You might also like
- 05 De Stavola 등 - 2021 - The Vestibular Shifted Flap Design for Vertical BoDocument9 pages05 De Stavola 등 - 2021 - The Vestibular Shifted Flap Design for Vertical Bosupercool0120No ratings yet
- The SAC Classification in Implant Dentistry 2nd Edition OriginalDocument289 pagesThe SAC Classification in Implant Dentistry 2nd Edition OriginalTheo_96No ratings yet
- Parte 3Document21 pagesParte 3chaps1995No ratings yet
- Pacquet2022 - Therapeutic Strategy For Cracked TeethDocument17 pagesPacquet2022 - Therapeutic Strategy For Cracked TeethJosé Ramón CuetoNo ratings yet
- Autotransplantation of Teeth PDFDocument196 pagesAutotransplantation of Teeth PDFChristian Torres100% (2)
- Integrated Esthetics in Periodontics and ImplantologyDocument818 pagesIntegrated Esthetics in Periodontics and ImplantologyThanh Nhan DinhNo ratings yet
- Oral Implantology Review A Study Guide, 2nd EditionDocument274 pagesOral Implantology Review A Study Guide, 2nd EditionThu Phuong NguyenNo ratings yet
- Anterior Veneer Restorations An Evidence-Based Minimal-Intervention PerspectiveDocument20 pagesAnterior Veneer Restorations An Evidence-Based Minimal-Intervention PerspectiveAlex Gutierrez AcostaNo ratings yet
- The Osteoperiosteal Flap: A Simplified Approach to Alveolar Bone ReconstructionFrom EverandThe Osteoperiosteal Flap: A Simplified Approach to Alveolar Bone ReconstructionRating: 4 out of 5 stars4/5 (1)
- Open-Bite Malocclusion: Treatment and StabilityFrom EverandOpen-Bite Malocclusion: Treatment and StabilityGuilherme JansonRating: 5 out of 5 stars5/5 (1)
- 2021 The Esthetic Biological Contour Concept For Implant RestorationDocument12 pages2021 The Esthetic Biological Contour Concept For Implant RestorationOd. Valeria Gutierrez G100% (3)
- Carvalho Et Al 2021 IJEDDocument19 pagesCarvalho Et Al 2021 IJEDclaudiaNo ratings yet
- PSCP Tables (MDRRMO Accomplished Table)Document11 pagesPSCP Tables (MDRRMO Accomplished Table)Chelsie Barbonio OnoyaNo ratings yet
- (IJPRD) GLUCKMAN 2017 - Partial Extraction Therapies Part 2 PDFDocument11 pages(IJPRD) GLUCKMAN 2017 - Partial Extraction Therapies Part 2 PDFFelipeGuzanskyMilaneziNo ratings yet
- Defectos Óseos - Diagnóstico Radiográfico"Document101 pagesDefectos Óseos - Diagnóstico Radiográfico"Nucleo AlgodonesNo ratings yet
- 2020 Emergence Profile Guidelines PDFDocument11 pages2020 Emergence Profile Guidelines PDFDiego Alejandro Cortés Linares100% (2)
- 7 Principles of Uncomplicated ExodontiaDocument43 pages7 Principles of Uncomplicated Exodontiaray774432No ratings yet
- Implant Failures - Part ADocument46 pagesImplant Failures - Part ADrIbrahimShaikh100% (3)
- Managing The Unstable CDDocument8 pagesManaging The Unstable CDNajeeb UllahNo ratings yet
- Treatment Planning Single Maxillary Anterior Implants for DentistsFrom EverandTreatment Planning Single Maxillary Anterior Implants for DentistsNo ratings yet
- Dental Implant Treatment Planning for New Dentists Starting Implant TherapyFrom EverandDental Implant Treatment Planning for New Dentists Starting Implant TherapyRating: 4 out of 5 stars4/5 (1)
- RecessionsDocument68 pagesRecessionsmaryamNo ratings yet
- @dentistinfoDocument266 pages@dentistinfoArnont YindeesugNo ratings yet
- Ebooks 10 Tips ImplantologyDocument16 pagesEbooks 10 Tips ImplantologylupusebastianNo ratings yet
- Artículo Khoury2018Document10 pagesArtículo Khoury2018Basma Derdabi100% (1)
- Densah Bur Surgical Technique ManualDocument44 pagesDensah Bur Surgical Technique ManualLuis Felipe50% (2)
- Periodontology 2000 - 2023 - Urban - Minimal Invasiveness in Vertical Ridge AugmentationDocument19 pagesPeriodontology 2000 - 2023 - Urban - Minimal Invasiveness in Vertical Ridge AugmentationLEONARDO ALBERTO CRESPIN ZEPEDANo ratings yet
- Periosteal Pocket Flap For Horizontal Bone RegenerDocument10 pagesPeriosteal Pocket Flap For Horizontal Bone RegenerViorel Ion100% (1)
