumab vs. the investigator’s choice of therapy in the Asian
population for recurrent or metastatic squamous cell carcinoma of the head and neck (CheckMate 141). Head Neck 42:2852-2862, 2020
26. Burtness B, Rischin D, Greil R, et al: Pembrolizumab alone or with chemotherapy for recurrent/metastatic head and neck squamous cell carcinoma in
KEYNOTE-048: Subgroup analysis by programmed death ligand-1 combined positive score. J Clin Oncol 40:2321-2332, 2022
27. Wang FH, Wei XL, Feng J, et al: Efficacy, safety, and correlative biomarkers of toripalimab in previously treated recurrent or metastatic nasopharyngeal
carcinoma: A phase II clinical trial (POLARIS-02). J Clin Oncol 39:704-712, 2021
28. Ma Y, Fang W, Zhang Y, et al: A phase I/II open-label study of nivolumab in previously treated advanced or recurrent nasopharyngeal carcinoma and other solid
tumors. Oncologist 24:891-e431, 2019
29. Segal NH, Ou SI, Balmanoukian A, et al: Safety and efficacy of durvalumab in patients with head and neck squamous cell carcinoma: results from a phase I/II
expansion cohort. Eur J Cancer 109:154-161, 2019
30. Siu LL, Even C, Mesı́a R, et al: Safety and efficacy of durvalumab with or without tremelimumab in patients with PD-L1-low/negative recurrent or metastatic
HNSCC: The phase 2 CONDOR randomized clinical trial. JAMA Oncol 5:195, 2019
31. Zandberg DP, Algazi AP, Jimeno A, et al: Durvalumab for recurrent or metastatic head and neck squamous cell carcinoma: Results from a single-arm, phase II
study in patients with $25% tumour cell PD-L1 expression who have progressed on platinum-based chemotherapy. Eur J Cancer 107:142-152, 2019
32. McBride S, Sherman E, Tsai CJ, et al: Randomized phase II trial of nivolumab with stereotactic body radiotherapy versus nivolumab alone in metastatic head
and neck squamous cell carcinoma. J Clin Oncol 39:30-37, 2021
33. Marabelle A, Fakih M, Lopez J, et al: Association of tumour mutational burden with outcomes in patients with advanced solid tumours treated with pem-
brolizumab: Prospective biomarker analysis of the multicohort, open-label, phase 2 KEYNOTE-158 study. Lancet Oncol 21:1353-1365, 2020
34. Cohen RB, Delord JP, Doi T, et al: Pembrolizumab for the treatment of advanced salivary gland carcinoma: Findings of the phase 1b KEYNOTE-028 study. Am J
Clin Oncol 41:1083-1088, 2018
35. Tada H, Takahashi H, Kawabata-Iwakawa R, et al: Molecular phenotypes of circulating tumor cells and efficacy of nivolumab treatment in patients with head
and neck squamous cell carcinoma. Sci Rep 10:21573, 2020
36. Samstein RM, Lee CH, Shoushtari AN, et al: Tumor mutational load predicts survival after immunotherapy across multiple cancer types. Nat Genet 51:202-206, 2019
37. Mukaigawa T, Hayashi R, Hashimoto K, et al: Programmed death ligand-1 expression is associated with poor disease free survival in salivary gland carcinomas.
J Surg Oncol 114:36-43, 2016
38. Wang J, Sun H, Zeng Q, et al: HPV-positive status associated with inflamed immune microenvironment and improved response to anti-PD-1 therapy in head
and neck squamous cell carcinoma. Sci Rep 9:13404, 2019
39. Zhang Y, Lin A, Li Y, et al: Age and mutations as predictors of the response to immunotherapy in head and neck squamous cell cancer. Front Cell Dev Biol 8:
608969, 2020
40. Haddad RI, Seiwert TY, Chow LQM, et al: Influence of tumor mutational burden, inflammatory gene expression profile, and PD-L1 expression on response to
pembrolizumab in head and neck squamous cell carcinoma. J Immunother Cancer 10:e003026, 2022
41. Bauml J, Seiwert TY, Pfister DG, et al: Pembrolizumab for platinum- and cetuximab-refractory head and neck cancer: Results from a single-arm, phase II study.
