You might also like
- Hepatitis B Virus and Liver DiseaseFrom EverandHepatitis B Virus and Liver DiseaseJia-Horng KaoNo ratings yet
- Ali2016 Article OutcomesOfTBTreatmentInHIVCo-iDocument9 pagesAli2016 Article OutcomesOfTBTreatmentInHIVCo-itishaNo ratings yet
- HIV-TB Co-Infection With Clinical PresentationDocument6 pagesHIV-TB Co-Infection With Clinical PresentationMarcellia AngelinaNo ratings yet
- Improving Survival With TBDocument8 pagesImproving Survival With TBdani catriaNo ratings yet
- Causes of Death in HIV-infected Persons Who Have Tuberculosis, ThailandDocument7 pagesCauses of Death in HIV-infected Persons Who Have Tuberculosis, Thailandfaradila aninda raesaNo ratings yet
- Paired Matched Case Control Study ChinaDocument12 pagesPaired Matched Case Control Study ChinaBadal BhandarkarNo ratings yet
- 19 Ninan EtalDocument6 pages19 Ninan EtaleditorijmrhsNo ratings yet
- Mortality During Treatment For Tuberculosis A Review of Surveillance Data in A Rural County in KenyaDocument15 pagesMortality During Treatment For Tuberculosis A Review of Surveillance Data in A Rural County in KenyadhaifahinayhNo ratings yet
- Prevalence and Determinants of Human Immunodeficiency Virus and Tuberculosis Co-Infection at Kampala International University Teaching HospitalDocument6 pagesPrevalence and Determinants of Human Immunodeficiency Virus and Tuberculosis Co-Infection at Kampala International University Teaching HospitalKIU PUBLICATION AND EXTENSIONNo ratings yet
- Prognostic Score To Predict Mortality During TB Treatment in TBHIV Co-Infected PatientsDocument12 pagesPrognostic Score To Predict Mortality During TB Treatment in TBHIV Co-Infected PatientsGani ArlondNo ratings yet
- The Burden of Bacteriologically Negative TB DiagnosisDocument9 pagesThe Burden of Bacteriologically Negative TB DiagnosisMeiyanti MeiyantiNo ratings yet
- Early Initiation of ARV Therapy Among TB-HIV Patients in Indonesia Prolongs Survival Rates!Document9 pagesEarly Initiation of ARV Therapy Among TB-HIV Patients in Indonesia Prolongs Survival Rates!Ayu DinafebrianiNo ratings yet
- Early Initiation of ARV Therapy Among TB-HIV Patients in Indonesia Prolongs Survival Rates!Document6 pagesEarly Initiation of ARV Therapy Among TB-HIV Patients in Indonesia Prolongs Survival Rates!Eka CintyaNo ratings yet
- HHS Public Access: Diagnostics For Pulmonary TuberculosisDocument15 pagesHHS Public Access: Diagnostics For Pulmonary TuberculosisPradipta ShivaNo ratings yet
- Tuberculosis Treatment Delay and Nosocomial Exposure Remain Important Risks For Patients Undergoing Regular HemodialysisDocument9 pagesTuberculosis Treatment Delay and Nosocomial Exposure Remain Important Risks For Patients Undergoing Regular HemodialysisRayCassidyNo ratings yet
- Ofx 137Document7 pagesOfx 137Sheila Alcalde RNo ratings yet
- Reference ThesisDocument13 pagesReference ThesisGhina SalsabilaNo ratings yet
- Burden and Consequences of Tuberculosis Among HIV-Infected Individuals Insights From The Itojo Hospital HIV Clinic in Ntungamo DistrictDocument8 pagesBurden and Consequences of Tuberculosis Among HIV-Infected Individuals Insights From The Itojo Hospital HIV Clinic in Ntungamo DistrictKIU PUBLICATION AND EXTENSIONNo ratings yet
