You might also like
- Vendor Document Master ListDocument3 pagesVendor Document Master ListGeetha_jagadish30No ratings yet
- Subject - Financial Services: Class - B.B.A./M.B.ADocument21 pagesSubject - Financial Services: Class - B.B.A./M.B.ADileep SinghNo ratings yet
- Employer'S Virtual Pag-Ibig Enrollment FormDocument2 pagesEmployer'S Virtual Pag-Ibig Enrollment FormRobert Paul A Moreno0% (2)
- Agency DraftDocument3 pagesAgency DraftMuskan TandonNo ratings yet
- SAMPLE Stock Statement Format Submitted in BankDocument2 pagesSAMPLE Stock Statement Format Submitted in BankKkvenkatesh Kkvsraksha64% (44)
- Employee Requisition Form (2015)Document5 pagesEmployee Requisition Form (2015)Ely Ray NacubuanNo ratings yet
- Cash Handling Test - ConcessionsDocument5 pagesCash Handling Test - ConcessionsLizelle LasernaNo ratings yet
- Sap Settlement ConfigurationDocument35 pagesSap Settlement Configurationfaycel045100% (1)
- Revised BBIL Outgoing Wire Transfer FormDocument1 pageRevised BBIL Outgoing Wire Transfer FormRODOLFONo ratings yet
- REG-FO-052 - Requests For Document PDFDocument1 pageREG-FO-052 - Requests For Document PDFRoynard Gadgode SantosNo ratings yet
- Onehub Egobyerno Company Enrollment Form 03112019Document3 pagesOnehub Egobyerno Company Enrollment Form 03112019JeremieNo ratings yet
- Al 01Document2 pagesAl 01chennie100% (1)
- Acord 125Document2 pagesAcord 125Roger ChinchillaNo ratings yet
- Unit 1: What Is The Nature and Scope of Project Management?Document24 pagesUnit 1: What Is The Nature and Scope of Project Management?Rahul kumarNo ratings yet
- Activity Sheet In: Business FinanceDocument8 pagesActivity Sheet In: Business FinanceCatherine Larce100% (1)
- ICARE Preweek APDocument15 pagesICARE Preweek APjohn paulNo ratings yet
- Adding Dropping Change of SubjectsDocument1 pageAdding Dropping Change of SubjectsFreshela AtasNo ratings yet
- Uap Membership Transfer FormDocument2 pagesUap Membership Transfer FormKei PNo ratings yet
- Client Clearance Form (CCF)Document1 pageClient Clearance Form (CCF)kimberly magallanesNo ratings yet
- Employer'S Virtual Pag-Ibig Enrollment Form: Address and Contact DetailsDocument2 pagesEmployer'S Virtual Pag-Ibig Enrollment Form: Address and Contact DetailstheffNo ratings yet
- Employer'S Virtual Pag-Ibig Enrollment FormDocument2 pagesEmployer'S Virtual Pag-Ibig Enrollment FormJhonna Magtoto100% (2)
- Uap Membership Transfer FormDocument1 pageUap Membership Transfer FormMelissa Ann PatanoNo ratings yet
- UoC-ARE-FRM010 Rev 00 Re-Sit & Repeat Registration FormDocument1 pageUoC-ARE-FRM010 Rev 00 Re-Sit & Repeat Registration FormNaqi SahaNo ratings yet
- Uap Membership Transfer FormDocument1 pageUap Membership Transfer FormMary KristineNo ratings yet
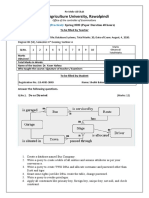
- Arid Agriculture University, Rawalpindi: Final Exam Spring 2020 (Paper Duration 48 Hours) To Be Filled by TeacherDocument6 pagesArid Agriculture University, Rawalpindi: Final Exam Spring 2020 (Paper Duration 48 Hours) To Be Filled by TeacherBOBBY BEATSNo ratings yet
- HDMF-MCRF-Blank FormDocument2 pagesHDMF-MCRF-Blank FormSheryll ArmadaNo ratings yet
- Part A. Application Form: Seaman S Application Prior Joining THE Vessel A ND Assessment ProfileDocument4 pagesPart A. Application Form: Seaman S Application Prior Joining THE Vessel A ND Assessment ProfileCap Karim ElSherbiniNo ratings yet
- IC Employee Leave Request Form 10678Document2 pagesIC Employee Leave Request Form 10678Mary JoyceNo ratings yet
- 11 Employees Transfer Request FormDocument1 page11 Employees Transfer Request FormsekarNo ratings yet