J Clin Oncol 35:1542-1549, 2017
42. Chow LQM, Haddad R, Gupta S, et al: Antitumor activity of pembrolizumab in biomarker-unselected patients with recurrent and/or metastatic head and neck
squamous cell carcinoma: Results from the phase Ib KEYNOTE-012 expansion cohort. J Clin Oncol 34:3838-3845, 2016
43. Botticelli A, Cirillo A, Strigari L, et al: Anti-PD-1 and anti-PD-L1 in head and neck cancer: A network meta-analysis, Front Immunol 12:705096, 2021
44. Sacco AG, Chen R, Worden FP, et al: Pembrolizumab plus cetuximab in patients with recurrent or metastatic head and neck squamous cell carcinoma: An
open-label, multi-arm, non-randomised, multicentre, phase 2 trial. Lancet Oncol 22:883-892, 2021
45. Chung CH, Bonomi M, Steuer CE, et al: Concurrent cetuximab and nivolumab as a second-line or beyond treatment of patients with recurrent and/or metastatic
head and neck squamous cell carcinoma: Results of phase I/II study. Cancers 13:1180, 2021
46. Chung CH, Li J, Steuer CE, et al: Phase II multi-institutional clinical trial result of concurrent cetuximab and nivolumab in recurrent and/or metastatic head and
neck squamous cell carcinoma. Clin Cancer Res 28:2329-2338, 2022
47. Zhang L, Yang Y, Pan J-j, et al: RATIONALE-309: Updated progression-free survival (PFS), PFS after next line of treatment, and overall survival from a phase 3
double-blind trial of tislelizumab versus placebo, plus chemotherapy, as first-line treatment for recurrent/metastatic nasopharyngeal cancer. J Clin Oncol 40,
2022 (suppl 36; abstr 384950)
48. Ma BBY, Lim WT, Goh BC, et al: Antitumor activity of nivolumab in recurrent and metastatic nasopharyngeal carcinoma: An international, multicenter study of
the Mayo clinic phase 2 consortium (NCI-9742). J Clin Oncol 36:1412-1418, 2018
49. Delord J-P, Hollebecque A, De Boer JP, et al: An open-label, multicohort, phase I/II study to evaluate nivolumab in patients with virus-associated tumors
(CheckMate 358): Efficacy and safety in recurrent or metastatic (R/M) nasopharyngeal carcinoma (NPC). J Clin Oncol 35, 2017 (suppl 15; abstr 6025)
50. Spaas M, Sundahl N, Rottey S, et al: OC-0625 immuno-radiotherapy in solid tumors: Preliminary results of the randomized phase 2 CHEERS trial. Radiother
Oncol 161:S490-S491, 2021
51. Qian JM, Schoenfeld JD: Radiotherapy and immunotherapy for head and neck cancer: Current evidence and challenges. Front Oncol 10:608772, 2020
52. Marabelle A, Le DT, Ascierto PA, et al: Efficacy of pembrolizumab in patients with noncolorectal high microsatellite instability/mismatch repair-deficient cancer:
Results from the phase II KEYNOTE-158 study. J Clin Oncol 38:1-10, 2020
53. Patel MI, Lopez AM, Blackstock W, et al: Cancer disparities and health equity: A policy statement from the American Society of Clinical Oncology. J Clin Oncol
38:3439-3448, 2020
Journal of Clinical Oncology 1145
Downloaded from ascopubs.org by 125.17.8.42 on February 19, 2023 from 125.017.008.042
Copyright © 2023 American Society of Clinical Oncology. All rights reserved.
Yilmaz et al
54. Howlader N, Noone AM, Krapcho M, et al: SEER Cancer Statistics Review, 1975-2013. Bethesda, MD, National Cancer Institute, 2016. http://seer.cancer.gov/
csr/1975_2013/
55. American Cancer Society: Cancer Facts & Figures 2020. Atlanta, GA, American Cancer Society, 2020
56. US Cancer Statistics Working Group: United States Cancer Statistics: 1999–2012 Incidence and Mortality Web-Based Report. Atlanta, GA, US Department of
Health and Human Services, Centers for Disease Control and Prevention and National Cancer Institute, 2015. www.cdc.gov/uscs
57. Mead H, Cartwright-Smith L, Jones K, et al: Racial and Ethnic Disparities in U.S. Health Care: A Chartbook. New York, NY, The Commonwealth Fund, 2008
58. Schnipper LE, Davidson NE, Wollins DS, et al: Updating the American Society of Clinical Oncology value framework: Revisions and reflections in response to
comments received. J Clin Oncol 34:2925-2934, 2016
59. Schnipper LE, Davidson NE, Wollins DS, et al: American Society of Clinical Oncology statement: A conceptual framework to assess the value of cancer treatment
options. J Clin Oncol 33:2563-2577, 2015
60. Streeter SB, Schwartzberg L, Husain N, et al: Patient and plan characteristics affecting abandonment of oral oncolytic prescriptions. JCO Oncol Pract 7:
46s-51s, 2011