- 2017 Article 2662Document11 pages2017 Article 2662Dhani KurniawanNo ratings yet
- TB Anywhere Is TB Everywhere: Commentary Open AccessDocument3 pagesTB Anywhere Is TB Everywhere: Commentary Open AccessSorina ElenaNo ratings yet
- A Research Proposal Paper On Hepatitis C in IndiaDocument32 pagesA Research Proposal Paper On Hepatitis C in IndiaVaruna Singh67% (6)
- Epidemiology of Tuberculosis and HIV Coinfections in Singapore, 2000 2014Document6 pagesEpidemiology of Tuberculosis and HIV Coinfections in Singapore, 2000 2014jessicaNo ratings yet
- 215067-Article Text-530618-1-10-20210927Document7 pages215067-Article Text-530618-1-10-20210927Yayew MaruNo ratings yet
- Short Course Regimens in TB and HIVDocument18 pagesShort Course Regimens in TB and HIVdani catriaNo ratings yet
- Medi 99 E23649Document6 pagesMedi 99 E23649kornelis aribowoNo ratings yet
- Directly Observed TreatmentDocument9 pagesDirectly Observed TreatmentNovelia CarolinNo ratings yet
- TBC and VihDocument12 pagesTBC and VihCynthia O. CórdovaNo ratings yet
- Manuscript HIVDocument29 pagesManuscript HIVSaroj BhattaraiNo ratings yet
- Survival Status and Treatment Outcome ofDocument6 pagesSurvival Status and Treatment Outcome ofEghar EverydayishellNo ratings yet
- Jurnal 10 HariantoDocument7 pagesJurnal 10 Hariantoaryzamelindah channelNo ratings yet
- Management of HIV-associated Tuberculosis in Resource-Limited Settings: A State-Of-The-Art ReviewDocument16 pagesManagement of HIV-associated Tuberculosis in Resource-Limited Settings: A State-Of-The-Art Reviewbarokahgroup groupNo ratings yet
- TB Burden Qatar: (CITATION Abu18 /L 1033)Document10 pagesTB Burden Qatar: (CITATION Abu18 /L 1033)Ahmad HashmiNo ratings yet
- Prevalence of Rifampicin-Resistant Tuberculosis and Treatment Outcomes in HIV PatientsDocument6 pagesPrevalence of Rifampicin-Resistant Tuberculosis and Treatment Outcomes in HIV PatientsHiqmal JayaNo ratings yet
- Supraja Kanipakam Case Study SummaryDocument3 pagesSupraja Kanipakam Case Study Summaryapi-329758130No ratings yet
- Ambo UniversityDocument12 pagesAmbo UniversityArarsa TolasaNo ratings yet
- Tuberculosis Among Migrant WorDocument8 pagesTuberculosis Among Migrant WorBimaSuryaNo ratings yet
- Early Detection of Unhealthy Behaviors, The Prevalence and Receipt of Antiviral Treatment For Disabled Adult Hepatitis B and C CarriersDocument7 pagesEarly Detection of Unhealthy Behaviors, The Prevalence and Receipt of Antiviral Treatment For Disabled Adult Hepatitis B and C CarriersNabillaNo ratings yet
- Fetch ObjectDocument7 pagesFetch ObjectBilly UntuNo ratings yet
- Annals of Medicine and Surgery: ReviewDocument11 pagesAnnals of Medicine and Surgery: ReviewDimas RizkyNo ratings yet
- Tuberculosis and HIV CoDocument34 pagesTuberculosis and HIV CoLouinel JosephNo ratings yet
- Surveillance Evaluation Report of Tuberculosis in District Bhawalpur-2018 by DR Ammara TahirDocument22 pagesSurveillance Evaluation Report of Tuberculosis in District Bhawalpur-2018 by DR Ammara TahirSantosh WadhwaniNo ratings yet