- Endorsement For Issuance of Gate PassDocument1 pageEndorsement For Issuance of Gate PassEMELYN HIWATIGNo ratings yet
- Application Form ICT Exam - RevisedDocument1 pageApplication Form ICT Exam - RevisedMYKO DIONGSONNo ratings yet
- Endorsement For Issuance of Gate Pass - Latest 3Document4 pagesEndorsement For Issuance of Gate Pass - Latest 3Kimgay MaglaquiNo ratings yet
- Job Description Form Template: Company Name Company LogoDocument3 pagesJob Description Form Template: Company Name Company LogopelputriNo ratings yet
- Request FormsDocument3 pagesRequest FormsAnne YasuzukaNo ratings yet
- HRD-009-0 Excuse Slip FormDocument1 pageHRD-009-0 Excuse Slip FormJoshua Kirby AcumanNo ratings yet
- Pup Ace FormDocument1 pagePup Ace FormJulie Ann EfaNo ratings yet
- PECE - PRC Form #004Document2 pagesPECE - PRC Form #004Norman DiolaNo ratings yet
- Uap Membership Transfer Form: A. Personal InformationDocument2 pagesUap Membership Transfer Form: A. Personal InformationDoremiFckyouuNo ratings yet
- IC Web Design Scope of Work 11492 - WORDDocument6 pagesIC Web Design Scope of Work 11492 - WORDSathish_yadav143No ratings yet
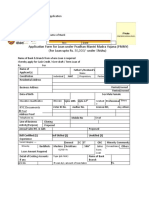
- IPPB Recruitment 2023 Application FormDocument4 pagesIPPB Recruitment 2023 Application FormSankarMathi VaigundhamNo ratings yet
- Indman ApplicationDocument2 pagesIndman Applicationsantoshkumarmishra2009No ratings yet
- SMBP Payment Thru The Bank Form PDFDocument2 pagesSMBP Payment Thru The Bank Form PDFAnonymous t4Iy7YiqC0% (1)
- PUP Ni GwyDocument1 pagePUP Ni GwyAnne Gwyneth HilarioNo ratings yet
- Loan Application (Form-11)Document1 pageLoan Application (Form-11)daily liveNo ratings yet
- Transfer FormDocument1 pageTransfer FormKay EcoNo ratings yet
- Consultants Application FormDocument4 pagesConsultants Application Formamjad121404No ratings yet
- Customer Data Sheet - Revised 1 2Document2 pagesCustomer Data Sheet - Revised 1 2Billy Maravillas Dela CruzNo ratings yet
- Gatepass Endorsement Request Form Rev06Document1 pageGatepass Endorsement Request Form Rev06Subic ForexNo ratings yet
- Company Profile FormateDocument3 pagesCompany Profile Formatefakeone.playNo ratings yet
- Application Form Certificates LS 120.3: Please Indicate The Applicable FormDocument1 pageApplication Form Certificates LS 120.3: Please Indicate The Applicable FormKelvinNo ratings yet
- Board of Intermediate Education, Karachi: CertificateDocument3 pagesBoard of Intermediate Education, Karachi: CertificateTalha Chauhan0% (1)
- ANNEX A Application Form For Promotion AppointmentDocument1 pageANNEX A Application Form For Promotion AppointmentEL BertNo ratings yet
- D3 Application Form For Renewal-UpdatedDocument3 pagesD3 Application Form For Renewal-UpdatedFlorence Benette Gallego100% (1)
- Ot April 7, 2022Document1 pageOt April 7, 2022Kent GarnetNo ratings yet
- Annex C 12072022Document2 pagesAnnex C 12072022Maria Larissa Briñas LptNo ratings yet
- Employer Data Change Request: This Form Is Not For SaleDocument2 pagesEmployer Data Change Request: This Form Is Not For SaleHR ZMCNo ratings yet
- PFF053 Member'SContributionRemittanceForm V03.1Document2 pagesPFF053 Member'SContributionRemittanceForm V03.1FA Marquez64% (11)
- Application Form 030418Document3 pagesApplication Form 030418Noureldin Mohamed AbdelalNo ratings yet
- Application For Academic RecordDocument1 pageApplication For Academic RecordpasambalyrradjohndarNo ratings yet
- Annex A Application Form For Promotion AppointmentDocument1 pageAnnex A Application Form For Promotion Appointmentkaizen shinichiNo ratings yet