61. Dusetzina SB, Winn AN, Abel GA, et al: Cost sharing and adherence to tyrosine kinase inhibitors for patients with chronic myeloid leukemia. J Clin Oncol 32:
306-311, 2014
62. Meropol NJ, Schrag D, Smith TJ, et al: American Society of Clinical Oncology guidance statement: The cost of cancer care. J Clin Oncol 27:3868-3874, 2009
63. Haddad R, Cohen EEW, Venkatachalam M, et al: Cost-effectiveness analysis of nivolumab for the treatment of squamous cell carcinoma of the head and neck in
the United States. J Med Econ 23:442-447, 2020
64. Tringale KR, Carroll KT, Zakeri K, et al: Cost-effectiveness analysis of nivolumab for treatment of platinum-resistant recurrent or metastatic squamous cell
carcinoma of the head and neck (ed 5). J Natl Cancer Inst 110:479-485, 2018
65. Ward MC, Shah C, Adelstein DJ, et al: Cost-effectiveness of nivolumab for recurrent or metastatic head and neck cancer. Oral Oncol 74, 49, 55, 2017
66. Bourhis J, Tao Y, Sun X, et al: LBA35 Avelumab-cetuximab-radiotherapy versus standards of care in patients with locally advanced squamous cell carcinoma of
head and neck (LA-SCCHN): Randomized phase III GORTEC-REACH trial. Ann Oncol 32:S1310, 2021
67. Lee NY, Ferris RL, Psyrri A, et al: Avelumab plus standard-of-care chemoradiotherapy versus chemoradiotherapy alone in patients with locally advanced
squamous cell carcinoma of the head and neck: A randomised, double-blind, placebo-controlled, multicentre, phase 3 trial. Lancet Oncol 22:450-462, 2021
68. Wise-Draper TM, Gulati S, Palackdharry S, et al: Phase II clinical trial of neoadjuvant and adjuvant pembrolizumab in resectable local-regionally advanced head
and neck squamous cell carcinoma. Clin Cancer Res 28:1345-1352, 2022
69. Machiels JP, Tao Y, Burtness B, et al: Pembrolizumab given concomitantly with chemoradiation and as maintenance therapy for locally advanced head and
neck squamous cell carcinoma: KEYNOTE-412. Future Oncol 16:1235-1243, 2020
70. Bourhis J, Sire C, Tao Y, et al: LBA38 Pembrolizumab versus cetuximab, concomitant with radiotherapy (RT) in locally advanced head and neck squamous cell
carcinoma (LA-HNSCC): Results of the GORTEC 2015-01;PembroRad; randomized trial. Ann Oncol 31:S1168, 2020
71. Haddad R, Wong DJ, Guo Y, et al: IMvoke010: Randomized phase III study of atezolizumab (atezo) as adjuvant monotherapy after definitive therapy of
squamous cell carcinoma of the head and neck (SCCHN). Ann Oncol 29:viii397, 2018
72. Mell LK, Torres-Saavedra PA, Wong SJ, et al: Safety of radiotherapy with concurrent and adjuvant MEDI4736 (durvalumab) in patients with locoregionally
advanced head and neck cancer with a contraindication to cisplatin: NRG-HN004. J Clin Oncol 37, 2019 (suppl 15; abstr 6065)
73. Spreafico A, Sultanem K, Chen B, et al: A randomized phase II study of cisplatin plus radiotherapy versus durvalumab plus radiotherapy followed by adjuvant
durvalumab versus durvalumab plus radiotherapy followed by adjuvant tremelimumab and durvalumab in intermediate risk, HPV-positive, locoregionally
advanced oropharyngeal squamous cell cancer (LA-OSCC) (Canadian Cancer Trials Group HN.9). Ann Oncol 29:viii399, 2018
74. Sacco AG, Sharabi A, Jing Z, et al: Radiotherapy with concurrent and adjuvant pembrolizumab in patients with P16-positive locoregionally advanced head and
neck cancer: KEYCHAIN trial lead-in results. Int J Radiat Oncol Biol Phys 105:E363-E364, 2019
75. Ferrell BR, Temel JS, Temin S, et al: Integration of palliative care into standard oncology care: American Society of Clinical Oncology clinical practice guideline
update. J Clin Oncol 35:96-112, 2017
76. Gilligan T, Coyle N, Frankel RM, et al: Patient-clinician communication: American Society of Clinical Oncology consensus guideline. J Clin Oncol 35:3618-3632, 2017
77. Koyfman SA, Ismaila N, Crook D, et al: Management of the neck in squamous cell carcinoma of the oral cavity and oropharynx: ASCO clinical practice guideline.
J Clin Oncol 37:1753-1774, 2019
78. Fakhry C, Lacchetti C, Rooper LM, et al: Human papillomavirus testing in head and neck carcinomas: ASCO clinical practice guideline endorsement of the
College of American Pathologists guideline. J Clin Oncol 36:3152-3161, 2018
79. Maghami E, Ismaila N, Alvarez A, et al: Diagnosis and management of squamous cell carcinoma of unknown primary in the head and neck: ASCO guideline.