- Influential Factors in TBHIV Co-Infection Among HIV-Positive Patients at Jinja Regional Referral Hospital, UgandaDocument12 pagesInfluential Factors in TBHIV Co-Infection Among HIV-Positive Patients at Jinja Regional Referral Hospital, UgandaKIU PUBLICATION AND EXTENSIONNo ratings yet
- Chapter II ReviewDocument5 pagesChapter II ReviewPardeepCharlyNo ratings yet
- 1 s2.0 S1684118214001790 MainDocument8 pages1 s2.0 S1684118214001790 MainPUPUT PUJIANTINo ratings yet
- 086-092 49958+nursalamDocument7 pages086-092 49958+nursalamSALSABILA RAHMA REFFANANANo ratings yet
- Who Hiv TB FaqDocument5 pagesWho Hiv TB FaqpaipandinNo ratings yet
- A Prospective Study of Tuberculosis and Human Immunodeficiency Virus Infection Clinical Manifestations and Factors Associated with SurvivalDocument8 pagesA Prospective Study of Tuberculosis and Human Immunodeficiency Virus Infection Clinical Manifestations and Factors Associated with SurvivalAbrahamKatimeNo ratings yet
- Research On Prevalence of TB FinalDocument9 pagesResearch On Prevalence of TB FinalBontuNo ratings yet
- Prevalence of Human Immunodeficiency Virus Infection Among Tuberculosis Patients at Infectious Disease Hospital, Kano State, NigeriaDocument8 pagesPrevalence of Human Immunodeficiency Virus Infection Among Tuberculosis Patients at Infectious Disease Hospital, Kano State, NigeriaUMYU Journal of Microbiology Research (UJMR)No ratings yet
- Mortality Among Tuberculosis Patients in The Democratic Republic of CongoDocument7 pagesMortality Among Tuberculosis Patients in The Democratic Republic of CongoGary Rios DionicioNo ratings yet
- Jia2 25392Document10 pagesJia2 25392Herpriiy BatukhNo ratings yet
- Status of Tuberculosis-Related Stigma and Associated Factors: A Cross-Sectional Study in Central ChinaDocument7 pagesStatus of Tuberculosis-Related Stigma and Associated Factors: A Cross-Sectional Study in Central ChinaCharis MurwadiNo ratings yet
- Undiagnosed Tuberculosis in Patients With HIV Infection Who Present With Severe Anaemia at A District HospitalDocument6 pagesUndiagnosed Tuberculosis in Patients With HIV Infection Who Present With Severe Anaemia at A District HospitalDian EsthyNo ratings yet
- Diagnosis & Treatment of Tuberculosis in HIV Co-Infected PatientsDocument16 pagesDiagnosis & Treatment of Tuberculosis in HIV Co-Infected PatientsdevisilalahiNo ratings yet
- Print 3-JEID-01-00003Document7 pagesPrint 3-JEID-01-00003SaskiaaNo ratings yet
- Bioengineering & Biomedical ScienceDocument4 pagesBioengineering & Biomedical ScienceEdwardA.WagyuNo ratings yet
- Extrapulmonary TuberculosisDocument19 pagesExtrapulmonary Tuberculosisanitaabreu123No ratings yet
- RESEARCH ARTICLE Detecting Spatial Clusters of HIV and Hepatitis CoinfectionsDocument16 pagesRESEARCH ARTICLE Detecting Spatial Clusters of HIV and Hepatitis CoinfectionsDicky rahadianNo ratings yet
- Tuberculosis Vih EthiopiaDocument9 pagesTuberculosis Vih Ethiopiajulma1306No ratings yet
- Jurnal Reading IDocument9 pagesJurnal Reading IDwi Andrio SeptadiNo ratings yet
- Bio Sem2 EssayDocument2 pagesBio Sem2 EssayEileen WongNo ratings yet
- Mechatronics Test Questions Set - 1Document13 pagesMechatronics Test Questions Set - 1ChippyVijayanNo ratings yet