- Case Selection in Dental Implant TherapyDocument4 pagesCase Selection in Dental Implant Therapymichealraj rousseauNo ratings yet
- UntitledDocument70 pagesUntitledPerebyinis PavloNo ratings yet
- A Guide To Implant Dentistry Part 2 Surgical and Prosthodontic ConsiderationsDocument7 pagesA Guide To Implant Dentistry Part 2 Surgical and Prosthodontic ConsiderationsPhú VinhNo ratings yet
- "Rules of Six"-: EbookDocument13 pages"Rules of Six"-: EbookElsa Fernanda Villegas JiménezNo ratings yet
- Bone Management in Dental Implantology by Andi Setiawan BudihardjaDocument15 pagesBone Management in Dental Implantology by Andi Setiawan Budihardjabuccal100% (1)
- Full-Mouth Rehabilitation of A Severe Tooth Wear Case: A Digital, Esthetic and Functional ApproachDocument22 pagesFull-Mouth Rehabilitation of A Severe Tooth Wear Case: A Digital, Esthetic and Functional Approachjose figueroaNo ratings yet
- The Early Causes of Crestal Bone Loss Around Dental ImplantDocument64 pagesThe Early Causes of Crestal Bone Loss Around Dental ImplantVijay SinghNo ratings yet
- Full Mouth Rehabilitation With Zygomatic Implants in Patients JCDocument28 pagesFull Mouth Rehabilitation With Zygomatic Implants in Patients JCsapnaNo ratings yet
- Implant Occlusion Articles AbstractDocument4 pagesImplant Occlusion Articles AbstractMrunal DoiphodeNo ratings yet
- Biomimetic (Latest)Document127 pagesBiomimetic (Latest)Pawee PiyasowanNo ratings yet
- Implant Failure and Their ManagementDocument61 pagesImplant Failure and Their ManagementDharshiniNo ratings yet
- Creating Veneer Provisionals Using Silicone Matrices and Models by DentistryDocument11 pagesCreating Veneer Provisionals Using Silicone Matrices and Models by Dentistrycesar amaro100% (1)
- Restorative Quick Guide: All-On-4® Treatment ConceptDocument17 pagesRestorative Quick Guide: All-On-4® Treatment ConceptStanislav StrîșcaNo ratings yet
- Principles of Designing Mucoperiosteal FlapsDocument70 pagesPrinciples of Designing Mucoperiosteal FlapsStephen KinyanjuiNo ratings yet
- A Biometric Approach To Aesthetic Crown LengtheningDocument11 pagesA Biometric Approach To Aesthetic Crown LengtheningpercycgNo ratings yet
- Immediate Loading FaizDocument85 pagesImmediate Loading FaizDrrksundar KumarNo ratings yet
- The Ideal Restoration of Endodontically Treated Teeth Structural and Esthetic Considerations A Review of The Literature and Clinical Guidelines For The Restorative ClinicianDocument31 pagesThe Ideal Restoration of Endodontically Treated Teeth Structural and Esthetic Considerations A Review of The Literature and Clinical Guidelines For The Restorative ClinicianLuis Alberto Carpio MorenoNo ratings yet
- J Adh Dent 2020 Effective Protocol For Daily High-Quality Direct Posterior Composite Restorations. Cavity Preparation and DesignDocument18 pagesJ Adh Dent 2020 Effective Protocol For Daily High-Quality Direct Posterior Composite Restorations. Cavity Preparation and DesignCesar Loyola SanchezNo ratings yet
- 2017 Implant Aesthetics - Keys To Diagnosis and TreatmentDocument453 pages2017 Implant Aesthetics - Keys To Diagnosis and TreatmentbetsaNo ratings yet
- UntitledDocument122 pagesUntitledfrancisco EscorciaNo ratings yet
- Anterior Open BiteDocument7 pagesAnterior Open BiteGowriNo ratings yet
- Urban 2016 Técnica de La SalchichaDocument8 pagesUrban 2016 Técnica de La SalchichaLukas Lopez RamirezNo ratings yet
- 2 Nonsurgical Periodontal Therapy - Pocket DentistryDocument14 pages2 Nonsurgical Periodontal Therapy - Pocket DentistryRizki OktavianiNo ratings yet
- The 17 Immutable Laws in Implant DentistryDocument70 pagesThe 17 Immutable Laws in Implant DentistrymedNo ratings yet
- Ebook: Zirconia: Facts and MisconceptionsDocument9 pagesEbook: Zirconia: Facts and MisconceptionsCaglarBursaNo ratings yet
- Basic Surgical Techniques For Endosseous Implant PlacementDocument101 pagesBasic Surgical Techniques For Endosseous Implant PlacementAnshuman Dwivedi100% (2)
