You might also like
- MOCA PEDS 2021 Required ReadingDocument26 pagesMOCA PEDS 2021 Required Readingerica100% (1)
- The Treatment of Migraine Headaches in Children and AdolescentsDocument11 pagesThe Treatment of Migraine Headaches in Children and Adolescentsdo leeNo ratings yet
- Finding the Path in Alzheimer’s Disease: Early Diagnosis to Ongoing Collaborative CareFrom EverandFinding the Path in Alzheimer’s Disease: Early Diagnosis to Ongoing Collaborative CareNo ratings yet
- Characterizing Opioid Use in A US Population With MigraineDocument12 pagesCharacterizing Opioid Use in A US Population With MigraineVagner PinheiroNo ratings yet
- A Clinical Pathway To Standardize Care of Children With Delirium in Pediatric Inpatient Settings-2019Document10 pagesA Clinical Pathway To Standardize Care of Children With Delirium in Pediatric Inpatient Settings-2019Juan ParedesNo ratings yet
- Ger - Leung, Brenda Takeda, Wendy Holec, Victoria. (2018)Document8 pagesGer - Leung, Brenda Takeda, Wendy Holec, Victoria. (2018)Rafael CostaNo ratings yet
- Homeopathic Treatment of Migraine in Children: Results of A Prospective, Multicenter, Observational StudyDocument5 pagesHomeopathic Treatment of Migraine in Children: Results of A Prospective, Multicenter, Observational StudysoylahijadeunvampiroNo ratings yet
- Persistence and Switching Patterns of Oral Migraine Prophylactic Medications Among Patients With Chronic Migraine: A Retrospective Claims AnalysisDocument16 pagesPersistence and Switching Patterns of Oral Migraine Prophylactic Medications Among Patients With Chronic Migraine: A Retrospective Claims AnalysisAzam alausyNo ratings yet
- Bipolar Disorder Vulnerability: Perspectives from Pediatric and High-Risk PopulationsFrom EverandBipolar Disorder Vulnerability: Perspectives from Pediatric and High-Risk PopulationsNo ratings yet
- JMCP 2023 29 1 58Document11 pagesJMCP 2023 29 1 58Javier Martin Bartolo GarciaNo ratings yet
- Glauser2016 PDFDocument14 pagesGlauser2016 PDFDiana De La CruzNo ratings yet
- Individual Cognitive Behavioral Therapy and Combined Family/individual Therapy For Young Adults With Anorexia Nervosa: A Randomized Controlled TrialDocument16 pagesIndividual Cognitive Behavioral Therapy and Combined Family/individual Therapy For Young Adults With Anorexia Nervosa: A Randomized Controlled TrialAggelou MayaNo ratings yet
- Evidence-Based_Treatment_in_the_Field_of_Child_andDocument2 pagesEvidence-Based_Treatment_in_the_Field_of_Child_andRayén F. HuenchunaoNo ratings yet
- George 2019Document8 pagesGeorge 2019Felicia FloraNo ratings yet
- Annett - Et - Al-2015-Pediatric - Blood - & - Cancer 2Document54 pagesAnnett - Et - Al-2015-Pediatric - Blood - & - Cancer 2KarolinaMaślakNo ratings yet
- Treatment for Preventing Tuberculosis in Children and AdolescentsDocument18 pagesTreatment for Preventing Tuberculosis in Children and AdolescentsPrillye DeasyNo ratings yet
- Dhawan 2016Document6 pagesDhawan 2016lilisNo ratings yet
- Antipsychotic Use in Children and Adolescents A.13Document7 pagesAntipsychotic Use in Children and Adolescents A.13jacopo pruccoliNo ratings yet
- Trial of Amitriptyline, Topiramate, and Placebo For Pediatric MigraineDocument10 pagesTrial of Amitriptyline, Topiramate, and Placebo For Pediatric Migraineaditya7No ratings yet