J Clin Oncol 38:2570-2596, 2020
80. Chen YP, Ismaila N, Chua MLK, et al: Chemotherapy in combination with radiotherapy for definitive-intent treatment of stage II-IVA nasopharyngeal carcinoma:
CSCO and ASCO guideline. J Clin Oncol 39:840-859, 2021
81. Geiger JL, Ismaila N, Beadle B, et al: Management of salivary gland malignancy: ASCO guideline. J Clin Oncol 39:1909-1941, 2021
82. Griggs J, Maingi S, Blinder V, et al: American Society of Clinical Oncology position statement: Strategies for reducing cancer health disparities among sexual and
gender minority populations. J Clin Oncol 35:2203-2208, 2017
83. Alpert AB, Gampa V, Lytle MC, et al: I’m not putting on that floral gown: Enforcement and resistance of gender expectations for transgender people with cancer,
Patient Educ Couns 104:2552-2558, 2021.
84. Alpert AB, Manzano C, Ruddick R: Degendering oncologic care and other recommendations to eliminate barriers to care for transgender people with cancer.
ASCO Daily News. January 19, 2021. https://dailynews.ascopubs.org/do/10.1200/ADN.21.200433/full/
85. National Center for Transgender Equality. Understanding Transgender People: The Basics. https://transequality.org/issues/resources/understanding-
transgender-people-the-basics
86. UCSF Transgender Care & Treatment Guidelines. Terminology & Definitions. https://transcare.ucsf.edu/guidelines/terminology
n n n
1146 © 2022 by American Society of Clinical Oncology Volume 41, Issue 5
Downloaded from ascopubs.org by 125.17.8.42 on February 19, 2023 from 125.017.008.042
Copyright © 2023 American Society of Clinical Oncology. All rights reserved.
Immunotherapy and Biomarker Testing in Head and Neck Cancers
AUTHORS’ DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST
Immunotherapy and Biomarker Testing in Recurrent and Metastatic Head and Neck Cancers: ASCO Guideline
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted.
Relationships are self-held unless noted. I 5 Immediate Family Member, Inst 5 My Institution. Relationships may not relate to the subject matter of this manuscript.
For more information about ASCO’s conflict of interest policy, please refer to www.asco.org/rwc or ascopubs.org/jco/authors/author-center.
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (Open Payments).
Emrullah Yilmaz Nabil F. Saba
Consulting or Advisory Role: Astellas Pharma Honoraria: Merck, EMD Serono, AstraZeneca, ReachMD, Vaccinex, Eisai,
Novartis, Exelixis, GlaxoSmithKline, Inovio Pharmaceuticals, American Journal
Nofisat Ismaila
of Managed Care.
Employment: GlaxoSmithKline
Consulting or Advisory Role: Mirati Therapeutics
Stock and Other Ownership Interests: GlaxoSmithKline
Research Funding: Bristol Myers Squibb, Exelixis
Julie E. Bauman Patents, Royalties, Other Intellectual Property: UpToDate chapter writing and
Consulting or Advisory Role: BlueDot, Exelixis editing, Springer textbook Royalty
Research Funding: Bristol Myers Squibb (Inst), AVEO (Inst), Novartis (Inst), Travel, Accommodations, Expenses: Merck
Celldex (Inst), Moderna Therapeutics (Inst), Lilly (Inst), AstraZeneca (Inst), CUE
Siddharth Sheth
Biopharma (Inst)
Honoraria: Naveris, Medscape
Raetasha Dabney Speakers’ Bureau: Exelixis
Employment: Magellan Health Research Funding: AstraZeneca/MedImmune, Merck (Inst), AstraZeneca (Inst),
Speakers’ Bureau: Myriad Genetics Inovio Pharmaceuticals (Inst)
Gregory Gan Travel, Accommodations, Expenses: AstraZeneca/MedImmune
Honoraria: AstraZeneca Trisha Michel Wise-Draper
Consulting or Advisory Role: IDEO Oncology Stock and Other Ownership Interests: High Enroll
Research Funding: Aclaris Therapeutics Honoraria: Physicians’ Education Resource
Patents, Royalties, Other Intellectual Property: US Patent Application #: Consulting or Advisory Role: Shattuck Labs, Rakuten Medical, Exicure, Merck,
15/506,421 Title: Inhibition of MK2 in Treatment of Cancer. Coinventor: Gregory Caris Life Sciences
Gan, Ellen Beswick Patent filed on Dec 2015 Research Funding: Merck, AstraZeneca/MedImmune, Bristol Myers Squibb,
GlaxoSmithKline, Caris Life Sciences, Janssen Oncology
Richard Jordan
Stock and Other Ownership Interests: Genomic Health Travel, Accommodations, Expenses: Merck, Bristol Myers Squibb, Bexion,
AstraZeneca/MedImmune, Caris Life Sciences, Lilly, Tesaro
Research Funding: Deciper Bio (Inst)
Kedar Kirtane Deborah Wong
Consulting or Advisory Role: Bristol Myers Squibb, Genentech/Roche,
Stock and Other Ownership Interests: Oncternal Therapeutics, Seattle Genetics,
Macrogenics, Immunomedics, Myovant Sciences, Veru, Agenus Sanofi/Aventis, Blueprint Medicines, Regeneron
Consulting or Advisory Role: MyCareGorithm Research Funding: Merck Serono (Inst), Merck Sharp & Dohme (Inst), ARMO
BioSciences (Inst), AstraZeneca/MedImmune (Inst), Kura Oncology (Inst),
Sean Matthew McBride Regeneron (Inst), Genentech/Roche (Inst), Bristol Myers Squibb (Inst), FSTAR
Consulting or Advisory Role: Janssen, AstraZeneca (Inst), Pfizer (Inst), Astellas Pharma (Inst), Enzychem Lifesciences (Inst), Lilly,
Research Funding: Genentech, AstraZeneca Elevar Therapeutics (Inst), TopAlliance Biosciences Inc (Inst), Checkmate
Matthew O. Old Pharmaceuticals (Inst), Bicara Therapeutics (Inst), Gilead Sciences (Inst)
Honoraria: KLS Martin Loren K. Mell
Travel, Accommodations, Expenses: KLS Martin Consulting or Advisory Role: Cel-Sci
Research Funding: Merck, AstraZeneca
Open Payments Link: https://openpaymentsdata.cms.gov/physician/286651
No other potential conflicts of interest were reported.
