You might also like
- Differences Between Democrats and RepublicansDocument4 pagesDifferences Between Democrats and RepublicansmiaubooksNo ratings yet
- Blood Physiology 2022Document116 pagesBlood Physiology 2022Gurmessa FekaduNo ratings yet
- Abacus & Junior Vedic Maths SyllabusDocument2 pagesAbacus & Junior Vedic Maths SyllabusDayalan ArunachalamNo ratings yet
- 2005 Sea-Doo 3D RFIDocument124 pages2005 Sea-Doo 3D RFIJessica DziakNo ratings yet
- Cesarean Scar Pregnancies and Their ManagementDocument7 pagesCesarean Scar Pregnancies and Their ManagementClinton SitanggangNo ratings yet
- Grade 7-Advanced Science Environmental ScienceDocument8 pagesGrade 7-Advanced Science Environmental ScienceChrisel Luat LopezNo ratings yet
- Omphalocele Associated With A PDFDocument5 pagesOmphalocele Associated With A PDFUtama puteraNo ratings yet
- Bilateral Adnexal Masses During Pregnancy and Torsion ComplicationDocument4 pagesBilateral Adnexal Masses During Pregnancy and Torsion ComplicationInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Incidence of The Bell'Clapper Deformity in An Autopsy SeriesDocument3 pagesIncidence of The Bell'Clapper Deformity in An Autopsy SeriesOttofianus Hewick KalangiNo ratings yet
- Keys2012 6Document5 pagesKeys2012 6TRIANDINI TRIANDININo ratings yet
- Ovarian Torsion in Pregnancy A Case ReportDocument3 pagesOvarian Torsion in Pregnancy A Case ReportCakraEkkyNo ratings yet
- Intrauterine Fetal TransfusionsDocument10 pagesIntrauterine Fetal TransfusionsSaddam FuadNo ratings yet
- Management of Uterine Inversion: Operative TechniquesDocument4 pagesManagement of Uterine Inversion: Operative TechniquesMuhammad AzkaNo ratings yet
- Artigo Gravidez EctópicaDocument2 pagesArtigo Gravidez EctópicaKevin UchoaNo ratings yet
- Hirose 2003Document5 pagesHirose 2003lakshay raoNo ratings yet
- CorrespondenceDocument2 pagesCorrespondenceShariq RiazNo ratings yet
- A Case of Body Stalk Anomaly Arising After Invitro Fertilization at 26 Week' GestationDocument3 pagesA Case of Body Stalk Anomaly Arising After Invitro Fertilization at 26 Week' GestationasclepiuspdfsNo ratings yet
- Total and Acute Uterine Inversion After Delivery A Case Report PDFDocument4 pagesTotal and Acute Uterine Inversion After Delivery A Case Report PDFatika sgrtNo ratings yet
- Undescended TestisDocument3 pagesUndescended TestisIoannis ValioulisNo ratings yet
- Testicular Torsion in Undescended TestisDocument5 pagesTesticular Torsion in Undescended TestisjimNo ratings yet
- Spontaneous Rupture of An Unscarred GravidDocument4 pagesSpontaneous Rupture of An Unscarred GraviddelaNo ratings yet
- Twin Gestation in A Uterus Didelphys With Only One Functional Cervix A Case ReportDocument4 pagesTwin Gestation in A Uterus Didelphys With Only One Functional Cervix A Case ReportRIECHELLE SEVILLANo ratings yet
- Urological Science: Jiun-Hung Geng, Chun-Nung HuangDocument4 pagesUrological Science: Jiun-Hung Geng, Chun-Nung Huangyerich septaNo ratings yet
- 1969 556 560 OctDocument5 pages1969 556 560 OctAakanksha AwariNo ratings yet
- Cesarean Scar Ectopic Pregnancies: Etiology, Diagnosis, and ManagementDocument9 pagesCesarean Scar Ectopic Pregnancies: Etiology, Diagnosis, and ManagementDinorah MarcelaNo ratings yet
- Case Reports in Women's HealthDocument4 pagesCase Reports in Women's Healthowadokunquick3154No ratings yet
