You might also like
- Drug Dosage and IV Rates Calculations PDFDocument6 pagesDrug Dosage and IV Rates Calculations PDFvarmaNo ratings yet
- Blood Transfusion GuidelinesDocument21 pagesBlood Transfusion GuidelinesCheska Tablang0% (1)
- Anaesthesia in Obese PatientsDocument72 pagesAnaesthesia in Obese PatientsPraveen RamasamyNo ratings yet
- How to Apply a Cast - Complete GuideDocument3 pagesHow to Apply a Cast - Complete GuideEmil A. AquinoNo ratings yet
- Nursing Practice 1Document4 pagesNursing Practice 1marieNo ratings yet
- Written ReportDocument50 pagesWritten ReportAngel Lynn YlayaNo ratings yet
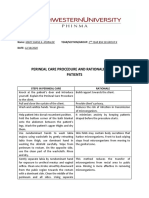
- Perineal Care Steps and RationaleDocument2 pagesPerineal Care Steps and RationaleMary Shane MoraldeNo ratings yet
- Rationale (Enema)Document10 pagesRationale (Enema)Mina RacadioNo ratings yet
- Assess Patient Data Such As Vital Signs, Laboratory Values, and Allergies Before Preparing and Administering Medications by InjectionDocument12 pagesAssess Patient Data Such As Vital Signs, Laboratory Values, and Allergies Before Preparing and Administering Medications by InjectionLRBNo ratings yet
- Fourth Semester FinalDocument14 pagesFourth Semester Finalmara5140No ratings yet
- Assisting IV BTDocument89 pagesAssisting IV BTmhelshy villanuevaNo ratings yet
- Perineal Care, Fleet Enema, Hot Sitz, Immediate Newborn CareDocument18 pagesPerineal Care, Fleet Enema, Hot Sitz, Immediate Newborn CarekesNo ratings yet
- Assignment On TPNDocument14 pagesAssignment On TPNBhawna Joshi100% (8)
- PERINEAL CARE-femaleDocument17 pagesPERINEAL CARE-femaleDarren RobertoNo ratings yet
- BSN 2A Garcia Essential Intrapartum and Newborn Care RationaleDocument5 pagesBSN 2A Garcia Essential Intrapartum and Newborn Care RationaleBellarmine MillenaNo ratings yet
- Misamis University: Administering Parenteral MedicationsDocument10 pagesMisamis University: Administering Parenteral MedicationsAkio OzaragaNo ratings yet
- Taketomo 2019Document328 pagesTaketomo 2019Oscar AguileraNo ratings yet
- Hand Washing Guideline for NursesDocument206 pagesHand Washing Guideline for NursesJosie CalunsagNo ratings yet
- NCM 104 RLE Module 3 FinalsDocument22 pagesNCM 104 RLE Module 3 FinalsAlexander DontonNo ratings yet
- DAVAO DOCTORS COLLEGE NURSING CARE PLANDocument1 pageDAVAO DOCTORS COLLEGE NURSING CARE PLANCrissa KayeNo ratings yet
- Bag Technique: Name: Angeline M. Taghap Grade: Year and Section: BSN 2 B DateDocument11 pagesBag Technique: Name: Angeline M. Taghap Grade: Year and Section: BSN 2 B DateAngeline TaghapNo ratings yet
- Leopold S ManeuverDocument5 pagesLeopold S Maneuverastak ghisingNo ratings yet
- Bag Technique 2 UCDocument2 pagesBag Technique 2 UCSoleil Maxwell0% (1)
- Assisting Delivery Name: Mary Grace G. Rivera Grade: - Year and Section:BSN-2D DateDocument3 pagesAssisting Delivery Name: Mary Grace G. Rivera Grade: - Year and Section:BSN-2D DateMary Grace RiveraNo ratings yet
- Inserting A Straight or Indwelling Catheter (Male)Document3 pagesInserting A Straight or Indwelling Catheter (Male)Mary Grace RiveraNo ratings yet
