You might also like
- Megacolon Toxic of Idiophatic Origin: Case ReportDocument6 pagesMegacolon Toxic of Idiophatic Origin: Case ReportgayutNo ratings yet
- A Case Report of Perforated Primary Follicular Lymphoma of The Jejunum Presenting As Aneurismal FormDocument3 pagesA Case Report of Perforated Primary Follicular Lymphoma of The Jejunum Presenting As Aneurismal FormPeertechz Publications Inc.No ratings yet
- Anggit Triadiana - Full Paper - LNHDocument6 pagesAnggit Triadiana - Full Paper - LNHDolaka CiciyuNo ratings yet
- Colitis EnfisematosaDocument2 pagesColitis EnfisematosaAdriana Gabriela Ugarte MacíasNo ratings yet
- Chronic Lymphocytic LeukemiaFrom EverandChronic Lymphocytic LeukemiaMichael HallekNo ratings yet
- Jurnal Radiologi 1Document4 pagesJurnal Radiologi 1Adelya Dwi AsyifaNo ratings yet
- Ann Oncol 2000 Limfoma ExtranodalDocument4 pagesAnn Oncol 2000 Limfoma ExtranodaldonkeyendutNo ratings yet
- Lymphoma Shofik EDITED BY SAYAM 8.53PMDocument35 pagesLymphoma Shofik EDITED BY SAYAM 8.53PMRAGHU NATH KARMAKERNo ratings yet
- Hodgkins Disease Case StudyDocument7 pagesHodgkins Disease Case StudyLyonsGraham100% (1)
- Case Report and Literature Review On Good's Syndrome, A Form of Acquired Immunodeficiency Associated With ThymomasDocument7 pagesCase Report and Literature Review On Good's Syndrome, A Form of Acquired Immunodeficiency Associated With ThymomasMudassar SattarNo ratings yet
- Lymphoid Lekemia: DR Budi Enoch SPPDDocument32 pagesLymphoid Lekemia: DR Budi Enoch SPPDLia pramitaNo ratings yet
- Non Hodgkin LymphomaDocument9 pagesNon Hodgkin LymphomaAhmad SaifulNo ratings yet
- 14 HF-Limfoma GI TractDocument27 pages14 HF-Limfoma GI TractNur akilaNo ratings yet
- Inflammatory Bowel DiseaseDocument15 pagesInflammatory Bowel DiseaseYanushka Bruce HerathNo ratings yet
- Coli TidesDocument11 pagesColi TidesAndrea Cayufilo CarmonaNo ratings yet
- Classic Versus Type II Enteropathy-Associated T-Cell LymphomaDocument5 pagesClassic Versus Type II Enteropathy-Associated T-Cell Lymphomaderek lauNo ratings yet
- Fundamentals of Colitis: Pergamon International Library of Science, Technology, Engineering and Social StudiesFrom EverandFundamentals of Colitis: Pergamon International Library of Science, Technology, Engineering and Social StudiesNo ratings yet
- Balantidium ColiDocument7 pagesBalantidium ColiOmar GhoneimNo ratings yet
- Colitis, Ulcerative: Whitney D. Lynch Ronald HsuDocument8 pagesColitis, Ulcerative: Whitney D. Lynch Ronald HsuAlexis DF SanchezNo ratings yet
- Advances in Management of NHLDocument34 pagesAdvances in Management of NHLMohammed Abd ElfattahNo ratings yet
- Path Questions (USMLE)Document27 pagesPath Questions (USMLE)Goljan UsmleNo ratings yet
- Neoplasia 6: Dr. Eman Krieshan, M.D. 5-1-2022Document34 pagesNeoplasia 6: Dr. Eman Krieshan, M.D. 5-1-2022MOHA BANATNo ratings yet
- Hodgkin's Lymphoma - LancetDocument9 pagesHodgkin's Lymphoma - LancetSurenderSingh100% (1)
- Pathologyq'sDocument358 pagesPathologyq'sNick JacobNo ratings yet
- Cytophagic Histiocytic Panniculitis, Hemophagocytic Lymphohistiocytosis and Undetermined Autoimmune Disorder: Reconciling The PuzzleDocument5 pagesCytophagic Histiocytic Panniculitis, Hemophagocytic Lymphohistiocytosis and Undetermined Autoimmune Disorder: Reconciling The PuzzleLe DungNo ratings yet
- Histiocytic SarcomaDocument8 pagesHistiocytic SarcomadanishNo ratings yet
- Differentiating Feline Inflammatory Bowel Disease From Alimentary Lymphoma in Duodenal Endoscopic BiopsiesDocument6 pagesDifferentiating Feline Inflammatory Bowel Disease From Alimentary Lymphoma in Duodenal Endoscopic BiopsiesJosé Moreira Lima NetoNo ratings yet
- Childhood Malignancies - Hodgkin's LymphomaDocument6 pagesChildhood Malignancies - Hodgkin's Lymphomavictortayor_26105009No ratings yet
- Chronic Lymphocytic Leukaemia: Key PointsDocument5 pagesChronic Lymphocytic Leukaemia: Key PointsJorge Tovar AvilaNo ratings yet
