You might also like
- GEAR UP Summer Camp Application 2019 FinalDocument3 pagesGEAR UP Summer Camp Application 2019 FinalMrs. LibbyNo ratings yet
- Enrolment Form 2022 2023Document6 pagesEnrolment Form 2022 2023jarrad agiusNo ratings yet
- MLP Registration FormDocument6 pagesMLP Registration FormDoll JonesNo ratings yet
- Free and Reduced Lunch ApplicationDocument2 pagesFree and Reduced Lunch Applicationhakone9027No ratings yet
- Little Miracles Daycare Enrollment FormsDocument14 pagesLittle Miracles Daycare Enrollment Formsapi-259070673No ratings yet
- Combined Enrollment PacketDocument9 pagesCombined Enrollment PacketJustin FXNo ratings yet
- Guideline On Medicine UseDocument2 pagesGuideline On Medicine UseTarleen PandherNo ratings yet
- Declaration of Medical Condition FormDocument1 pageDeclaration of Medical Condition FormCassandra100% (1)
- Parental/Guardian Permission and Liability Waiver Name of Student BirthDocument2 pagesParental/Guardian Permission and Liability Waiver Name of Student BirthlifeteenministryNo ratings yet
- Authorization Letter With No Parent But Need SignatureDocument1 pageAuthorization Letter With No Parent But Need SignatureBretana joanNo ratings yet
- Newborn-Infirmation SheetDocument7 pagesNewborn-Infirmation SheetJONABELL B YLAGANNo ratings yet
- Client Intake Form: (Last) (First) (MI)Document20 pagesClient Intake Form: (Last) (First) (MI)Prabha Gupta0% (1)
- Religious Exemption Form 081815 040816Document2 pagesReligious Exemption Form 081815 040816thor_axxNo ratings yet
- Health History FormDocument4 pagesHealth History Formganesh chowdaryNo ratings yet
- Childcare Application FormDocument2 pagesChildcare Application Formapi-655739915No ratings yet
- Baltimore Medical ReleaseDocument3 pagesBaltimore Medical ReleaseDanielNo ratings yet
- Parental Consent Forms For Minors Travelling Without ParentsDocument4 pagesParental Consent Forms For Minors Travelling Without ParentsLuckyTTinioNo ratings yet
- Vaccine ExemptionVacLib GeorgiaDocument2 pagesVaccine ExemptionVacLib GeorgiaDonnaNo ratings yet
- Dare To Dream 2011 Medical ReleaseDocument1 pageDare To Dream 2011 Medical Releaserls2orgNo ratings yet
- Consent Form and Payment Letter FOBISIA Orchestra and Choral Festival Indonesia May 2024Document4 pagesConsent Form and Payment Letter FOBISIA Orchestra and Choral Festival Indonesia May 2024sage.ebony.meadowNo ratings yet
- Medical Waiver 2014-2015Document4 pagesMedical Waiver 2014-2015api-73377093No ratings yet
- Learners Record BookDocument11 pagesLearners Record BookMarjhun Flores GuingayanNo ratings yet
- Lock in Permission SlipDocument2 pagesLock in Permission SlipRocky Nguyen100% (2)
- TFFT Release Form and Waiver 2017Document3 pagesTFFT Release Form and Waiver 2017Brittany Dickey GalosiNo ratings yet
- AZ Request Exempt Immun Child CareDocument1 pageAZ Request Exempt Immun Child CareDonnaNo ratings yet
- Department of Education AND Department of Health Region IiiDocument1 pageDepartment of Education AND Department of Health Region IiiRej NicdaoNo ratings yet
- Parental Consent: (Complete Name of Student)Document1 pageParental Consent: (Complete Name of Student)arianasNo ratings yet
- Profile Form-Spl Cncrns-New STDNT-LTR SizeDocument4 pagesProfile Form-Spl Cncrns-New STDNT-LTR SizeSalmaNo ratings yet
- Family Application Form: Please Print ClearlyDocument9 pagesFamily Application Form: Please Print ClearlyJulie Lyles CarrNo ratings yet
- Registration PacketDocument8 pagesRegistration PacketTeriElmoreWilsonNo ratings yet