- Psychopharmacology and Pregnancy: Treatment Efficacy, Risks, and GuidelinesFrom EverandPsychopharmacology and Pregnancy: Treatment Efficacy, Risks, and GuidelinesNo ratings yet
- 1 s2.0 S0165032723009357 MainDocument7 pages1 s2.0 S0165032723009357 MainjuanNo ratings yet
- Understanding ADHD Diagnosis and TreatmentDocument3 pagesUnderstanding ADHD Diagnosis and TreatmentIan Mizzel A. DulfinaNo ratings yet
- Ferenchick-Depressionprimarycare-2019 240119 225653Document11 pagesFerenchick-Depressionprimarycare-2019 240119 225653loloNo ratings yet
- Sleep Medicine: Judith A. Owens, Carol L. Rosen, Jodi A. Mindell, Hal L. KirchnerDocument9 pagesSleep Medicine: Judith A. Owens, Carol L. Rosen, Jodi A. Mindell, Hal L. KirchnerHernán MarínNo ratings yet
- Migrain TreatmentDocument10 pagesMigrain TreatmentveNo ratings yet
- Clinician's Manual - Treatment of Pediatric Migraine - D. Lewis, (Springer, 2010) WW PDFDocument75 pagesClinician's Manual - Treatment of Pediatric Migraine - D. Lewis, (Springer, 2010) WW PDFAnonymous VrCndGbKNo ratings yet
- Migraine: Emerging Innovations and Treatment OptionsFrom EverandMigraine: Emerging Innovations and Treatment OptionsShalini ShahNo ratings yet
- The Massachusetts General Hospital Guide to Depression: New Treatment Insights and OptionsFrom EverandThe Massachusetts General Hospital Guide to Depression: New Treatment Insights and OptionsBenjamin G. ShaperoNo ratings yet
- gl0087 PDFDocument58 pagesgl0087 PDFNurul HikmahNo ratings yet
- Medication PrescribingDocument13 pagesMedication PrescribingadrianaNo ratings yet
- SDOM Promising TherapiesDocument16 pagesSDOM Promising TherapiesdarlingcarvajalduqueNo ratings yet
- Pro M.Document8 pagesPro M.lysafontaineNo ratings yet
- Original Article: Childhood Epilepsy Prognostic Factors in Predicting The Treatment FailureDocument8 pagesOriginal Article: Childhood Epilepsy Prognostic Factors in Predicting The Treatment FailureAisya FikritamaNo ratings yet
- Jones Et Al 2018 Psychoeducational Interventions in Adolescent Depression PDFDocument20 pagesJones Et Al 2018 Psychoeducational Interventions in Adolescent Depression PDFAliftaNo ratings yet
- Genetics, revised edition: A Guide for Students and Practitioners of Nursing and Health CareFrom EverandGenetics, revised edition: A Guide for Students and Practitioners of Nursing and Health CareNo ratings yet
- Supportive Care in Pediatric Oncology: A Practical Evidence-Based ApproachFrom EverandSupportive Care in Pediatric Oncology: A Practical Evidence-Based ApproachJames H. FeusnerNo ratings yet
- Pediatric Integrative PDFDocument21 pagesPediatric Integrative PDFallexyssNo ratings yet
- Alcohol, Drugs and Medication in Pregnancy: The Long Term Outcome for the ChildFrom EverandAlcohol, Drugs and Medication in Pregnancy: The Long Term Outcome for the ChildPhilip M PreeceRating: 1 out of 5 stars1/5 (1)
- Artigo Lancet Medicamentos AnsiedadeDocument10 pagesArtigo Lancet Medicamentos AnsiedadeRebecca DiasNo ratings yet
- Articles: BackgroundDocument10 pagesArticles: BackgroundPsiquiatría CESAMENo ratings yet
- Epilepsy & Behavior: Shanna M. Guilfoyle, Sally Monahan, Cindy Wesolowski, Avani C. ModiDocument6 pagesEpilepsy & Behavior: Shanna M. Guilfoyle, Sally Monahan, Cindy Wesolowski, Avani C. ModiJhonny BatongNo ratings yet
- Treatment of Pediatric Migraine: Current Treatment Options in Neurology January 2015Document20 pagesTreatment of Pediatric Migraine: Current Treatment Options in Neurology January 2015akshayajainaNo ratings yet