- Megalourethra - Clinical Review and ManagementDocument4 pagesMegalourethra - Clinical Review and ManagementNugroho HarsonoNo ratings yet
- 01 Testis Sparing Surgery For Epidermoid Cyst of Testis in A 3 Year Old BoyDocument3 pages01 Testis Sparing Surgery For Epidermoid Cyst of Testis in A 3 Year Old BoyAli AhmadNo ratings yet
- Cervical Ectopic Pregnancy After in Vitro Fertilization: Case Report Successfully Treated With Cervical Electric AspirationDocument5 pagesCervical Ectopic Pregnancy After in Vitro Fertilization: Case Report Successfully Treated With Cervical Electric AspirationMatias Alarcon ValdesNo ratings yet
- Bowl in 2017Document12 pagesBowl in 2017kafosidNo ratings yet
- Testicular Torsion: An Analysis of Sixteen Consecutive Cases and A Review of The LiteratureDocument3 pagesTesticular Torsion: An Analysis of Sixteen Consecutive Cases and A Review of The LiteratureLea Bali Ulina SinurayaNo ratings yet
- A Rare Case of Endometriosis in Turners SyndromeDocument3 pagesA Rare Case of Endometriosis in Turners SyndromeElison J PanggaloNo ratings yet
- B-Lynch Uterine Compression Suture For PDocument3 pagesB-Lynch Uterine Compression Suture For PBagusHibridaNo ratings yet
- 1 s2.0 S1028455909601686 MainDocument5 pages1 s2.0 S1028455909601686 MainAgudisarfNo ratings yet
- Thoracic-Omphalopagus Conjoined Twins A Case Report and Review of The LiteratureDocument3 pagesThoracic-Omphalopagus Conjoined Twins A Case Report and Review of The LiteratureInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Case Report: Retained Intrauterine Device (IUD) : Triple Case Report and Review of The LiteratureDocument9 pagesCase Report: Retained Intrauterine Device (IUD) : Triple Case Report and Review of The LiteratureYosie Yulanda PutraNo ratings yet
- Case Report: MRI Detection of Uterine Necrosis After Uterine Artery Embolization For FibroidsDocument4 pagesCase Report: MRI Detection of Uterine Necrosis After Uterine Artery Embolization For FibroidsAnwar Ul HaqueNo ratings yet
- 2017 Pediatric Testicular TorsionDocument12 pages2017 Pediatric Testicular TorsionVladimir BasurtoNo ratings yet
- Lin 2019Document3 pagesLin 2019Mahmoud AbouelsoudNo ratings yet
- Effectiveness of Delayed Absorbable Monofila - 2014 - Taiwanese Journal of ObsteDocument3 pagesEffectiveness of Delayed Absorbable Monofila - 2014 - Taiwanese Journal of ObsteSami KahtaniNo ratings yet
- An Unusual Localization of Leiomyoma: Vaginal LeiomyomaDocument4 pagesAn Unusual Localization of Leiomyoma: Vaginal Leiomyomaistiana sariNo ratings yet
- Journal of Pediatric Surgery Case ReportsDocument3 pagesJournal of Pediatric Surgery Case ReportsKhaidar Ismail JuWiNo ratings yet
- Abrasio PlacentaDocument3 pagesAbrasio Placentamuhammad azamNo ratings yet
- Umbilical Cord Hernias: Prenatal Diagnosis and Natural HistoryDocument4 pagesUmbilical Cord Hernias: Prenatal Diagnosis and Natural HistoryFriska GriffinNo ratings yet
- University of Colorado School of Medicine University of Colorado School of Medicine and Children's Hospital ColoradoDocument2 pagesUniversity of Colorado School of Medicine University of Colorado School of Medicine and Children's Hospital ColoradoashwiniNo ratings yet
- Omphalocele, Exstrophy of Cloaca, Imperforate Anus, and Spinal Defect Complex, Multiple Major Reconstructive Surgeries NeededDocument4 pagesOmphalocele, Exstrophy of Cloaca, Imperforate Anus, and Spinal Defect Complex, Multiple Major Reconstructive Surgeries NeededluqmanhasansNo ratings yet