- Parenteral Administration of DrugsDocument3 pagesParenteral Administration of DrugspauchanmnlNo ratings yet
- Rho (D) Immune Globulin (Human) - RhogamDocument4 pagesRho (D) Immune Globulin (Human) - RhogamJamaicah IliganNo ratings yet
- Perilite Exposure JuecoDocument3 pagesPerilite Exposure JuecoTrishaNo ratings yet
- Course Unit 13 Ethical Issues Related To Technology in The Delivery of Health CareDocument3 pagesCourse Unit 13 Ethical Issues Related To Technology in The Delivery of Health Carerising starNo ratings yet
- Assisting I.V. InsertionDocument4 pagesAssisting I.V. InsertionMary Grace RiveraNo ratings yet
- Self Breast ExaminationDocument2 pagesSelf Breast ExaminationMaye Marquino Lofranco NeriNo ratings yet
- Nursing Care Plan - Genetic Health Before ConceptionDocument1 pageNursing Care Plan - Genetic Health Before ConceptionCristoper BodionganNo ratings yet
- Week 8 - Activity (Case Scenario)Document7 pagesWeek 8 - Activity (Case Scenario)Jollan Marie BuenvenidaNo ratings yet
- Impaired Physical MobilityDocument2 pagesImpaired Physical MobilityAbdelhafiz SusmiranNo ratings yet
- Enc Return DemoDocument3 pagesEnc Return DemoJoyce MadarangNo ratings yet
- Einc Lectures - CeDocument5 pagesEinc Lectures - Ceboxed juiceNo ratings yet
- Open GlovingDocument5 pagesOpen GlovingMierre Sirius100% (1)
- Leopolds Maneuver - Return DemoDocument1 pageLeopolds Maneuver - Return DemornrmmanphdNo ratings yet
- Post-Partum CareDocument4 pagesPost-Partum CarejoethemangoNo ratings yet
- Assessment: Nutrition Diagnosis Nutrition Intervention Monitoring and Evaluation of Nutritional Status Goals: Goals MetDocument3 pagesAssessment: Nutrition Diagnosis Nutrition Intervention Monitoring and Evaluation of Nutritional Status Goals: Goals MetIvan PogiNo ratings yet
- Nursing Foundations I: SOAPIE Documentation for Client with Leg PainDocument2 pagesNursing Foundations I: SOAPIE Documentation for Client with Leg PainJubilee AngNo ratings yet
- Nutrition (LAB) SAS23Document7 pagesNutrition (LAB) SAS23nicoleangela ubasroselloNo ratings yet
- CUNANAN - Changing Monitoring Discontinuing IVFDocument6 pagesCUNANAN - Changing Monitoring Discontinuing IVFAbbyNo ratings yet
- Intramuscular Injection RationaleDocument3 pagesIntramuscular Injection RationaleDUMMY DUMMYNo ratings yet
- Chapter 11 Health EducationDocument12 pagesChapter 11 Health EducationJapaanNo ratings yet
- PRS Ear Instillation - GlovaDocument3 pagesPRS Ear Instillation - GlovaAndrea Colleen GlovaNo ratings yet
- NCM 100 H.A Procedure DPPER 3Document51 pagesNCM 100 H.A Procedure DPPER 3Richelle Joy Durano RegatunaNo ratings yet
- Elderhood: Jerry Mae Chiong Joliza Lancara Dianne Kay Fernandez Rhea Joy GolenaDocument50 pagesElderhood: Jerry Mae Chiong Joliza Lancara Dianne Kay Fernandez Rhea Joy GolenaRj Santiago0% (1)
- Return Demonstration NursingDocument2 pagesReturn Demonstration NursingShing Shang ShongNo ratings yet
- Nursing Procedure For Skills Lab Leopolds ManueverDocument4 pagesNursing Procedure For Skills Lab Leopolds Manueveralyza lumpodNo ratings yet
- Rectal and Vaginal Suppository Insertion GuideDocument2 pagesRectal and Vaginal Suppository Insertion GuideMariah Jane TaladuaNo ratings yet
