You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- CY 2022 2024 DOH Devolution Transition PlanDocument480 pagesCY 2022 2024 DOH Devolution Transition PlanThata Thata100% (2)
- Designing of Clinical Study DocumentsDocument16 pagesDesigning of Clinical Study DocumentsSaranya Smiley100% (1)
- (PMLS) Defining Medical Technology ProfessionDocument3 pages(PMLS) Defining Medical Technology ProfessionBanana BananaNo ratings yet
- Evidenced Based PracticesDocument12 pagesEvidenced Based PracticesCHRISTINE JOY. MOLINANo ratings yet
- 2021 American College of Rheumatology Guideline For The Treatment of Rheumatoid ArthritisDocument30 pages2021 American College of Rheumatology Guideline For The Treatment of Rheumatoid Arthritisjose pablo quero reyesNo ratings yet
- The Pathogenesis of Rheumatoid ArthritisDocument15 pagesThe Pathogenesis of Rheumatoid Arthritisjose pablo quero reyesNo ratings yet
- Diferentiation and Diagnosis of JaundiceDocument9 pagesDiferentiation and Diagnosis of Jaundicejose pablo quero reyesNo ratings yet
- Updates in ANCA-associated VasculitisDocument14 pagesUpdates in ANCA-associated Vasculitisjose pablo quero reyesNo ratings yet
- Cost-Related Prescription Non-Adherence and Patient-Reported Outcomes in Systemic Lupus Erythematosus: The Michigan LupusDocument9 pagesCost-Related Prescription Non-Adherence and Patient-Reported Outcomes in Systemic Lupus Erythematosus: The Michigan Lupusjose pablo quero reyesNo ratings yet
- Effect of Pepermint OilDocument7 pagesEffect of Pepermint OilKuro chanNo ratings yet
- Philhealth: Romeo R. Andaya, MD - MSCPD, PHD, Fpafp Chair, DPMCHDocument19 pagesPhilhealth: Romeo R. Andaya, MD - MSCPD, PHD, Fpafp Chair, DPMCHKatNo ratings yet
- CE-marking: Medical and Health Service, ASEAN Tüv Süd PSBDocument8 pagesCE-marking: Medical and Health Service, ASEAN Tüv Süd PSBDuc Nguyen ManhNo ratings yet
- HEARS Field Report 04.16.19Document1 pageHEARS Field Report 04.16.19HEMB BATMCNo ratings yet
- ILBS Recruitment Advertisement Nov 2018Document3 pagesILBS Recruitment Advertisement Nov 2018Roy ANo ratings yet
- (2018) - The Lancet Commission On Global Mental Health and Sustainable Development. The Lancet.Document46 pages(2018) - The Lancet Commission On Global Mental Health and Sustainable Development. The Lancet.Aarón ParedesNo ratings yet
- CV Elective Program For International StudentsDocument5 pagesCV Elective Program For International StudentsYosafatPrasetyadiNo ratings yet
- The Impact of The Pandemic On Neurosurgical Services A Study From A Coronavirus Disease 2019 Referral Hospital in SurakartaDocument5 pagesThe Impact of The Pandemic On Neurosurgical Services A Study From A Coronavirus Disease 2019 Referral Hospital in SurakartaPradhi BaliNo ratings yet
- COVID-19 or Not COVID-19 - Compared Characteristics of Patients Hospitalized For Suspected COVID-19Document6 pagesCOVID-19 or Not COVID-19 - Compared Characteristics of Patients Hospitalized For Suspected COVID-19naqibsakila4286No ratings yet
- Health Systems Lifestyle PoliciesDocument455 pagesHealth Systems Lifestyle PoliciesLMNo ratings yet
- Dental Caries Experience and Oral Health Related Quality of Life in Working AdultsDocument8 pagesDental Caries Experience and Oral Health Related Quality of Life in Working AdultsArida BitanajshaNo ratings yet
- ICN Code of EthicsDocument12 pagesICN Code of Ethicsakhimoloos100% (1)
- SotonomuxoxumusolijomakigDocument2 pagesSotonomuxoxumusolijomakigJake BallNo ratings yet
- HC776Document4 pagesHC776Dawn CasuncadNo ratings yet
- JIT at Arnold Palmer HospitalDocument1 pageJIT at Arnold Palmer HospitalAparajita SinghNo ratings yet
- Neonatal Emergency LaparotomyDocument5 pagesNeonatal Emergency LaparotomyJoilson TravassosNo ratings yet
- Tinjauan Sistematis Instrumen Kualitas Hidup Pada Penderita Kanker Payudara Jangka Panjang - EnGLISHDocument15 pagesTinjauan Sistematis Instrumen Kualitas Hidup Pada Penderita Kanker Payudara Jangka Panjang - EnGLISHJihan Dini PramestiNo ratings yet
- AmysaDocument14 pagesAmysaawanisfauzi90No ratings yet
- Digital Drugs An Anatomy of New Medicines PDFDocument27 pagesDigital Drugs An Anatomy of New Medicines PDFshraddha5jNo ratings yet
- Total Dental Surgeons Are Listed in Drdata Directory: NavigationDocument11 pagesTotal Dental Surgeons Are Listed in Drdata Directory: Navigationvivek kumarNo ratings yet
- Patients' Bill of Rights: ATTY. Misheena Joyce C. Tiatco Practicing LawyerDocument54 pagesPatients' Bill of Rights: ATTY. Misheena Joyce C. Tiatco Practicing LawyerMJ CarreonNo ratings yet
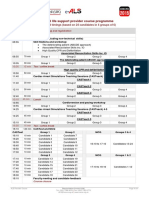
- E-ALS Programme IO ARS (March 2016)Document1 pageE-ALS Programme IO ARS (March 2016)Florentina GasttiNo ratings yet
- Nursing Foundation Harinderjeet GoyalDocument31 pagesNursing Foundation Harinderjeet Goyalmanrajghumman555No ratings yet
- 9400215141: Patient ID 94009314 Sid No Tirur Branch Ms. THASNIYA 273864Document1 page9400215141: Patient ID 94009314 Sid No Tirur Branch Ms. THASNIYA 273864Abdul LatheefNo ratings yet
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary DetailsANILNo ratings yet
- DapusDocument1 pageDapusJihadNo ratings yet