You might also like
- Bodybuilding Chemical Muscle Enhancement SteroidsDocument226 pagesBodybuilding Chemical Muscle Enhancement SteroidsLak vir Singh100% (3)
- Practical MindfulnessDocument70 pagesPractical Mindfulnessnagaraja100% (4)
- Endocrine SystemDocument14 pagesEndocrine SystemNovie Jane HontiverosNo ratings yet
- Qigong For Strengthening The KidneysDocument15 pagesQigong For Strengthening The Kidneysdan20050505100% (1)
- Adrenal Fatigue Cure Guide (Beat Chronic fatigue): Restoring your Hormones and Controling Thyroidism: Restoring your Hormones and Controling ThyroidismFrom EverandAdrenal Fatigue Cure Guide (Beat Chronic fatigue): Restoring your Hormones and Controling Thyroidism: Restoring your Hormones and Controling ThyroidismRating: 1 out of 5 stars1/5 (1)
- Adrenal Fatigue: Understanding the Symptoms: How Malfunctioning Adrenal Glands Negatively Affect the BodyFrom EverandAdrenal Fatigue: Understanding the Symptoms: How Malfunctioning Adrenal Glands Negatively Affect the BodyNo ratings yet
- Theories of LabourDocument22 pagesTheories of LaboursubashikNo ratings yet
- The Endocrine Glands & Their HormonesDocument35 pagesThe Endocrine Glands & Their HormonesEtta Sagita Leonora100% (1)
- Adrenal Gland DisordersDocument7 pagesAdrenal Gland Disorderscn351073No ratings yet
- Addison' S Disease: Case PresentationDocument34 pagesAddison' S Disease: Case PresentationShane Olanosa PillonarNo ratings yet
- Adrenal InsufficiencyDocument33 pagesAdrenal InsufficiencypukitagabNo ratings yet
- NCM 116: Neurologic Dysfunctions: Joyce Bernadette P. Andot - Anna Delle Nicole P. Aranding, BSN-IIIDocument46 pagesNCM 116: Neurologic Dysfunctions: Joyce Bernadette P. Andot - Anna Delle Nicole P. Aranding, BSN-IIIMercy Anne EcatNo ratings yet
- Addison's DiseaseDocument1 pageAddison's DiseaseDurrotul SalmaNo ratings yet
- Adrenal Fatigue: Enhancing Quality of Life For Patients With A Functional DisorderDocument6 pagesAdrenal Fatigue: Enhancing Quality of Life For Patients With A Functional Disordercraig10140% (1)
- UWorld Endocrinology - Pathology PhysiologyDocument136 pagesUWorld Endocrinology - Pathology PhysiologyDaniel DiasNo ratings yet
- The Teenage Brain: New Knowledge From NeuroscienceDocument7 pagesThe Teenage Brain: New Knowledge From NeuroscienceLegal MomentumNo ratings yet
- Stress Management.Document404 pagesStress Management.James Adhikaram100% (1)
- Introduction To Adrenal Fatigue DR LamDocument21 pagesIntroduction To Adrenal Fatigue DR Lamiri_bal0% (1)
- Addison's DiseaseDocument17 pagesAddison's DiseaseMah Jezthy100% (1)
- 02 StressDocument44 pages02 StressnowayidontwantitNo ratings yet
- Autoimmune DiseasesDocument125 pagesAutoimmune DiseasesJustin Ahorro-DionisioNo ratings yet
- Biology: D.Harish Kannan Topic: Addison's DiseaseDocument7 pagesBiology: D.Harish Kannan Topic: Addison's DiseaseG. ShanjanaNo ratings yet
- Diseases of Circulatory SystemDocument7 pagesDiseases of Circulatory SystemMary Anne YadaoNo ratings yet
- Igcse Biology: Co-Odination and ResponseDocument9 pagesIgcse Biology: Co-Odination and ResponseThamiso GolwelwangNo ratings yet
- Endocrine System: One of Us, and I'm Not Certain Which, Has A Glandular DisorderDocument10 pagesEndocrine System: One of Us, and I'm Not Certain Which, Has A Glandular Disorderroserem2000No ratings yet