- Chapter 8: Nursing Care of The Subfertile CoupleDocument10 pagesChapter 8: Nursing Care of The Subfertile CoupleAlyssaGrandeMontimorNo ratings yet
- JRSMU Nursing Skills ChecklistDocument4 pagesJRSMU Nursing Skills ChecklistJustine CagatanNo ratings yet
- Nursing Case Analysis 4Document3 pagesNursing Case Analysis 4Luna GrayNo ratings yet
- Share DRUGSTUDYDocument4 pagesShare DRUGSTUDYTyronne JingcoNo ratings yet
- NDT Reviewer PDFDocument9 pagesNDT Reviewer PDFAnonymousTargetNo ratings yet
- Pregestational & Gestational ConditionsDocument2 pagesPregestational & Gestational ConditionsJheanAlphonsineT.MeansNo ratings yet
- Nursing Care Plan for Magda with EpisiotomyDocument2 pagesNursing Care Plan for Magda with EpisiotomyRainier IbarretaNo ratings yet
- St. Michael's College: Nursing Care Plan FormDocument3 pagesSt. Michael's College: Nursing Care Plan Formacademic purposesNo ratings yet
- Drug Therapeutic Record TemplateDocument1 pageDrug Therapeutic Record TemplateAubrey Justine GaleonNo ratings yet
- 4 P's of Labor and Birth: Presented By: Ana Laurice R. Nastor & Nerissa N. Natata RLE II-7.2Document56 pages4 P's of Labor and Birth: Presented By: Ana Laurice R. Nastor & Nerissa N. Natata RLE II-7.2steffiNo ratings yet
- Female Catheterization ProcedureDocument3 pagesFemale Catheterization ProcedureMacy Marquez100% (1)
- Aseptic TechniqueDocument7 pagesAseptic TechniqueRochele Buenavista- BuenaventuraNo ratings yet
- Diseases Associated in Carbohydrates 3Document2 pagesDiseases Associated in Carbohydrates 3Mary Joy FalcesoNo ratings yet
- Administering An EnemaDocument2 pagesAdministering An EnemaJazzmin Angel ComalingNo ratings yet
- Xavier University - Ateneo de Cagayan College of Nursing: Project: Step-By-Step ProcedureDocument45 pagesXavier University - Ateneo de Cagayan College of Nursing: Project: Step-By-Step ProcedureShamsa AfdalNo ratings yet
- NCM: 112 Care of The Client With Problem in Oxygenation Venipuncture Using Needle or CatheterDocument7 pagesNCM: 112 Care of The Client With Problem in Oxygenation Venipuncture Using Needle or CatheterIssaiah Nicolle CeciliaNo ratings yet
- CU 13. The Role of The Nurse EducatorDocument10 pagesCU 13. The Role of The Nurse EducatorWonie booNo ratings yet
- Sweet Temptation - LOGO PDFDocument2 pagesSweet Temptation - LOGO PDFWonie booNo ratings yet
- Nursing Care Plan for Constipation ReliefDocument3 pagesNursing Care Plan for Constipation ReliefWonie booNo ratings yet
- Student Health Assessment FormDocument1 pageStudent Health Assessment FormWonie booNo ratings yet
- NCP Imbalance-Nutrition.Document5 pagesNCP Imbalance-Nutrition.Wonie booNo ratings yet
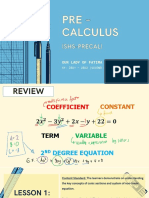
- Lesson 1 - Conics 8Document13 pagesLesson 1 - Conics 8Wonie booNo ratings yet
- Get That Glow!Document2 pagesGet That Glow!Wonie booNo ratings yet
- 3Q Individual Activity #1Document1 page3Q Individual Activity #1Wonie booNo ratings yet
- IV Therapy Article For ExamDocument10 pagesIV Therapy Article For ExamHui HuangNo ratings yet
- PHBP Week1 & 2Document11 pagesPHBP Week1 & 2Katrina EscobarNo ratings yet
