You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Advanced Life Support Questions - Answers PaperDocument5 pagesAdvanced Life Support Questions - Answers Paperjahangirealam50% (10)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Final FRCA Viva Questions From June 2011 Exam Some General Feedback For The Day For Any Future CandidatesDocument56 pagesFinal FRCA Viva Questions From June 2011 Exam Some General Feedback For The Day For Any Future Candidatesjahangirealam89% (9)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- MEDACS ReferenceDocument3 pagesMEDACS ReferencejahangirealamNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Acute Stridor in Children CA1080 v.8Document13 pagesAcute Stridor in Children CA1080 v.8jahangirealamNo ratings yet
- Specialty Doctor in ICU and Anaesthetics Job Description: East and North Hertfordshire NHS TrustDocument20 pagesSpecialty Doctor in ICU and Anaesthetics Job Description: East and North Hertfordshire NHS TrustjahangirealamNo ratings yet
- Applied IM & FM Programs 2018Document269 pagesApplied IM & FM Programs 2018jahangirealamNo ratings yet
- Intubation Checklist 45 060219Document2 pagesIntubation Checklist 45 060219jahangirealamNo ratings yet
- Fibreoptic Intubation Update 2011Document8 pagesFibreoptic Intubation Update 2011jahangirealamNo ratings yet
- Cam PDFDocument13 pagesCam PDFjahangirealamNo ratings yet
- 426-288-18DD-A - Job Description Specialty Doctor August 2018Document11 pages426-288-18DD-A - Job Description Specialty Doctor August 2018jahangirealamNo ratings yet
- Support Staff Employment Application Form September 2017.122288453Document10 pagesSupport Staff Employment Application Form September 2017.122288453jahangirealamNo ratings yet
- I FoundationsDocument7 pagesI FoundationsjahangirealamNo ratings yet
- Dla1a Child PrintDocument61 pagesDla1a Child PrintjahangirealamNo ratings yet
- Obstructive Sleep Apnoea and AnaesthesiaDocument21 pagesObstructive Sleep Apnoea and AnaesthesiajahangirealamNo ratings yet
- Baromtric (89 Pages)Document89 pagesBaromtric (89 Pages)jahangirealamNo ratings yet
- Find Multiples of 2Document1 pageFind Multiples of 2jahangirealamNo ratings yet
- NHS Lothian Medical Application FormDocument17 pagesNHS Lothian Medical Application FormjahangirealamNo ratings yet
- Bier Block (Intravenous Regional Anesthesia), Handout PDFDocument8 pagesBier Block (Intravenous Regional Anesthesia), Handout PDFjahangirealamNo ratings yet
- Duplicate Copy: Balance Due 123001.08Document2 pagesDuplicate Copy: Balance Due 123001.08jahangirealamNo ratings yet
- Dress Up As... : The GruffaloDocument4 pagesDress Up As... : The GruffalojahangirealamNo ratings yet
- List of OSCE Stations in Past Six Months in PLAB Part 2 PLAB Part 2Document12 pagesList of OSCE Stations in Past Six Months in PLAB Part 2 PLAB Part 2jahangirealam100% (1)
- Application SummaryDocument3 pagesApplication SummaryjahangirealamNo ratings yet
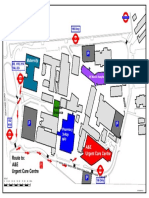
- NPHNew Wayfinding V6Document1 pageNPHNew Wayfinding V6jahangirealamNo ratings yet
- Acute: Renal Failure Management in The NeonateDocument8 pagesAcute: Renal Failure Management in The NeonatejahangirealamNo ratings yet