- Adrenal Glands MS2Document38 pagesAdrenal Glands MS2Tatiana Leashe WootenNo ratings yet
- Adrenal Gland Grp5Document17 pagesAdrenal Gland Grp5Kathrine GoNo ratings yet
- Stress and AdaptationDocument4 pagesStress and AdaptationAlec Xavier MirandaNo ratings yet
- The Endocrine SystemDocument38 pagesThe Endocrine Systemsaifulla dubaiNo ratings yet
- Adrenal GlandsDocument2 pagesAdrenal GlandsYary MayorNo ratings yet
- Module 3 - Non-Communicable DiseaseDocument2 pagesModule 3 - Non-Communicable DiseasejessafesalazarNo ratings yet
- Hormones, The Endocrine System and HomeostasisDocument5 pagesHormones, The Endocrine System and Homeostasischiusavi77No ratings yet
- Endocrine SystemDocument22 pagesEndocrine SystemUnknownKidNo ratings yet
- NCMB 316 Lecture & RleDocument34 pagesNCMB 316 Lecture & RleVenansius GanggusNo ratings yet
- Adrenal GlandDocument16 pagesAdrenal GlandTanya SinghNo ratings yet
- Chapter 15 - Hormones & Endocrine GlandsDocument17 pagesChapter 15 - Hormones & Endocrine Glandsapi-3728508100% (1)
- Insufisiensi Adrenal (Dr. Makbul)Document52 pagesInsufisiensi Adrenal (Dr. Makbul)Rahmat AzimiNo ratings yet
- Adrenalglandlecture 111115200310 Phpapp01Document25 pagesAdrenalglandlecture 111115200310 Phpapp01varshasharma05No ratings yet
- Adrenal GlandDocument28 pagesAdrenal GlandAthar Habib ShahaniNo ratings yet
- EndocrineDocument7 pagesEndocrineKharrel YballeNo ratings yet
- WK 4 Learning IssuesDocument7 pagesWK 4 Learning Issuesjacintacw7No ratings yet
- AdrenalDocument5 pagesAdrenalJC MolNo ratings yet
- Adrenal Glands: Crishkey Cuario Nathaniel Estipona Mario Revillosa Jopay ContrerasDocument8 pagesAdrenal Glands: Crishkey Cuario Nathaniel Estipona Mario Revillosa Jopay ContrerasKathlene BalicoNo ratings yet
- SCIENCE-REPORT-GROUP-2.pdf 20240211 212133 0000Document48 pagesSCIENCE-REPORT-GROUP-2.pdf 20240211 212133 0000taishishiroganeNo ratings yet
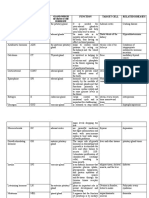
- Hormone Abbreviation Function Target Cell Related Diseases: Gland Which Secretes The HormoneDocument4 pagesHormone Abbreviation Function Target Cell Related Diseases: Gland Which Secretes The HormoneMarianne Jubille CataquisNo ratings yet
- Endo 3 Notes PDFDocument9 pagesEndo 3 Notes PDFDilNo ratings yet
- Lecture 15 - Adrenal Gland BNS KUMDocument17 pagesLecture 15 - Adrenal Gland BNS KUMabdulsaboor30No ratings yet
- BIOLOGY 10 REVIEWER - 3rd QuarterDocument10 pagesBIOLOGY 10 REVIEWER - 3rd QuarterGeromme TudNo ratings yet
- Hormonas de Estrés English FinalDocument46 pagesHormonas de Estrés English FinalGuillermo Alfonso Solórzano MoralesNo ratings yet
- Endocrine System ActivityDocument4 pagesEndocrine System ActivityPablo GarciaNo ratings yet
- Dynamic Balance: Steady BalanceDocument17 pagesDynamic Balance: Steady Balancesakura1717No ratings yet
- The Endocrine Glands & Their HormonesDocument35 pagesThe Endocrine Glands & Their HormonesRizky PratamaNo ratings yet
- CortisolDocument4 pagesCortisollevelupwithlaura21No ratings yet
- Bio - EndocrineDocument16 pagesBio - EndocrineYash PrajapatiNo ratings yet
- Control CoordinationDocument7 pagesControl CoordinationShaurya AgrawalNo ratings yet
- Endocrine Disorders and Their PharmacotherapyDocument4 pagesEndocrine Disorders and Their PharmacotherapyYemaya84No ratings yet
- Stress and AdaptationDocument4 pagesStress and AdaptationJonna EstabilloNo ratings yet