- Wilson 2006Document5 pagesWilson 2006RizzaNo ratings yet
- Oup Accepted Manuscript 2020Document3 pagesOup Accepted Manuscript 2020Rizka Desti AyuniNo ratings yet
- A Large Parasitic Dermoid Cyst in The Pouch of Douglas: A Torsion Complication?Document4 pagesA Large Parasitic Dermoid Cyst in The Pouch of Douglas: A Torsion Complication?RaidenNo ratings yet
- Bilobed Testicle in Children - Diagnosis and ManagementDocument2 pagesBilobed Testicle in Children - Diagnosis and ManagementJad DegheiliNo ratings yet
- Kista Terpluntir NcbiDocument2 pagesKista Terpluntir NcbiFatimahNo ratings yet
- Uterine RuptureDocument3 pagesUterine RuptureAndreaAlexandraNo ratings yet
- Incompetent Department: CervixDocument5 pagesIncompetent Department: CervixFaradiba NoviandiniNo ratings yet
- Do Zavanelli ModifDocument3 pagesDo Zavanelli ModifSAKAI69No ratings yet
- Leong Et Al-2004-BJOG: An International Journal of Obstetrics & GynaecologyDocument2 pagesLeong Et Al-2004-BJOG: An International Journal of Obstetrics & GynaecologyAngie MandeoyaNo ratings yet
- Echinococcosis of The Spleen During Pregnancy: The Israel Medical Association Journal: IMAJ May 2001Document3 pagesEchinococcosis of The Spleen During Pregnancy: The Israel Medical Association Journal: IMAJ May 2001Ibtissam BelehssenNo ratings yet
- University Journal of Surgery and Surgical Specialities: Dhivya Lakshmi S JDocument4 pagesUniversity Journal of Surgery and Surgical Specialities: Dhivya Lakshmi S JYonathanWaisendiNo ratings yet
- Laparoscopic Ovarian Suspension Before IrradiationDocument3 pagesLaparoscopic Ovarian Suspension Before IrradiationFreddy Chavez VasquezNo ratings yet
- Myopia and Delivery: Should Mode of Delivery Be in Uenced by Moderate and High Myopia?Document3 pagesMyopia and Delivery: Should Mode of Delivery Be in Uenced by Moderate and High Myopia?Prinastiti Tia SetiawatiNo ratings yet
- 170031-Article Text-437088-1-10-20180420Document6 pages170031-Article Text-437088-1-10-20180420Ghani Ikhsan MajidNo ratings yet
- The Paediatric Thymus: Recognising Normal and Ectopic Thymic TissueDocument11 pagesThe Paediatric Thymus: Recognising Normal and Ectopic Thymic TissueFifi FathiraNo ratings yet
- Breast Reconstruction With Free Anterolateral Thigh FlapDocument5 pagesBreast Reconstruction With Free Anterolateral Thigh Flapcusom34No ratings yet
- Case Report: Unusual Presentations in Inguinal Hernia: Four Cases With Review of LiteratureDocument7 pagesCase Report: Unusual Presentations in Inguinal Hernia: Four Cases With Review of LiteratureHolly JonesNo ratings yet
- Term Live Primary Ovarian Pregnancy A Case ReportDocument4 pagesTerm Live Primary Ovarian Pregnancy A Case ReportNico PlantadoNo ratings yet
- The CervixFrom EverandThe CervixJoseph JordanNo ratings yet
- Children 10 00643Document10 pagesChildren 10 00643miaubooksNo ratings yet
- The Witcher (Video Game) : Jump To Navigationjump To SearchDocument11 pagesThe Witcher (Video Game) : Jump To Navigationjump To SearchmiaubooksNo ratings yet
- Industrial Preparation and VarietiesDocument3 pagesIndustrial Preparation and VarietiesmiaubooksNo ratings yet
- Histology,: (Help 1)Document1 pageHistology,: (Help 1)miaubooksNo ratings yet
- Early Life, Training, and Medical CareerDocument2 pagesEarly Life, Training, and Medical CareermiaubooksNo ratings yet