- Pathology Charts - Answers PDFDocument23 pagesPathology Charts - Answers PDF182 ROHIL HNo ratings yet
- Follicular Cholecystitis With Cholelithiasis A Rare Case ReportDocument3 pagesFollicular Cholecystitis With Cholelithiasis A Rare Case ReportSSR-IIJLS JournalNo ratings yet
- Muto 2020Document5 pagesMuto 2020pamela queirozNo ratings yet
- Art08 PDFDocument10 pagesArt08 PDFEdwin Eloy Sanchez PoloNo ratings yet
- Hodgkein and Nonhodgkein LymphomaDocument57 pagesHodgkein and Nonhodgkein Lymphomasamar yousif mohamedNo ratings yet
- Background: Ormdl3 and of GSDMB Were Significantly Increased in Hrv-Stimulated PBMCSDocument6 pagesBackground: Ormdl3 and of GSDMB Were Significantly Increased in Hrv-Stimulated PBMCSSav GaNo ratings yet
- Soal Hodgkin Nonhodgkin RobbinsDocument4 pagesSoal Hodgkin Nonhodgkin RobbinsAlfian DjaafaraNo ratings yet
- Third Case Report Pseudomembranous Colitis Dr. Lisa FarianiDocument18 pagesThird Case Report Pseudomembranous Colitis Dr. Lisa FarianirizkyauliautamaNo ratings yet
- Atypical Presentation of Pseudomembranous Colitis Localized in Adenomatous PolypsDocument3 pagesAtypical Presentation of Pseudomembranous Colitis Localized in Adenomatous PolypsKiana TehraniNo ratings yet
- 2014 - Lecture - Pathology of The Small and Large IntestineDocument12 pages2014 - Lecture - Pathology of The Small and Large IntestinesammysandsongNo ratings yet
- Severe Systemic Cytomegalovirus Infection in An Immunocompetent Patient Outside The Intensive Care Unit: A Case ReportDocument4 pagesSevere Systemic Cytomegalovirus Infection in An Immunocompetent Patient Outside The Intensive Care Unit: A Case ReportSebastián Garay HuertasNo ratings yet
- An Sell 2005Document11 pagesAn Sell 2005Rachel AutranNo ratings yet
- Medicine Seminar Combined-1Document30 pagesMedicine Seminar Combined-1Deepanshu KumarNo ratings yet
- Jurnal MelenaDocument4 pagesJurnal MelenaMadetolis PhotoworksNo ratings yet
- Manejo en Colangitis Aguda - Libro XDocument4 pagesManejo en Colangitis Aguda - Libro XRodrigo MartinezNo ratings yet
- An Unresectable Klatskin's Tumor?: Johannes Hartl, Tobias Werner, and Christoph SchrammDocument2 pagesAn Unresectable Klatskin's Tumor?: Johannes Hartl, Tobias Werner, and Christoph SchrammLourdes MollardNo ratings yet
- Linteret de Lileo-Coloscopie Dans Le Bilan Dextension Du Lymphome GastriqueDocument5 pagesLinteret de Lileo-Coloscopie Dans Le Bilan Dextension Du Lymphome GastriqueIJAR JOURNALNo ratings yet
- Radiology Case Report - Splenic AbscessDocument6 pagesRadiology Case Report - Splenic AbscessAbeebNo ratings yet
- Case Report: Streptococcus AnginosusDocument4 pagesCase Report: Streptococcus AnginosusIesanu MaraNo ratings yet
- Caz Bun 3Document7 pagesCaz Bun 3Dumitru RadulescuNo ratings yet
- A Case of Persistent Bloody DiarrhoeaDocument9 pagesA Case of Persistent Bloody DiarrhoeaRuhama ErmiasNo ratings yet
- Ulcerative Colitis: Pathogenesis & PathologyDocument12 pagesUlcerative Colitis: Pathogenesis & PathologyironNo ratings yet
- Approach To Patients With LymphadenopathyDocument5 pagesApproach To Patients With LymphadenopathyAngela Mitchelle NyanganNo ratings yet
- A Me Bias IsDocument5 pagesA Me Bias IsRavinder NainawatNo ratings yet
- Written Case StudyDocument16 pagesWritten Case Studyapi-234402582No ratings yet
- Seminario 2Document7 pagesSeminario 2andreaNo ratings yet
- KMJ 34 78Document5 pagesKMJ 34 78Faril RahmaNo ratings yet
- Frankhouse 2021Document11 pagesFrankhouse 2021marta idziakNo ratings yet
- Primary Mantle Cell Lymphoma of The Tonsil: An Uncommon CaseDocument4 pagesPrimary Mantle Cell Lymphoma of The Tonsil: An Uncommon Casevam buddhaNo ratings yet
- 10 11648 J CRJ 20200802 14Document3 pages10 11648 J CRJ 20200802 14Marj MendezNo ratings yet
- A Series of Catastrophes and MiraclesDocument9 pagesA Series of Catastrophes and Miracleswamu8850% (1)