- Lecture 13Document23 pagesLecture 13Rezwan Noor NSUNo ratings yet
- Anatomy & Physiology Endocrine System: Ilah M, SKPDocument36 pagesAnatomy & Physiology Endocrine System: Ilah M, SKPOmbun FajarNo ratings yet
- Steroids AND TerpenesDocument88 pagesSteroids AND Terpenesbuttercuplady_18763No ratings yet
- Ana, Patho UroDocument5 pagesAna, Patho UroDan Ataniel EnsaladaNo ratings yet
- Adrenal GlandDocument9 pagesAdrenal GlandArzooGargNo ratings yet
- Chapter 5 - The Endocrine System - FinalDocument57 pagesChapter 5 - The Endocrine System - FinalKharrel YballeNo ratings yet
- Ca1 DLP Ms2 Nursing Care Management 103 CodyyoungbloodDocument3 pagesCa1 DLP Ms2 Nursing Care Management 103 CodyyoungbloodYoungbloodNo ratings yet
- Anatomy: Pineal GlandDocument5 pagesAnatomy: Pineal GlandJoshua LuminariasNo ratings yet
- Nursing Intervention For DKADocument3 pagesNursing Intervention For DKADarius CrisostomoNo ratings yet
- Anatomy ActivityDocument15 pagesAnatomy ActivityAllesa San JoseNo ratings yet
- Q3 1 EndocrineDocument42 pagesQ3 1 Endocrineerlamay.valeNo ratings yet
- Clinical MarasmusDocument27 pagesClinical MarasmusHANNo ratings yet
- NCMB 316 Lec Midterm 1Document14 pagesNCMB 316 Lec Midterm 1zh4hft6pnzNo ratings yet
- Jillian Michaels - HormonesDocument6 pagesJillian Michaels - HormonesalerynNo ratings yet
- A New Paradigm For Student LearnersDocument92 pagesA New Paradigm For Student LearnersTerry DoyleNo ratings yet
- 4.1 Reading VocabularyDocument4 pages4.1 Reading VocabularyMahmoud RammalNo ratings yet
- CUSHING'S SyndromeDocument9 pagesCUSHING'S SyndromeTheavuthyNo ratings yet
- AldosteronismDocument48 pagesAldosteronismMiguel Cuevas DolotNo ratings yet
- Cortisol II 2020-03 v6Document5 pagesCortisol II 2020-03 v6Parishan SaeedNo ratings yet
- Biochemistry JD 2Document6 pagesBiochemistry JD 2failinNo ratings yet
- Effects of Stress On Human Health: By: Liza Ormol 5 SemesterDocument14 pagesEffects of Stress On Human Health: By: Liza Ormol 5 SemesterANA LEE MENDOZANo ratings yet
- Midl Nursing NowDocument213 pagesMidl Nursing Nowbemina jaNo ratings yet
- Answers To Case StudiesDocument7 pagesAnswers To Case StudiesPhú NguyễnNo ratings yet
- Webinar 14 Juli 2020: Dr. Rachmi Primadiati, Darom, Dherbmed, Cidesco, CibtacDocument35 pagesWebinar 14 Juli 2020: Dr. Rachmi Primadiati, Darom, Dherbmed, Cidesco, CibtacDefi PazdilaNo ratings yet
- Laboratory and Diagnostic Tests Answer KeyDocument25 pagesLaboratory and Diagnostic Tests Answer KeyCourtney Dela FierraNo ratings yet
- Learning and The BrainDocument5 pagesLearning and The BrainBrendan MakidonNo ratings yet
- Uman Hysiology: Endocrine Control of Growth and MetabolismDocument24 pagesUman Hysiology: Endocrine Control of Growth and Metabolismpanairina03026273No ratings yet
- LaughterDocument4 pagesLaughterRizqon Sya'baniNo ratings yet
- AACE Abstracts 2019 Los AngelesDocument357 pagesAACE Abstracts 2019 Los Angelesmimran1974No ratings yet
- Internal Medicine TopicsDocument56 pagesInternal Medicine TopicsBogdan UrichianuNo ratings yet
- Effects of Yoga Practice On Neuroendocrinological ChangesDocument6 pagesEffects of Yoga Practice On Neuroendocrinological ChangesJelly JewelryNo ratings yet
- Adrenal PathophysiologyDocument5 pagesAdrenal PathophysiologyditabokNo ratings yet