- Postmodern EthicsDocument1 pagePostmodern Ethicsgeorge elerickNo ratings yet
- Detailed Lesson Plan in General MathematicsDocument6 pagesDetailed Lesson Plan in General MathematicsAira Jane Irarum78% (18)
- 9709 s15 QP 12Document4 pages9709 s15 QP 12Abrar JahinNo ratings yet
- Sampling and Field Testing at Wastewater Treatment FacilitiesDocument11 pagesSampling and Field Testing at Wastewater Treatment FacilitiesSundarapandiyan SundaramoorthyNo ratings yet
- SGDJ PDFDocument334 pagesSGDJ PDFDouglas Rogério de CastroNo ratings yet
- Unit 4 Early HumansDocument8 pagesUnit 4 Early HumansSepfira ReztikaNo ratings yet
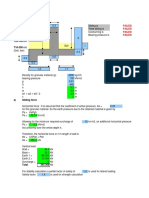
- Sliding, Overturning, Bearing Pressure and Bending Reinforcement Calculations for Retaining WallDocument4 pagesSliding, Overturning, Bearing Pressure and Bending Reinforcement Calculations for Retaining WallAbdul Aziz Julkarnain ZulkifliNo ratings yet
- Top 21 Largest EMS Companies in WorldDocument22 pagesTop 21 Largest EMS Companies in WorldjackNo ratings yet
- PMR205 DR Shawn BakerDocument31 pagesPMR205 DR Shawn Bakerspiridon_andrei2011No ratings yet
- Pantheon-Katalog Eng WebDocument16 pagesPantheon-Katalog Eng WebJoe DoeNo ratings yet
- My Version of Meatlaof Project DraftDocument3 pagesMy Version of Meatlaof Project DraftCloue Faye I. BasalloNo ratings yet
- Time Rates ExplainedDocument6 pagesTime Rates ExplainedAljohn Escalona100% (1)
- Comparative Study of Organic Solvents For Extraction of Copper From Ammoniacal Carbonate Solution Hu2010Document6 pagesComparative Study of Organic Solvents For Extraction of Copper From Ammoniacal Carbonate Solution Hu2010mtanaydinNo ratings yet
- Sabp X 002Document18 pagesSabp X 002Hassan MokhtarNo ratings yet
- Wily Walnut BRAIN SQUEEZERS Vol.1Document116 pagesWily Walnut BRAIN SQUEEZERS Vol.1tarzaman88% (8)
- Karl Marx'S Philosophy and Its Relevance Today: Haroon RashidDocument14 pagesKarl Marx'S Philosophy and Its Relevance Today: Haroon RashidJuan Carlos LinaresNo ratings yet
- Interpuls Novinki 2014Document64 pagesInterpuls Novinki 2014BaklanovaSVNo ratings yet
- Girbau STI-54 STI-77 Parts ManualDocument74 pagesGirbau STI-54 STI-77 Parts Manualrpm14sheratonbsasNo ratings yet
- Cell Structure ActivityDocument4 pagesCell Structure ActivitysharksiedNo ratings yet
- Owner S Manual Subaru LegacyDocument20 pagesOwner S Manual Subaru LegacyLexBgNo ratings yet
- Brief History About Volley BallDocument1 pageBrief History About Volley BallAmbrad, Merlyn H.No ratings yet
- Mohair FiberDocument33 pagesMohair FiberMuhammad Ahsan AftabNo ratings yet
- Diagrama 4 AMBIENT AIR TEMPER..Document1 pageDiagrama 4 AMBIENT AIR TEMPER..Gustavo PérezNo ratings yet
- Zenopus ClassicDocument32 pagesZenopus Classicserenity42No ratings yet
- IRRIGATION ENGINEERING MCQDocument40 pagesIRRIGATION ENGINEERING MCQpriya dharshini100% (1)
- Essotherm 500 PDFDocument8 pagesEssotherm 500 PDFdonyaNo ratings yet
- Normal Distribution PortfolioDocument6 pagesNormal Distribution Portfoliosophia harris100% (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (14)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)