- Annex A Application Form For Promotion AppointmentDocument1 pageAnnex A Application Form For Promotion AppointmentAillen Joy GavinoNo ratings yet
- JV-HRD Form-2020-029-Application FormDocument3 pagesJV-HRD Form-2020-029-Application FormCarlo Martin CardinezNo ratings yet
- Applicant Data SheetDocument5 pagesApplicant Data SheetShaira NievaNo ratings yet
- Certificate Form Final1 LEGALDocument2 pagesCertificate Form Final1 LEGALJt100% (1)
- Renewal Certificate Individual Appl Form 2018 - New - May2018Document3 pagesRenewal Certificate Individual Appl Form 2018 - New - May2018Rodney NkunaNo ratings yet
- Performance-Based Certification: How to Design a Valid, Defensible, Cost-Effective ProgramFrom EverandPerformance-Based Certification: How to Design a Valid, Defensible, Cost-Effective ProgramNo ratings yet
- Purchase OrderDocument2 pagesPurchase OrderRox BlancaNo ratings yet
- Warming Disciplinary MeetingDocument1 pageWarming Disciplinary MeetingRox BlancaNo ratings yet
- Liquidation FormDocument1 pageLiquidation FormRox BlancaNo ratings yet
- Pre-Employment Checklist (For New Hire)Document6 pagesPre-Employment Checklist (For New Hire)Rox BlancaNo ratings yet
- 3 Ways To Calculate Your TrainingDocument3 pages3 Ways To Calculate Your TrainingSonal ChaturvediNo ratings yet
- Application Form For Mudra Loan ShishuDocument2 pagesApplication Form For Mudra Loan ShishuSree DigitalNo ratings yet
- Invoice - INV C 2023 2327041Document1 pageInvoice - INV C 2023 2327041Rahul Shrestha (Rahul Shrestha)No ratings yet
- GD 001Document26 pagesGD 001Preethi Raj ThakurNo ratings yet
- Overview of Co-Operative BankingDocument14 pagesOverview of Co-Operative BankingDr. Meghna DangiNo ratings yet
- Two-Folded BrochuresDocument2 pagesTwo-Folded BrochuresRizalyn Joy A. EsparteroNo ratings yet
- 13 ConsumerAwarenessDocument9 pages13 ConsumerAwarenessVibha GoyalNo ratings yet
- Sakshi Jain - Offer APAC - India Summer (Final 2020)Document1 pageSakshi Jain - Offer APAC - India Summer (Final 2020)Sakshi JainNo ratings yet
- Lecture Notes On Intellectual Property LawDocument55 pagesLecture Notes On Intellectual Property LawArieza MontañoNo ratings yet
- RAP Demofest 2022 Letter of InvitationDocument2 pagesRAP Demofest 2022 Letter of InvitationRomss SyNo ratings yet
- Structure of GlobalizationDocument23 pagesStructure of GlobalizationLea HaberNo ratings yet
- Chapter 3 AssignmentDocument9 pagesChapter 3 AssignmentAnas Omar MuffarrejNo ratings yet
- 12 Ida Dme Ibc Conf 2002Document29 pages12 Ida Dme Ibc Conf 2002danaosajoNo ratings yet
- Foaming of Rubber Wood Plastic CompositeDocument65 pagesFoaming of Rubber Wood Plastic CompositeAwad M. El ArabyNo ratings yet
- Collection of Land RevenueDocument13 pagesCollection of Land Revenuemanuarora81No ratings yet
- CASE 02 - Carodan Vs China BankDocument3 pagesCASE 02 - Carodan Vs China Bankbernadeth ranolaNo ratings yet
- Guo 2020Document9 pagesGuo 2020gujjarashrafNo ratings yet
- IPTC 17465 A Comprehensive Approach of Well Integrity SurveillanceDocument11 pagesIPTC 17465 A Comprehensive Approach of Well Integrity SurveillanceEdi Agurto CarrascoNo ratings yet
- Review Test QuestionsDocument24 pagesReview Test QuestionsKent Mathew BacusNo ratings yet
- SWOT Analysis: Strengths WeaknessesDocument2 pagesSWOT Analysis: Strengths WeaknessesALALADE VICTOR aNo ratings yet
- Report: Mean (Expected Value) of A Discrete Random Variable 100%Document2 pagesReport: Mean (Expected Value) of A Discrete Random Variable 100%abel mahendraNo ratings yet
- Building Brand Architecture ReportDocument3 pagesBuilding Brand Architecture ReportTamoor DanishNo ratings yet