Journal of Clinical Oncology
Downloaded from ascopubs.org by 125.17.8.42 on February 19, 2023 from 125.017.008.042
Copyright © 2023 American Society of Clinical Oncology. All rights reserved.
Yilmaz et al
APPENDIX
TABLE A1. Recommendation Rating Definitions
Term Definitions
Quality of evidence
High We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of
the effect, but there is a possibility that it is substantially different.
Low Our confidence in the effect estimate is limited: The true effect may be substantially different from the
estimate of the effect.
Very low We have very little confidence in the effect estimate: The true effect is likely to be substantially different
from the estimate of effect.
Strength of recommendation
Strong In recommendations for an intervention, the desirable effects of an intervention outweigh its
undesirable effects.
In recommendations against an intervention, the undesirable effects of an intervention outweigh its
desirable effects.
All or almost all informed people would make the recommended choice for or against an intervention.
Weak In recommendations for an intervention, the desirable effects probably outweigh the undesirable
effects, but appreciable uncertainty exists.
In recommendations against an intervention, the undesirable effects probably outweigh the desirable
effects, but appreciable uncertainty exists.
Most informed people would choose the recommended course of action, but a substantial number
would not.
TABLE A2. Immunotherapy and Biomarker Testing in Recurrent and Metastatic Head and Neck Cancers Guideline Expert Panel Membership
Name Affiliation Role or Area of Expertise
Emrullah Yilmaz, MD, PhD Cleveland Clinic, Cleveland, OH Medical Oncology
(co-chair)
Loren K. Mell, MD (co-chair) University of California San Diego, La Jolla, CA Radiation Oncology
Julie Bauman, MPH, MD George Washington University, Washington, DC Medical Oncology
Raetasha Dabney, MD The Center for Cancer and Blood Disorder, Southlake, TX PGIN Representation
Gregory Gan, MD, PhD Kansas University Medical Center, Kansas City, KS Radiation Oncology
Richard Jordan, DDS, PhD University of California San Francisco, San Francisco, CA Pathologist
Marnie Kaufman Needham Heights, MA Patient Representation
Kedar Kirtane, MD Moffitt Cancer Center, Tampa, FL Medical Oncology
Sean Matthew McBride, MD, MPH Memorial Sloan Kettering Cancer Center, New York, NY Radiation Oncology
Matthew O. Old, MD Ohio State University, Columbus, OH Surgical Oncology
Lisa Rooper, MD Johns Hopkins Medicine, Baltimore, MD Pathologist
Nabil F. Saba, FACP, MD Emory University, Atlanta, GA Medical Oncology
Siddharth Sheth, DO, MPH University of North Carolina, Chapel Hill, NC Medical Oncology
Rathan M. Subramaniam, Otaga Medical School, University of Otago, Dunedin, NZ Radiologist and Nuclear Medicine
MD, PhD, MPH, MBA Duke University, Durham, NC Physician
Trisha Michel Wise-Draper, University of Cincinnati, Cincinnati, OH Medical Oncology
MD, PhD
Deborah Wong, MD, PhD University of California Los Angeles, Los Angeles, CA Medical Oncology
Nofisat Ismaila, MD American Society of Clinical Oncology, Alexandria, VA ASCO Practice Guideline Staff
(Health Research Methods)
© 2022 by American Society of Clinical Oncology Volume 41, Issue 5
Downloaded from ascopubs.org by 125.17.8.42 on February 19, 2023 from 125.017.008.042
Copyright © 2023 American Society of Clinical Oncology. All rights reserved.
