You might also like
- Final Complete Group4 RPDocument10 pagesFinal Complete Group4 RPapi-632526087No ratings yet
- Eval 2 FallDocument3 pagesEval 2 Fallapi-632526087No ratings yet
- HN Proknow ScorecardDocument1 pageHN Proknow Scorecardapi-632526087No ratings yet
- Roils ReportDocument5 pagesRoils Reportapi-632526087No ratings yet
- Csi AssignmentDocument11 pagesCsi Assignmentapi-632526087No ratings yet
- Capstone IIIDocument6 pagesCapstone IIIapi-632526087No ratings yet
- KF Resume 2023Document2 pagesKF Resume 2023api-632526087No ratings yet
- Eval 1 SummerDocument3 pagesEval 1 Summerapi-632526087No ratings yet
- Eval 2 SummerDocument3 pagesEval 2 Summerapi-632526087No ratings yet
- Phase II RodDocument3 pagesPhase II Rodapi-632526087No ratings yet
- Eval 2Document3 pagesEval 2api-632526087No ratings yet
- Clinical Lung LabDocument17 pagesClinical Lung Labapi-632526087No ratings yet
- Intact Breast TangentsDocument2 pagesIntact Breast Tangentsapi-632526087No ratings yet
- Neck PP 2018Document4 pagesNeck PP 2018api-632526087No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- SARMS Powders Prices - David FromDocument1 pageSARMS Powders Prices - David FromOld World OrderNo ratings yet
- AloeliciousDocument25 pagesAloeliciousAlex Miguel GarciaNo ratings yet
- Academic Sessions: Date Topic Speaker Designation DepartmentDocument6 pagesAcademic Sessions: Date Topic Speaker Designation Departmentgoutham valapalaNo ratings yet
- Fine Needle Aspiration Cytology Fnac in EvaluationDocument4 pagesFine Needle Aspiration Cytology Fnac in EvaluationHakim naufaldiNo ratings yet
- Ronald P. Hattis, MD, MPH: Associate Professor, Preventive Medicine, Loma Linda UnivDocument56 pagesRonald P. Hattis, MD, MPH: Associate Professor, Preventive Medicine, Loma Linda UnivAde margusNo ratings yet
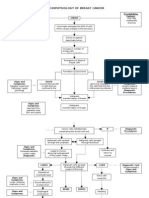
- Pathophysiology of Breast Cancer: Unkno Predisposing Factors: Precipitating FactorsDocument3 pagesPathophysiology of Breast Cancer: Unkno Predisposing Factors: Precipitating FactorsKevin Ercia100% (1)
- ESMO Handbook Nutrition and Cancer 2nd EditionDocument164 pagesESMO Handbook Nutrition and Cancer 2nd EditionClecia SampaioNo ratings yet
- DNB-Radio Therapy: Competency Based Training ProgrammeDocument56 pagesDNB-Radio Therapy: Competency Based Training ProgrammeLinda PhilipsNo ratings yet
- Chapter 19 - The PancreasDocument8 pagesChapter 19 - The PancreasAgnieszka WisniewskaNo ratings yet
- Vitamin D EbookDocument26 pagesVitamin D EbookBelinda100% (3)
- Peng 2016Document5 pagesPeng 2016Alberto GonzalesNo ratings yet
- Cervical Cancer MalaysiaDocument12 pagesCervical Cancer MalaysiaAlbina Mary RajooNo ratings yet
- Primer: Hepatocellular CarcinomaDocument28 pagesPrimer: Hepatocellular CarcinomaAinun Aii NoorNo ratings yet
- ProCaSS Intervention Tool (Final 23-07)Document47 pagesProCaSS Intervention Tool (Final 23-07)Lim ZXNo ratings yet
- Biores CourseDocument43 pagesBiores CoursehldrmoneyNo ratings yet
- Bronchogenic CarcinomaDocument7 pagesBronchogenic CarcinomaRashed ShatnawiNo ratings yet
- Case Report MielopatiDocument37 pagesCase Report MielopatiAnnisaNo ratings yet
- Calling of An Angel - Plus More InfoDocument342 pagesCalling of An Angel - Plus More InfoSemperParatus100% (8)
- 2017 ESMO Essentials For Clinicians Gynaecological TumoursDocument100 pages2017 ESMO Essentials For Clinicians Gynaecological TumoursMaria RamosNo ratings yet
- The Live Food FactorDocument903 pagesThe Live Food FactorCláudio Matos100% (1)
- The Use of Metaphor To Portray Life, Cancer, and Death in John Green's The Fault in Our StarsDocument12 pagesThe Use of Metaphor To Portray Life, Cancer, and Death in John Green's The Fault in Our StarsrifkamsNo ratings yet
- Package - Insert - 08814 - I - en - 30429 - CA 15-3 PDFDocument7 pagesPackage - Insert - 08814 - I - en - 30429 - CA 15-3 PDFadybaila4680No ratings yet
- Factors That Modify Breast Cancer Risk in Women - UpToDateDocument31 pagesFactors That Modify Breast Cancer Risk in Women - UpToDatelaura valeriaNo ratings yet
- Been There, Done That, Wrote The Blog: The Choices and Challenges of Supporting Adolescents and Young Adults With CancerDocument8 pagesBeen There, Done That, Wrote The Blog: The Choices and Challenges of Supporting Adolescents and Young Adults With CancerNanis DimmitrisNo ratings yet
- KRÄUER GANS LISTE ENGLISCH With IINDEX 22.01.2018 PDFDocument231 pagesKRÄUER GANS LISTE ENGLISCH With IINDEX 22.01.2018 PDFRodolfo JarquinNo ratings yet
- Anti-Angiogenic Potential of Theobroma Cacao L. (Cacao) Seed Extract On Anas Platyrhynchos (Mallard Duck) EmbryoDocument41 pagesAnti-Angiogenic Potential of Theobroma Cacao L. (Cacao) Seed Extract On Anas Platyrhynchos (Mallard Duck) EmbryoJulienne Baldonado50% (2)
- DC Healthy People ReportDocument108 pagesDC Healthy People ReportChristina SturdivantNo ratings yet
- Breast CancerDocument18 pagesBreast CancerJohn AlcantaraNo ratings yet
- MCQ PDF 14 PharmacologyDocument4 pagesMCQ PDF 14 PharmacologyBerta São BrazNo ratings yet
- GliomasDocument35 pagesGliomasRabbya Nasir 5No ratings yet