- The Diseases You Suffer From: MelaninDocument2 pagesThe Diseases You Suffer From: MelaninmiaubooksNo ratings yet
- Adjectives Describing People and Personal Qualities Vocabulary Word ListDocument2 pagesAdjectives Describing People and Personal Qualities Vocabulary Word ListmiaubooksNo ratings yet
- CAE 1 BookDocument192 pagesCAE 1 Bookromeroyunge100% (2)
- Coord Angle and BearingDocument18 pagesCoord Angle and BearingvNo ratings yet
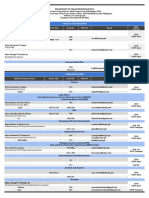
- Updated DOTr Directory As of 29 October 2021Document9 pagesUpdated DOTr Directory As of 29 October 2021Twinkle MiguelNo ratings yet
- Customer Service Skills For Success 6th Edition Lucas Test Bank 1Document36 pagesCustomer Service Skills For Success 6th Edition Lucas Test Bank 1yolandarichardsqiyrfwmazc100% (23)
- Meat PieDocument13 pagesMeat Piecrispitty100% (1)
- Vandex Plug: Rapid-Setting, Crystalline Hydraulic CementDocument2 pagesVandex Plug: Rapid-Setting, Crystalline Hydraulic CementQuerubin EboliNo ratings yet
- EmpathyDocument5 pagesEmpathyHijaab KhaanNo ratings yet
- Le - 2 Sep. 2019: Reçuclt/Cih/IthDocument18 pagesLe - 2 Sep. 2019: Reçuclt/Cih/IthAlero ViteNo ratings yet
- Optoelectronics Circuit CollectionDocument18 pagesOptoelectronics Circuit CollectionSergiu CristianNo ratings yet
- Queueing TheoryDocument6 pagesQueueing TheoryElmer BabaloNo ratings yet
- Numerology 666 Meaning: What Angel Number 666 REALLY Means!Document2 pagesNumerology 666 Meaning: What Angel Number 666 REALLY Means!LlNo ratings yet
- PIA Rivalry Strategy MapDocument16 pagesPIA Rivalry Strategy MapRomeo KhanNo ratings yet
- Spring Diameter of Spring Coil/cm Elastic Limit/n Spring Constant/nm-1 MaterialDocument4 pagesSpring Diameter of Spring Coil/cm Elastic Limit/n Spring Constant/nm-1 MaterialZahari Bin BakriNo ratings yet
- Alfa Laval Energy Balance Casestory enDocument2 pagesAlfa Laval Energy Balance Casestory enHélder FernandoNo ratings yet
- Herpes Simplex KeratitisDocument20 pagesHerpes Simplex KeratitisriskhapangestikaNo ratings yet
- BCB NO1) Bearing CatalogDocument17 pagesBCB NO1) Bearing CatalogGabriela TorresNo ratings yet
- Example Lab ReportDocument12 pagesExample Lab ReportHung Dang QuangNo ratings yet
- How To Write A Research Paper With Parenthetical DocumentationDocument5 pagesHow To Write A Research Paper With Parenthetical Documentationc9spy2qzNo ratings yet
- F5 BIG IP LTM 301A 301B Key Notes Feb 2023 1677506622Document63 pagesF5 BIG IP LTM 301A 301B Key Notes Feb 2023 1677506622MuhammadAbidHameedNo ratings yet
- Group 3 Aia ReportDocument26 pagesGroup 3 Aia ReportNAVAS E VNo ratings yet
- Unit P1, P1.1: The Transfer of Energy by Heating ProcessesDocument9 pagesUnit P1, P1.1: The Transfer of Energy by Heating ProcessesTemilola OwolabiNo ratings yet
- Country Item Name Litre Quart Pint Nip 700 ML IndiaDocument17 pagesCountry Item Name Litre Quart Pint Nip 700 ML Indiajhol421No ratings yet
- Biogas Processes and Sustainable DevelopmentDocument199 pagesBiogas Processes and Sustainable DevelopmentH.J.PrabhuNo ratings yet
- TransportationDocument4 pagesTransportationShrinidhi Priyankaa 1912985630No ratings yet
- Concept Paper Group 1Document9 pagesConcept Paper Group 1Kaime KeilarNo ratings yet
- NUMBERS 2 Percentage ChangeDocument2 pagesNUMBERS 2 Percentage ChangeDinangaNo ratings yet
- Police Log July 30, 2016Document16 pagesPolice Log July 30, 2016MansfieldMAPoliceNo ratings yet