- A Systematic Review of Psychosocial Interventions For Children and Young People With EpilepsyDocument40 pagesA Systematic Review of Psychosocial Interventions For Children and Young People With EpilepsyFERNANDO ALVESNo ratings yet
- Article 4Document8 pagesArticle 4gogih64190No ratings yet
- Identifying Perinatal Depression and Anxiety: Evidence-based Practice in Screening, Psychosocial Assessment and ManagementFrom EverandIdentifying Perinatal Depression and Anxiety: Evidence-based Practice in Screening, Psychosocial Assessment and ManagementJeannette MilgromNo ratings yet
- Psychopharmacology of AutismDocument17 pagesPsychopharmacology of AutismMichelle2No ratings yet
- Therapist's Guide to Pediatric Affect and Behavior RegulationFrom EverandTherapist's Guide to Pediatric Affect and Behavior RegulationNo ratings yet
- Advances in Psychosocial OncologyDocument7 pagesAdvances in Psychosocial OncologyVanessa SilvaNo ratings yet
- Homeopathic Preparations For Preventing and Treating Acute Upper Respiratory Tract Infections in Children: A Systematic Review and Meta-AnalysisDocument10 pagesHomeopathic Preparations For Preventing and Treating Acute Upper Respiratory Tract Infections in Children: A Systematic Review and Meta-AnalysisCarlos Arturo Vera VásquezNo ratings yet
- Neurotechnology and Brain Stimulation in Pediatric Psychiatric and Neurodevelopmental DisordersFrom EverandNeurotechnology and Brain Stimulation in Pediatric Psychiatric and Neurodevelopmental DisordersLindsay M. ObermanNo ratings yet
- CBTforpediatricchronicmigraine JAMAeditorial Dec2013 PDFDocument3 pagesCBTforpediatricchronicmigraine JAMAeditorial Dec2013 PDFFlory23ibc23No ratings yet
- Cognitive Behavioral Therapy For Treatment of Pediatric Chronic MigraineDocument3 pagesCognitive Behavioral Therapy For Treatment of Pediatric Chronic MigraineFlory23ibc23No ratings yet
- Diet and Nutrition On MigraineDocument17 pagesDiet and Nutrition On MigraineRenju KuriakoseNo ratings yet
- Timlim 2014Document14 pagesTimlim 2014Romina Fernanda Inostroza NaranjoNo ratings yet
- Articulo 1Document8 pagesArticulo 1Silvia CastellanosNo ratings yet
- Self-assessment Questions for Clinical Molecular GeneticsFrom EverandSelf-assessment Questions for Clinical Molecular GeneticsRating: 5 out of 5 stars5/5 (1)
- My ProjectDocument34 pagesMy ProjectrahmatullahqueenmercyNo ratings yet
- The Effectiveness of Psychosocial Interventions For Psychological Outcomes in Pediatric Oncology: A Systematic ReviewDocument21 pagesThe Effectiveness of Psychosocial Interventions For Psychological Outcomes in Pediatric Oncology: A Systematic ReviewFirnawati MaspekeNo ratings yet
- Guideline MD Listing and Authorization MDS-G5 PDFDocument153 pagesGuideline MD Listing and Authorization MDS-G5 PDFSyed SalmanNo ratings yet
- Liquefaction of Soil in KathmanduDocument9 pagesLiquefaction of Soil in Kathmanduajay shresthaNo ratings yet
- Medical Imaging - Seminar Topics Project Ideas On Computer ...Document52 pagesMedical Imaging - Seminar Topics Project Ideas On Computer ...Andabi JoshuaNo ratings yet
- Engine Cpta Czca Czea Ea211 EngDocument360 pagesEngine Cpta Czca Czea Ea211 EngleuchiNo ratings yet
- Datasheet 1MBH 50D - 60Document5 pagesDatasheet 1MBH 50D - 60jtec08No ratings yet
