You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Diagnostic Tests To Determine Phase of Acute or Chronic HBVDocument1 pageDiagnostic Tests To Determine Phase of Acute or Chronic HBVadityoNo ratings yet
- Journal Pone 0269233Document9 pagesJournal Pone 0269233adityoNo ratings yet
- Diagnostic Approach To Children and Adolescents With Short Stature - UpToDateDocument30 pagesDiagnostic Approach To Children and Adolescents With Short Stature - UpToDateadityoNo ratings yet
- Twin Pregnancy: Prenatal Issues - UpToDateDocument70 pagesTwin Pregnancy: Prenatal Issues - UpToDateadityoNo ratings yet
- Au Bard 1999Document9 pagesAu Bard 1999adityoNo ratings yet
- Epilepsy in PregnancyDocument52 pagesEpilepsy in PregnancyadityoNo ratings yet
- Highlights: Data As Of: 01 July 2020Document22 pagesHighlights: Data As Of: 01 July 2020adityoNo ratings yet
- MAPPING Ginekologi Onkologi 22-05-2018Document7 pagesMAPPING Ginekologi Onkologi 22-05-2018adityoNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Korean Lesson 1Document12 pagesKorean Lesson 1Ivett97No ratings yet
- Carbanions Carbocations and CarboradicalsDocument21 pagesCarbanions Carbocations and CarboradicalsAnaAmaruNo ratings yet
- Unit Iv Ce 6405Document13 pagesUnit Iv Ce 6405HanafiahHamzahNo ratings yet
- Determinants of Income InequalityDocument30 pagesDeterminants of Income InequalityKorawit Booranakit100% (1)
- HyperMILL Readme enDocument20 pagesHyperMILL Readme enjimNo ratings yet
- Concrete Mix DesignDocument11 pagesConcrete Mix DesignV Vinoth Edac100% (1)
- Squall (Better) Training Manual: ModelsDocument83 pagesSquall (Better) Training Manual: ModelsSilomo-saka MambaNo ratings yet
- Yohimbine InjectionDocument1 pageYohimbine InjectionKasidit SornchaiNo ratings yet
- DPP 01 Periodic Table JH Sir-3576 PDFDocument5 pagesDPP 01 Periodic Table JH Sir-3576 PDFChessNo ratings yet
- Band Gaps and Electronics Structure of PerovskitesDocument12 pagesBand Gaps and Electronics Structure of PerovskitesThanh Long TaNo ratings yet
- Periodic Table of ElementsDocument60 pagesPeriodic Table of ElementsruchitlpatelNo ratings yet
- 10) C2 Trigonometrical Identities and Equations QuestionsDocument26 pages10) C2 Trigonometrical Identities and Equations QuestionsBoxOneTwoNo ratings yet
- Simple MachinesDocument25 pagesSimple MachinesMay ArispeNo ratings yet
- 5510 0004 04 - 18 1021 Basic Principles of Ship Propulsion - MAN PDFDocument68 pages5510 0004 04 - 18 1021 Basic Principles of Ship Propulsion - MAN PDFAlex FatecNo ratings yet
- V-Ray For SketchUp Rendering An Exterior Scene PDFDocument7 pagesV-Ray For SketchUp Rendering An Exterior Scene PDFDevohNo ratings yet
- Abbott 2021 ApJL 915 L5Document24 pagesAbbott 2021 ApJL 915 L5Manju SanthakumariNo ratings yet
- Electric Power Applications, Engine & Generator SizingDocument120 pagesElectric Power Applications, Engine & Generator SizingDIPPOSNo ratings yet
- IP03 Loops-4slides PDFDocument10 pagesIP03 Loops-4slides PDFRamesh GNo ratings yet
- ACPS CP S1 01 FDA SlidesDocument78 pagesACPS CP S1 01 FDA SlidesBlueSagaNo ratings yet
- Lab ReportDocument5 pagesLab Reportivan glenn baldomerostNo ratings yet
- Microstructure Characteristics and Performance of Dissimilar Welds Between Magnesium Alloy and Aluminum Formed by Friction StirringDocument5 pagesMicrostructure Characteristics and Performance of Dissimilar Welds Between Magnesium Alloy and Aluminum Formed by Friction StirringLeidy Silvana Chacón VelascoNo ratings yet
- E Rich Burn Control System: With Stablesense™ TechnologyDocument4 pagesE Rich Burn Control System: With Stablesense™ TechnologyYasir JamilNo ratings yet
- Part 1Document120 pagesPart 1Raju Halder0% (1)
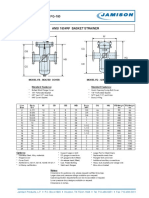
- FB-150 FQ-150 Basket StrainerDocument1 pageFB-150 FQ-150 Basket Strainerklich77No ratings yet
- Microsoft WordDocument79 pagesMicrosoft Wordthamel_09No ratings yet
- MCAT Uhs Past Paper (2008-2016)Document180 pagesMCAT Uhs Past Paper (2008-2016)Abdullah SheikhNo ratings yet
- Adjectives 4Document34 pagesAdjectives 4Delia Bolasoc100% (1)
- Sentiment AnalysisDocument5 pagesSentiment AnalysisShruti PantNo ratings yet
- Crane Wheels-General InformationDocument3 pagesCrane Wheels-General InformationArvind VaishNo ratings yet
- Welding of Thermoplastics Heated Tool Butt Welding Directive DVS 2207-25Document7 pagesWelding of Thermoplastics Heated Tool Butt Welding Directive DVS 2207-25Yuriy Nechaevskiy100% (1)