- GCCSACCEmergency Card InformationDocument1 pageGCCSACCEmergency Card InformationAl-juffrey Luis AmilhamjaNo ratings yet
- JR High 2010 Registration FormDocument4 pagesJR High 2010 Registration FormryanlashleeNo ratings yet
- Registration Page 4Document3 pagesRegistration Page 4api-314708963No ratings yet
- BBYO Medical FormDocument2 pagesBBYO Medical Formbenhen37No ratings yet
- ALIVE Registration Form 2010 11Document1 pageALIVE Registration Form 2010 11mjburnsyNo ratings yet
- HPV Consent - EnglishDocument1 pageHPV Consent - EnglishRosebery Andres ParroNo ratings yet
- NSLP App Attach BDocument2 pagesNSLP App Attach Bapi-248185821No ratings yet
- Medical Release Form2010Document2 pagesMedical Release Form2010Kaya AbrahamsonNo ratings yet
- Midrand Montessori Preschool EnrolmentDocument8 pagesMidrand Montessori Preschool Enrolmentanarki85No ratings yet
- 2013-Appendix-2 1-Child-Enrolment-FormDocument15 pages2013-Appendix-2 1-Child-Enrolment-Formapi-311470786No ratings yet
- Student Enrollment FormDocument3 pagesStudent Enrollment Formapi-239237152No ratings yet
- Last First M. D.O.BDocument43 pagesLast First M. D.O.BXlian Myzter Yosa100% (1)
- Infant/Toddler Enrollment PacketDocument8 pagesInfant/Toddler Enrollment PacketlearninghiveNo ratings yet
- Medical ReleaseDocument2 pagesMedical Releaseapi-288406339No ratings yet
- Vaccination Exemption Pursuant To Wisconsin Statute 252.04Document2 pagesVaccination Exemption Pursuant To Wisconsin Statute 252.04DonnaNo ratings yet
- Bowling LockIn Reg From and Consent Form 2010Document3 pagesBowling LockIn Reg From and Consent Form 2010Keon Gunie HuhNo ratings yet
- 5ab OralHealth NotificationLetter - AssessmentWaiver FormDocument3 pages5ab OralHealth NotificationLetter - AssessmentWaiver FormGenevieve AlcalaNo ratings yet
- 1716 Parental ConsentDocument1 page1716 Parental Consentapi-306606945No ratings yet
- Declaration of Exemption From Trustline Registration and Health and Safety Self-CertificationDocument1 pageDeclaration of Exemption From Trustline Registration and Health and Safety Self-CertificationLOLANo ratings yet
- Sequoia Choice - AZ Distance Learning - Mesa, AZ Vaccine WaiverDocument2 pagesSequoia Choice - AZ Distance Learning - Mesa, AZ Vaccine WaiverDonnaNo ratings yet
- Student Emergency Information Card 2021-2022Document1 pageStudent Emergency Information Card 2021-2022api-291350308No ratings yet
- KP Student Application 2024 ReadyDocument4 pagesKP Student Application 2024 Readyapi-245886452No ratings yet
- ShpenrolformDocument5 pagesShpenrolformapi-79523689No ratings yet
- PDF Kids Application Forms 2012Document8 pagesPDF Kids Application Forms 2012api-300139082No ratings yet
- Caregiver MedicalDocument2 pagesCaregiver Medicaloliverfox654No ratings yet
- Intake Interview ChildDocument8 pagesIntake Interview ChildKaz AmosNo ratings yet
- Therapeutic Activities for Children and Teens Coping with Health IssuesFrom EverandTherapeutic Activities for Children and Teens Coping with Health IssuesNo ratings yet
- I-C-E in Case of Emergency: Your Essential Medical JournalFrom EverandI-C-E in Case of Emergency: Your Essential Medical JournalNo ratings yet
- Parenting Through Puberty: Mood Swings, Acne, and Growing PainsFrom EverandParenting Through Puberty: Mood Swings, Acne, and Growing PainsNo ratings yet
- Health Care SystemsDocument15 pagesHealth Care Systems7hrqd6zxjkNo ratings yet