- Infineon IKCM30F60GD DataSheet v02 - 05 ENDocument17 pagesInfineon IKCM30F60GD DataSheet v02 - 05 ENBOOPATHIMANIKANDAN SNo ratings yet
- Activity No.1 in GED 103Document2 pagesActivity No.1 in GED 103Kenneth HerreraNo ratings yet
- Lecture 8: Dynamics Characteristics of SCR: Dr. Aadesh Kumar AryaDocument9 pagesLecture 8: Dynamics Characteristics of SCR: Dr. Aadesh Kumar Aryaaadesh kumar aryaNo ratings yet
- Vietnamese sentence structure: key rules for SVO ordering, adjective and adverb placementDocument7 pagesVietnamese sentence structure: key rules for SVO ordering, adjective and adverb placementvickyzaoNo ratings yet
- Oil & Gas Rig Roles Functions ProcessesDocument5 pagesOil & Gas Rig Roles Functions ProcessesAnant Ramdial100% (1)
- Social Studies Bece Mock 2024Document6 pagesSocial Studies Bece Mock 2024awurikisimonNo ratings yet
- Xerox University Microfilms: 300 North Zeeb Road Ann Arbor, Michigan 48106Document427 pagesXerox University Microfilms: 300 North Zeeb Road Ann Arbor, Michigan 48106Muhammad Haris Khan KhattakNo ratings yet
- Dcs Ict2113 (Apr22) - LabDocument6 pagesDcs Ict2113 (Apr22) - LabMarwa NajemNo ratings yet
- Einstein and Oppenheimer's Real Relationship Was Cordial and Complicated Vanity FairDocument1 pageEinstein and Oppenheimer's Real Relationship Was Cordial and Complicated Vanity FairrkwpytdntjNo ratings yet
- Official Statement On Public RelationsDocument1 pageOfficial Statement On Public RelationsAlexandra ZachiNo ratings yet
- Shimano 105 Gear Change ManualDocument1 pageShimano 105 Gear Change Manual1heUndertakerNo ratings yet
- Registration Confirmation: 315VC18331 Aug 24 2009 7:47PM Devashish Chourasiya 24/05/1989 Mechanical RanchiDocument2 pagesRegistration Confirmation: 315VC18331 Aug 24 2009 7:47PM Devashish Chourasiya 24/05/1989 Mechanical Ranchicalculatorfc101No ratings yet
- Pressure Variation in Tunnels Sealed Trains PDFDocument258 pagesPressure Variation in Tunnels Sealed Trains PDFsivasankarNo ratings yet
- John Constantine Rouge Loner Primordial Orphan Paranormal DetectiveDocument4 pagesJohn Constantine Rouge Loner Primordial Orphan Paranormal DetectiveMirko PrćićNo ratings yet
- D 4 Development of Beam Equations: M X V XDocument1 pageD 4 Development of Beam Equations: M X V XAHMED SHAKERNo ratings yet
- Phy 111 - Eos Exam 2015Document7 pagesPhy 111 - Eos Exam 2015caphus mazengeraNo ratings yet
- Netprobe 2000Document351 pagesNetprobe 2000Jordon CampbellNo ratings yet
- ATC Flight PlanDocument21 pagesATC Flight PlanKabanosNo ratings yet
- Sims4 App InfoDocument5 pagesSims4 App InfooltisorNo ratings yet
- Galvanic CorrosionDocument5 pagesGalvanic Corrosionsatheez3251No ratings yet
- Hot and Cold CorrosionDocument6 pagesHot and Cold CorrosioniceburnerNo ratings yet
- Text EditorDocument2 pagesText EditorVarunNo ratings yet
- SIGA Monitoring ToolDocument3 pagesSIGA Monitoring ToolMhalou Jocson EchanoNo ratings yet
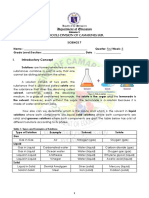
- SCI 7 Q1 WK5 Solutions A LEA TOMASDocument5 pagesSCI 7 Q1 WK5 Solutions A LEA TOMASJoyce CarilloNo ratings yet
- Valve Control System On A Venturi To Control FiO2 A Portable Ventilator With Fuzzy Logic Method Based On MicrocontrollerDocument10 pagesValve Control System On A Venturi To Control FiO2 A Portable Ventilator With Fuzzy Logic Method Based On MicrocontrollerIAES IJAINo ratings yet