You might also like
- Thoughts and Mood WorksheetsDocument12 pagesThoughts and Mood Worksheetssadepressionscreen95% (44)
- BLUEBIRD (Some Part)Document17 pagesBLUEBIRD (Some Part)Mushtaq RahiNo ratings yet
- Aloe Vera Soothing GelDocument8 pagesAloe Vera Soothing GelReymar RodriguezNo ratings yet
- Subacute Combined Degeneration of Spinal CordDocument4 pagesSubacute Combined Degeneration of Spinal CordPriyanka MathurNo ratings yet
- Toilet TrainingDocument2 pagesToilet Trainingpaulinejones37No ratings yet
- Ayurveda Massage Therapist & Yoga Instructor ResumeDocument2 pagesAyurveda Massage Therapist & Yoga Instructor ResumePartheebanNo ratings yet
- Nursing Intervention Plan for Fracture PatientDocument2 pagesNursing Intervention Plan for Fracture PatientAce Dioso TubascoNo ratings yet
- Pain Management PDFDocument38 pagesPain Management PDFYulia Fransisca PurbaNo ratings yet
- NCP For SchizoDocument5 pagesNCP For SchizoRichelene Mae Canja100% (2)
- Drug StudyDocument10 pagesDrug StudyRye IbarraNo ratings yet
- Published Applied Kinesiology TextsDocument10 pagesPublished Applied Kinesiology TextsVíctor Muñoz López100% (1)
- Schneider Et Al 2021 Management of Immune Related Adverse Events in Patients Treated With Immune Checkpoint InhibitorDocument64 pagesSchneider Et Al 2021 Management of Immune Related Adverse Events in Patients Treated With Immune Checkpoint InhibitorAlexandra MoraesNo ratings yet
- Biomarkers in Precision Cancer ImmunotherapyDocument17 pagesBiomarkers in Precision Cancer ImmunotherapyYachao LiuNo ratings yet
- Prediction Model For Shortterm Mortality After Palliative Therapy For Patients Having Advanced Cancer - A Cohort Study From Routine Electronic Medical DataDocument10 pagesPrediction Model For Shortterm Mortality After Palliative Therapy For Patients Having Advanced Cancer - A Cohort Study From Routine Electronic Medical DataHollis LukNo ratings yet
- Barsanti-Innes The Oncologist - 2016Document8 pagesBarsanti-Innes The Oncologist - 2016Liz BethNo ratings yet
- Immunotherapy in Non Small Cell Lung Cancer Facts and HopeDocument22 pagesImmunotherapy in Non Small Cell Lung Cancer Facts and HopeasdffdsaNo ratings yet
- CPCNP MTXDocument9 pagesCPCNP MTXMary CogolloNo ratings yet
- Pembrolizumab For Previously TreatedDocument11 pagesPembrolizumab For Previously Treatedalex.losadaNo ratings yet
- ASCO Antiemetic Guidelines Update Aug 2020Document18 pagesASCO Antiemetic Guidelines Update Aug 2020catalina roa zagalNo ratings yet
- High-Risk Non-Small Cell Lung Cancer Treated With Active Scanning Proton Beam Radiation Therapy and ImmunotherapyDocument9 pagesHigh-Risk Non-Small Cell Lung Cancer Treated With Active Scanning Proton Beam Radiation Therapy and ImmunotherapyRaul Matute MartinNo ratings yet
- Validation of The Meet URO Score in Patients WithDocument9 pagesValidation of The Meet URO Score in Patients Withveaceslav coscodanNo ratings yet
- NSCLCMADocument9 pagesNSCLCMAapi-26302710No ratings yet
- (583950958) Journal Leucopenia Treatment Effiicacy NPCDocument8 pages(583950958) Journal Leucopenia Treatment Effiicacy NPCDaniel HoseaNo ratings yet
- Head NeckDocument8 pagesHead NeckerandolphsavageNo ratings yet
- Bu Wiwin 1Document19 pagesBu Wiwin 1Dinny Fitriani FullNo ratings yet
- MainDocument8 pagesMainIoana CucuNo ratings yet
- Diagnosis and Management of Squamous Cell Carcinoma of Unknown Primary in The Head and Neck - ASCO GuidelineDocument29 pagesDiagnosis and Management of Squamous Cell Carcinoma of Unknown Primary in The Head and Neck - ASCO GuidelineFabian Camelo OtorrinoNo ratings yet
- Antiemetics: ASCO Guideline Update: PurposeDocument18 pagesAntiemetics: ASCO Guideline Update: Purposeyuliana160793No ratings yet
- Artículo 3 - Malignancies. Corrona RegistryDocument7 pagesArtículo 3 - Malignancies. Corrona RegistryNicolas CharrisNo ratings yet