- Gastrointestinal Oncology Principles and PracticesDocument794 pagesGastrointestinal Oncology Principles and Practicesjohny3333No ratings yet
- Tugas Terstruktur Day 2 StudentsDocument17 pagesTugas Terstruktur Day 2 StudentsAurellia ShafitriNo ratings yet
- 1 s2.0 S209379112300063X MainDocument8 pages1 s2.0 S209379112300063X Mainshoshanasingh52No ratings yet
- Studi Kasus Teori Pemodelan SistemDocument14 pagesStudi Kasus Teori Pemodelan SistemRenaldo Yoku100% (1)
- Lecture9-Nutrition and CancerDocument65 pagesLecture9-Nutrition and Cancermirabel IvanaliNo ratings yet
- Intl J Gynecology Obste - 2021 - OlawaiyeDocument12 pagesIntl J Gynecology Obste - 2021 - OlawaiyeKalaivathanan VathananNo ratings yet
- LeukemiaDocument1 pageLeukemiamarto langNo ratings yet
- Terapi CMLDocument7 pagesTerapi CMLAnnisa Dwi AndrianiNo ratings yet
- Unapproved Covid VaccineDocument57 pagesUnapproved Covid VaccineKenny Lynch100% (3)
- EAPP q1 Mod3 Thesis Statement Colal v3Document20 pagesEAPP q1 Mod3 Thesis Statement Colal v3Marilou T. Makil SolisNo ratings yet
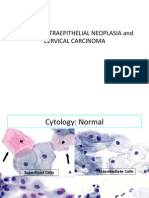
- 04 CIN and Cervical Cancer UNEDITEDDocument120 pages04 CIN and Cervical Cancer UNEDITEDRalph JuicoNo ratings yet
- 2018 NYC Marathon TeamDocument9 pages2018 NYC Marathon TeamAnonymous kTzxI9NNo ratings yet
- Chapter 1 Cucumber, Apple, CeleryDocument12 pagesChapter 1 Cucumber, Apple, CeleryAnis AdilahNo ratings yet
- Cancer & Massage Therapy - Part 1Document15 pagesCancer & Massage Therapy - Part 1Mya AlissandraNo ratings yet
- YES-INUIT GOT CANCER. PALEO NOW DEBUNKED. WESTON PRICE DEBUNKED - Inuit Greenland Mummies Confirmed Infested With Carcinoma, Bone Disease, Birth Defects, Lice, And Parasites, While on Wholly Native Meat Based Primal Natural Paleolithic DietDocument1 pageYES-INUIT GOT CANCER. PALEO NOW DEBUNKED. WESTON PRICE DEBUNKED - Inuit Greenland Mummies Confirmed Infested With Carcinoma, Bone Disease, Birth Defects, Lice, And Parasites, While on Wholly Native Meat Based Primal Natural Paleolithic DietFRAUDWATCHCOMMISSIONNo ratings yet
- Nursing Care Plan For Breast Cancer NCP PDFDocument2 pagesNursing Care Plan For Breast Cancer NCP PDFMaina BarmanNo ratings yet
- Synthesis, Characterization and Biological Activity of Antimony (III)Document15 pagesSynthesis, Characterization and Biological Activity of Antimony (III)inoka911No ratings yet
- M 2Document8 pagesM 2Aijem RyanNo ratings yet
- Benign High Risk and Premalignant Lesions of The BreastDocument17 pagesBenign High Risk and Premalignant Lesions of The BreastjanetaNo ratings yet
- Lesson: Dr. Leon Hammer, M.DDocument14 pagesLesson: Dr. Leon Hammer, M.DRocío JMNo ratings yet
- Urological Cancer Clinical ScenariosDocument27 pagesUrological Cancer Clinical ScenariosMohammed FathyNo ratings yet
- Nance Evolution of Pap Testing at A Community Hospital A Ten Year ExperienceDocument6 pagesNance Evolution of Pap Testing at A Community Hospital A Ten Year ExperienceSok Ling YeeNo ratings yet
- Thyroid NodulesDocument7 pagesThyroid NodulesPravat SatpathyNo ratings yet
- Pancreatic Cystic Lesions English 2019Document25 pagesPancreatic Cystic Lesions English 2019Worku KifleNo ratings yet
- Retroperitoneal and Pelvic MassesDocument61 pagesRetroperitoneal and Pelvic MassesChris FrenchNo ratings yet
- Wallach Mineral-DeficiencysDocument11 pagesWallach Mineral-Deficiencyshaskellb572093% (15)
- The Enzyme Treatment of Cancer - John Beard 1911Document156 pagesThe Enzyme Treatment of Cancer - John Beard 1911Trombonino100% (18)
- Original PDF Voice Disorders Third Edition 3rd Edition PDFDocument41 pagesOriginal PDF Voice Disorders Third Edition 3rd Edition PDFclarence.barcia711100% (40)
- Health Facility and Humanresource Factors Supporting Uptake of Cervical Cancer Screening in Kakamega County, KenyaDocument7 pagesHealth Facility and Humanresource Factors Supporting Uptake of Cervical Cancer Screening in Kakamega County, KenyaIJAR JOURNALNo ratings yet