- Boardworks History KS4 MedicineDocument7 pagesBoardworks History KS4 MedicineAlehop Craft BeerNo ratings yet
- Vaccination Schedule of Small and Large Animals NewDocument5 pagesVaccination Schedule of Small and Large Animals NewMahnoor ArshadNo ratings yet
- Article 05Document100 pagesArticle 05Abdulphatah Mohamed IbrahimNo ratings yet
- Jacobson v. MassachusettsDocument2 pagesJacobson v. MassachusettsKyle Janvier VillaluzNo ratings yet
- Polio Cases Rise To 16 New Cases Logged in Quezon City, Mindanao - DOHDocument2 pagesPolio Cases Rise To 16 New Cases Logged in Quezon City, Mindanao - DOHJudel LozadaNo ratings yet
- Health Promotion Disease PreventionDocument23 pagesHealth Promotion Disease PreventionMagnus JordanNo ratings yet
- Jurnal Dokter KeluargaDocument7 pagesJurnal Dokter KeluargaJojo McalisterNo ratings yet
- IATF Resolution 160-ADocument5 pagesIATF Resolution 160-AmonchanNo ratings yet
- Certificate 1Document1 pageCertificate 1Purushottam DamodareNo ratings yet
- Cagayan Valley Center For Health DevelopmentDocument7 pagesCagayan Valley Center For Health Developmentmaria_abigailNo ratings yet
- Q3 First Summative Test in English 6Document5 pagesQ3 First Summative Test in English 6vinn100% (1)
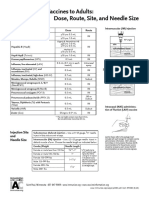
- Administering Vaccines To Adults: Dose, Route, Site, and Needle SizeDocument1 pageAdministering Vaccines To Adults: Dose, Route, Site, and Needle SizeAkashNo ratings yet
- Vaccine Report LatestDocument2 pagesVaccine Report LatestEmmanuel DemostheneNo ratings yet
- Tracking of FormsDocument3 pagesTracking of FormsEUGENE ABULOCNo ratings yet
- Japanese EncephalitisDocument2 pagesJapanese EncephalitisWoke MillennialsNo ratings yet
- 67166-Apvma Veterinary Medicines Technical Report TemplateDocument42 pages67166-Apvma Veterinary Medicines Technical Report Templateali aimanNo ratings yet
- UK - Pandemic Is Over For The Unvaccinated - by Igor ChudovDocument9 pagesUK - Pandemic Is Over For The Unvaccinated - by Igor ChudovOn The PathNo ratings yet
- Algorithm Immunisation Status Jan2020Document1 pageAlgorithm Immunisation Status Jan2020Afsan BulbulNo ratings yet
- BASILIO, Performance Task Module1&2Document2 pagesBASILIO, Performance Task Module1&2Tricia lyxNo ratings yet
- Stand: in Favor: Freedom To Choose COVID-19 VaccineDocument3 pagesStand: in Favor: Freedom To Choose COVID-19 VaccineAlyanna Ysabelle VistanNo ratings yet
- Unending Lockdowns Resulting To Millions of Jobless FilipinoDocument2 pagesUnending Lockdowns Resulting To Millions of Jobless FilipinoShaena LarezaNo ratings yet
- Event 201Document5 pagesEvent 201Pandu DhioNo ratings yet
- The Great Awakening Encyclopedia of EverythingDocument6 pagesThe Great Awakening Encyclopedia of EverythingbiomkeshbakshiNo ratings yet
- Wild and Vaccine Derived Poliovirus Circulation and Implications For Polio EradicationDocument7 pagesWild and Vaccine Derived Poliovirus Circulation and Implications For Polio Eradicationmuhfajar1_42539617No ratings yet
- PCV Demonstration ProgramDocument29 pagesPCV Demonstration Programfikri ajpNo ratings yet
- BCG ChecklistDocument2 pagesBCG ChecklistBSN 1A- Serrano Evytte Joy B.No ratings yet
- Department of Education: School Contingency PlanDocument8 pagesDepartment of Education: School Contingency PlanNIMFA SEPARANo ratings yet
- HHold Final B 2019Document29 pagesHHold Final B 2019Ahmad UsmanNo ratings yet
- Sample Facility Letter To Staff:: This IncludesDocument1 pageSample Facility Letter To Staff:: This IncludesVishwanath Prasad KurmiNo ratings yet