- Gomella 2009Document8 pagesGomella 2009Evelynππ θσυNo ratings yet
- ST Gallen 2021 A OncologyDocument20 pagesST Gallen 2021 A OncologyJorge Apolo PinzaNo ratings yet
- A Novel Radiogenomics Biomarker For Predicting Treatment Response and Pneumotoxicity From Programmed Cell Death Protein or Ligand-1 Inhibition Immunotherapy in NSCLCDocument13 pagesA Novel Radiogenomics Biomarker For Predicting Treatment Response and Pneumotoxicity From Programmed Cell Death Protein or Ligand-1 Inhibition Immunotherapy in NSCLCJOSE DIAZNo ratings yet
- UntitledDocument15 pagesUntitledMARTIN DANIEL COLMENAREZ RODRIGUEZNo ratings yet
- Neadyuvancia Cancer de Pene 1Document5 pagesNeadyuvancia Cancer de Pene 1Ivan Perez NestaresNo ratings yet
- Nuhn 2018Document12 pagesNuhn 2018Evelynππ θσυNo ratings yet
- NeutropeniaDocument17 pagesNeutropeniaassajadda lizikriNo ratings yet
- Testicular Cancer GuidelineDocument44 pagesTesticular Cancer GuidelineElssyNo ratings yet
- Cancers 13 04912Document12 pagesCancers 13 04912mirzaNo ratings yet
- Clinical Practice GuidelineDocument7 pagesClinical Practice GuidelineSuwandi AlghozyNo ratings yet
- TCA-12-2161Document9 pagesTCA-12-2161hafidisara05No ratings yet
- Systemic Therapy in The Curative Treatment of Head and Neck Squamous Cell Cancer: A Systematic ReviewDocument11 pagesSystemic Therapy in The Curative Treatment of Head and Neck Squamous Cell Cancer: A Systematic ReviewLorena Sánchez PérezNo ratings yet
- HNF 2 SRO Cho2018Document10 pagesHNF 2 SRO Cho2018Abhinav IngleNo ratings yet
- Clinical Impact of Tumour Burden On The Efficacy oDocument10 pagesClinical Impact of Tumour Burden On The Efficacy oYasar HammorNo ratings yet
- RSE Society - of - Critical - Care - MedicineDocument20 pagesRSE Society - of - Critical - Care - MedicinemjvaldezNo ratings yet
- Neuro OncologyDocument10 pagesNeuro OncologylarissaNo ratings yet
- Systemic Therapy For Advanced Appendiceal Adenocarcinoma: An Analysis From The NCCN Oncology Outcomes Database For Colorectal CancerDocument8 pagesSystemic Therapy For Advanced Appendiceal Adenocarcinoma: An Analysis From The NCCN Oncology Outcomes Database For Colorectal Canceralberto cabelloNo ratings yet
- Prognostic Factors in Nasopharyngeal Carcinoma With Synchronous Liver Metastasis: A Retrospective Study For The Management of TreatmentDocument7 pagesPrognostic Factors in Nasopharyngeal Carcinoma With Synchronous Liver Metastasis: A Retrospective Study For The Management of TreatmentChairul Nurdin AzaliNo ratings yet
- JMP 02 00022Document19 pagesJMP 02 00022Peterpan NguyenNo ratings yet
- Jop 18 00005Document4 pagesJop 18 00005Anonymous 8KN8IR1GTWNo ratings yet
- Jco 2015 64 8931Document10 pagesJco 2015 64 8931Kamila MuyasarahNo ratings yet
- Walk 2020Document19 pagesWalk 2020Marcus ShawNo ratings yet
- LeprosyDocument20 pagesLeprosyHafiz Sulistio UtomoNo ratings yet
- E002435 FullDocument33 pagesE002435 FullAlizaPinkyNo ratings yet
- Jin Et Al-2023-Cardiotoxicity of Lung Cancer Related Immunotherapy Vs ChemotherapyDocument11 pagesJin Et Al-2023-Cardiotoxicity of Lung Cancer Related Immunotherapy Vs ChemotherapyDimas AdhiatmaNo ratings yet
- 10.1245/s10434 018 6369 XDocument9 pages10.1245/s10434 018 6369 Xsayumiholic89No ratings yet
- Critical Reviews in Oncology / HematologyDocument6 pagesCritical Reviews in Oncology / HematologyasdffdsaNo ratings yet
- Efficacy, Safety, and Health-Related Quality of Life With Camrelizumab Plus Pemetrexed and Carboplatin As First-Line Treatment For Advanced Nonsquamous NSCLC With Brain MetastasesDocument11 pagesEfficacy, Safety, and Health-Related Quality of Life With Camrelizumab Plus Pemetrexed and Carboplatin As First-Line Treatment For Advanced Nonsquamous NSCLC With Brain MetastasesJOSE DIAZNo ratings yet
- Standardized Classification Schemes in Reporting Onco 1676551394Document12 pagesStandardized Classification Schemes in Reporting Onco 1676551394Tahir BhatNo ratings yet