- Magnesium SulphateDocument9 pagesMagnesium SulphateMartinNo ratings yet
- Syringe Driver / Syringe Pump: By: Lacsamana, Joan Noemy CDocument6 pagesSyringe Driver / Syringe Pump: By: Lacsamana, Joan Noemy CMr. Christian ParabuacNo ratings yet
- Xii. Medical Management A. Diet 1. Soft Low Salt Low Fat DietDocument4 pagesXii. Medical Management A. Diet 1. Soft Low Salt Low Fat DietLiezelNo ratings yet
- Mannitol For Reduce IOPDocument7 pagesMannitol For Reduce IOPHerryantoThomassawaNo ratings yet
- Principles of Temperature MonitoringDocument8 pagesPrinciples of Temperature MonitoringOllie EvansNo ratings yet
- Scorpion Envenomation Causing Neuromuscular Toxicity (United States, Mexico, Central America, and Southern Africa) - UpToDateDocument28 pagesScorpion Envenomation Causing Neuromuscular Toxicity (United States, Mexico, Central America, and Southern Africa) - UpToDatejoaoalmeida_1955100% (1)
- Pharmacokinetics of Oral and Intravenous Paracetamol (Acetaminophen) When Co-Administered With Intravenous Morphine in Healthy Adult SubjectsDocument10 pagesPharmacokinetics of Oral and Intravenous Paracetamol (Acetaminophen) When Co-Administered With Intravenous Morphine in Healthy Adult SubjectsRara MaharrumNo ratings yet
- Micotil 300 - Elanco - AngliaDocument7 pagesMicotil 300 - Elanco - AngliaandreililioanceaNo ratings yet
- Evaluation Examination For Medicine WardDocument3 pagesEvaluation Examination For Medicine WardMarvick GalimaNo ratings yet
- Specific Criteria Nabl-112 (2012)Document53 pagesSpecific Criteria Nabl-112 (2012)kinnusaraiNo ratings yet
- IV Therapy GuideDocument34 pagesIV Therapy GuideWarrenPeaceNo ratings yet
- The Nurse The Math The Meds Drug Calculations Using Dimensional Analysis 3rd Edition Mulholland Test BankDocument18 pagesThe Nurse The Math The Meds Drug Calculations Using Dimensional Analysis 3rd Edition Mulholland Test Banklaylafarleyh3i8j9100% (24)
- XLW Ec Auto Tensile TesterDocument3 pagesXLW Ec Auto Tensile TesterTri AriadiNo ratings yet
- Guidelines For The Inter and Intrahospital.38 LT PDFDocument88 pagesGuidelines For The Inter and Intrahospital.38 LT PDFTMRC RSCMNo ratings yet
- The Use of Smart Pumps and InformaticsDocument13 pagesThe Use of Smart Pumps and Informaticsapi-489685873No ratings yet
- Non AntimicrobialsDocument88 pagesNon AntimicrobialsArvenaa SubramaniamNo ratings yet
- B Braun RegionalanesthesiaportfolioproductcatalogDocument33 pagesB Braun RegionalanesthesiaportfolioproductcatalogMohammad BilalNo ratings yet
- TM194861ENOUS HOTLINE Disposables and Accessories Technical Sheet Revise 041415Document2 pagesTM194861ENOUS HOTLINE Disposables and Accessories Technical Sheet Revise 041415AphichetNo ratings yet
- 2023 Updated-Nursing Skills ChecklistDocument7 pages2023 Updated-Nursing Skills Checklistapi-652071746No ratings yet
- نسخة اختبارDocument318 pagesنسخة اختبارSami AlanziNo ratings yet
- A Comparison of Sterofundin & RL On Intraoperative Acid Base & Electrolytes Status in Children (ACCM Journal)Document8 pagesA Comparison of Sterofundin & RL On Intraoperative Acid Base & Electrolytes Status in Children (ACCM Journal)TedyJaswadiNo ratings yet