- Implant Surgical AnatomyDocument14 pagesImplant Surgical AnatomyKo YotoNo ratings yet
- Iñaki Gamborena, DMD, MSD, Fid Yoshihiro Sasaki, CDT Markus B. Blatz, DMD, PHDDocument15 pagesIñaki Gamborena, DMD, MSD, Fid Yoshihiro Sasaki, CDT Markus B. Blatz, DMD, PHDKyoko CP100% (1)
- Model Guided Soft Tissue AugmentationDocument10 pagesModel Guided Soft Tissue AugmentationPedro Amaral100% (2)
- Ridge AugmentationDocument109 pagesRidge AugmentationSingh Jyoti100% (3)
- BernottiDocument44 pagesBernottiAlexandra Alexandra100% (2)
- WorkflowDocument2 pagesWorkflowAnirban MullickNo ratings yet
- EigrpDocument26 pagesEigrpChidanandaNo ratings yet
- Lee Chee Kwong v. Kutiandy Thanniamalay & AnorDocument16 pagesLee Chee Kwong v. Kutiandy Thanniamalay & AnorC.Y. Ong & Co. - Adv. & Sol.No ratings yet
- Flat Slab - Types of Flat Slab Design and Its AdvantagesDocument7 pagesFlat Slab - Types of Flat Slab Design and Its AdvantagesnandanaNo ratings yet
- Eaton DCF800 FilterDocument2 pagesEaton DCF800 Filterkyle100% (1)
- Inverter Design: 12 V 1000 W Inverter SpesificationsDocument3 pagesInverter Design: 12 V 1000 W Inverter SpesificationsAlfiyan MaulanaNo ratings yet
- CHAPTER 12 Roles and Competencies of School HeadsDocument5 pagesCHAPTER 12 Roles and Competencies of School HeadsRoxanne Joy A. TrillanesNo ratings yet
- Metaverse Presentation - CopieDocument30 pagesMetaverse Presentation - Copiem.e.r.m.2024No ratings yet
- Leancafe09 SlidesDocument64 pagesLeancafe09 SlidesTon DorchainNo ratings yet
- Market ResearchDocument19 pagesMarket ResearchClarck DioncoNo ratings yet
- Hurricane Ultra II Data Sheet PDFDocument1 pageHurricane Ultra II Data Sheet PDFCarlos CubasNo ratings yet
- Group 3 - Core of SciencesDocument10 pagesGroup 3 - Core of Sciencesapi-557677480No ratings yet
- Deploy Flask App With Nginx Using Gunicorn - Faun - MediumDocument6 pagesDeploy Flask App With Nginx Using Gunicorn - Faun - MediumFolha ChaNo ratings yet
- Openings Amateurs PDFDocument461 pagesOpenings Amateurs PDFjold100% (1)
- STR1 041 3 PDFDocument3 pagesSTR1 041 3 PDFMouhamadou yassineNo ratings yet
- Educ-4 - Facilitating Learner-Centered Teaching-Manayon-ActivityDocument1 pageEduc-4 - Facilitating Learner-Centered Teaching-Manayon-ActivityMYLE MANAYONNo ratings yet
- Guidelines For Maxillary Incisal Edge Position A Pilot Study The Key Is The Canine J Prosthodont 2007Document5 pagesGuidelines For Maxillary Incisal Edge Position A Pilot Study The Key Is The Canine J Prosthodont 2007Iulia Florina SimaNo ratings yet
- Ambient CommunicationsDocument19 pagesAmbient CommunicationsMaria Anna M LegaspiNo ratings yet
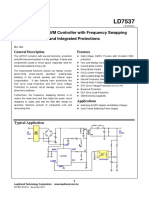
- LD 7537 - Controlador PWMDocument16 pagesLD 7537 - Controlador PWMTiago LeonhardtNo ratings yet
- Module 2Document7 pagesModule 2Fiona Belle DaganteNo ratings yet
- Action Plan in WatchDocument1 pageAction Plan in WatchCharycel de GuzmanNo ratings yet
- Ata 34 Navigation 1Document139 pagesAta 34 Navigation 1omarmasaquizaNo ratings yet
- Audit Data Analytics To Traditional Procedures Mapping DocumentDocument549 pagesAudit Data Analytics To Traditional Procedures Mapping DocumentMuhammadChaerulTammimiNo ratings yet
- LV Motor Starting & ProtectionDocument10 pagesLV Motor Starting & ProtectionContract 42154No ratings yet
- Hell On Earth - Arch - Children O' The AtomDocument129 pagesHell On Earth - Arch - Children O' The AtomEvgeny Petrov100% (1)
- 1 Concept Paper On The 6-Year CurriculumDocument9 pages1 Concept Paper On The 6-Year CurriculumJoseph Tabadero Jr.100% (3)
- US1994497 - Indicator - Winters For Gladwin, 1935Document5 pagesUS1994497 - Indicator - Winters For Gladwin, 1935devheadbotNo ratings yet
- Danone PMDocument9 pagesDanone PMnghia_ho_15No ratings yet
- Blank Communication Letter For TeachersDocument18 pagesBlank Communication Letter For TeachersEJZIRUNo ratings yet