- BR Vs CHOPDocument8 pagesBR Vs CHOPabdullahNo ratings yet
- Ricardo - Management of Lung Nodules and Lung Cancer Screening During COVIDDocument10 pagesRicardo - Management of Lung Nodules and Lung Cancer Screening During COVIDCIRUGIA CARDIOTORÁCICA MINIMAMENTE INVASIVANo ratings yet
- Hap+vap Ats - Idsa 2016 (01-20)Document20 pagesHap+vap Ats - Idsa 2016 (01-20)rahayuNo ratings yet
- Risk Factors For Drug-Resistant Streptococcus Pneumoniae and Antibiotic Prescribing Practices in Outpatient Community-Acquired PneumoniaDocument4 pagesRisk Factors For Drug-Resistant Streptococcus Pneumoniae and Antibiotic Prescribing Practices in Outpatient Community-Acquired PneumoniakingkinresmytaNo ratings yet
- The Pattern of Antimicrobial Use For Palliative Care In-Patients During The Last Week of LifeDocument4 pagesThe Pattern of Antimicrobial Use For Palliative Care In-Patients During The Last Week of Lifem1k0eNo ratings yet
- 1 s2.0 S0956566323005869 MainDocument16 pages1 s2.0 S0956566323005869 MainLuís CerdeiraNo ratings yet
- Background: Nivolumab For Recurrent Squamous-Cell Carcinoma of The Head and NeckDocument10 pagesBackground: Nivolumab For Recurrent Squamous-Cell Carcinoma of The Head and NeckjoitNo ratings yet
- Niemann 37Document19 pagesNiemann 37banitavlad5No ratings yet
- 15.promoting End-Of-Life Discussions in Advanced CancerDocument15 pages15.promoting End-Of-Life Discussions in Advanced Cancerbunga mawarNo ratings yet
- Cancer de PancreasDocument12 pagesCancer de PancreasRuben RoaNo ratings yet
- Original ArticlesDocument7 pagesOriginal ArticlesFernando Emanuel Olmedo BroemserNo ratings yet
- Manejo Sarcoma de Kaposi Guia Europea 2019Document11 pagesManejo Sarcoma de Kaposi Guia Europea 2019wilNo ratings yet
- Sasha Brattain - Weebly ResumeDocument3 pagesSasha Brattain - Weebly Resumeapi-451586061No ratings yet
- Airway ExamDocument7 pagesAirway ExamCharmaine LingdasNo ratings yet
- SPINAL CORD INJURY OVERVIEWDocument59 pagesSPINAL CORD INJURY OVERVIEWfazliahNo ratings yet
- ICF and Guidelines - ComPsych v.2022Document5 pagesICF and Guidelines - ComPsych v.2022JAY JOB TabiNo ratings yet
- RLE Nutritional Support NGT FeedingDocument41 pagesRLE Nutritional Support NGT FeedingRoiniel AntonioNo ratings yet
- BDI-II and BAI ReviewDocument3 pagesBDI-II and BAI ReviewMary Winston DozierNo ratings yet
- EpisodeBasedPayment PerspectivesforConsiderationDocument24 pagesEpisodeBasedPayment PerspectivesforConsiderationHazelnutNo ratings yet
- (SURG) Case Surgical Oncology PDFDocument5 pages(SURG) Case Surgical Oncology PDFDave RapaconNo ratings yet
- MK Sastry Nada Protocol The Grassroots TreatmentDocument12 pagesMK Sastry Nada Protocol The Grassroots Treatmentwilyanto yangNo ratings yet
- Noncompartment Model - Pharmacokinetics: DR C. V. S. SubrahmanyamDocument44 pagesNoncompartment Model - Pharmacokinetics: DR C. V. S. SubrahmanyamBandameedi RamuNo ratings yet
- 8th Week Pregnancy - Symptoms, Baby Development, Tips and Body ChangesDocument8 pages8th Week Pregnancy - Symptoms, Baby Development, Tips and Body ChangesamnroNo ratings yet
- 2Document78 pages2api-3744136No ratings yet
- Tertiary Hospital in Major Cities of PakistanDocument79 pagesTertiary Hospital in Major Cities of PakistanGregg AustriaNo ratings yet
- Bhasa InggrisDocument23 pagesBhasa InggrisrinaNo ratings yet
- ImplementingDocument10 pagesImplementingBNo ratings yet
- Psyche A AkDocument21 pagesPsyche A AkSamuel John SaludezNo ratings yet
- Landmark Trials Genitourinary CompilationDocument55 pagesLandmark Trials Genitourinary CompilationBhanuNo ratings yet
- Ravindra Muddana CoursesDocument3 pagesRavindra Muddana CoursesRavindra MuddanaNo ratings yet
- Artikel Medical AcupunctureDocument8 pagesArtikel Medical AcupunctureCamille EgídioNo ratings yet