You might also like
- 2 Myasthenia Gravis and MS 2Document50 pages2 Myasthenia Gravis and MS 2Rawbeena RamtelNo ratings yet
- Miastenia GravisDocument28 pagesMiastenia Gravismariateresajijon7No ratings yet
- Myasthenia Gravis and Lambert-Eaton Myasthenic Syndrome - Continuum December 2016Document28 pagesMyasthenia Gravis and Lambert-Eaton Myasthenic Syndrome - Continuum December 2016Habib G. Moutran BarrosoNo ratings yet
- Motor Endplate Disorders Myasthenia Gravis Overview and DefinitionDocument4 pagesMotor Endplate Disorders Myasthenia Gravis Overview and DefinitionPJHGNo ratings yet
- 51.differential Diagnosis of Myasthenia Gravis - A ReviewDocument11 pages51.differential Diagnosis of Myasthenia Gravis - A ReviewSeptime TyasNo ratings yet
- Myasthenia Gravis Anesthetic Implications and ManagementDocument31 pagesMyasthenia Gravis Anesthetic Implications and Managementaashish45No ratings yet
- Review: Myasthenic CrisisDocument11 pagesReview: Myasthenic CrisisRaisha TriasariNo ratings yet
- RJN 2017 2 Art-04Document3 pagesRJN 2017 2 Art-04Ana GabrielaNo ratings yet
- Myasthenia Gravis and Other Neuromuscular Junction DisordersDocument8 pagesMyasthenia Gravis and Other Neuromuscular Junction Disordersidno1008No ratings yet
- Myasthenia Gravis: A Review: Hideyuki Matsumoto, MD, PHD and Yoshikazu Ugawa, MD, PHDDocument7 pagesMyasthenia Gravis: A Review: Hideyuki Matsumoto, MD, PHD and Yoshikazu Ugawa, MD, PHDZainal AbidinNo ratings yet
- Neuromuscular Junction DisordersDocument32 pagesNeuromuscular Junction Disordersepic sound everNo ratings yet
- L 7 ANESTHESIS Myasthenia GravisDocument20 pagesL 7 ANESTHESIS Myasthenia Graviskatherinerance331No ratings yet
- Myesthenia Gravis MedscapeDocument8 pagesMyesthenia Gravis MedscapeSarah OvinithaNo ratings yet
- Bja MGDocument6 pagesBja MGVignesh VenkatesanNo ratings yet
- Referat MG Desya BismillahDocument20 pagesReferat MG Desya BismillahDesya BillaNo ratings yet
- Myasthenia Gravis: Assoc. Prof. Dr. Rodica BălașaDocument31 pagesMyasthenia Gravis: Assoc. Prof. Dr. Rodica BălașaIstván MáthéNo ratings yet
- Neuromuscular DisordersDocument3 pagesNeuromuscular DisordersMaharaniDewiNo ratings yet
- Source 3Document3 pagesSource 3PJHGNo ratings yet
- Neuromuscular Junction DisorderDocument10 pagesNeuromuscular Junction DisorderZosmita Shane GalgaoNo ratings yet
- Myasthenia Gravis Lecture 12Document59 pagesMyasthenia Gravis Lecture 12Pop D. MadalinaNo ratings yet
- Myasthenia GravisDocument11 pagesMyasthenia GravisParvathy RNo ratings yet
- Presented By: VIVEK DEVDocument38 pagesPresented By: VIVEK DEVFranchesca LugoNo ratings yet
- Myasthenia GravisDocument17 pagesMyasthenia GravisYanski DarmantoNo ratings yet
- Jurnal Trigeminal Neuralgia 1Document12 pagesJurnal Trigeminal Neuralgia 1nabilla putriNo ratings yet
- MyasteniaDocument7 pagesMyastenialmcarmonaNo ratings yet
- Lambru2021 2Document12 pagesLambru2021 2Deyvid CapeloNo ratings yet
- MG Desya BismillahDocument20 pagesMG Desya BismillahDesya BillaNo ratings yet
- Myasthenia Gravis in Clinical Practice: Miastenia Gravis Na Prática ClínicaDocument9 pagesMyasthenia Gravis in Clinical Practice: Miastenia Gravis Na Prática ClínicaMasDhedotNo ratings yet
- Myasthenia Gravis ReferenceDocument19 pagesMyasthenia Gravis ReferenceIka Wulan PermataNo ratings yet
- Trigeminal Neuralgia - A Practical GuideDocument12 pagesTrigeminal Neuralgia - A Practical Guide전영우No ratings yet
- Myastenia Gravis PDFDocument7 pagesMyastenia Gravis PDFAdrian CiurciunNo ratings yet
- MG 2Document5 pagesMG 2vaishnaviNo ratings yet
- Anaesthesia For Children WithDocument5 pagesAnaesthesia For Children Withnanang hidayatullohNo ratings yet
- Debilidad Muscular en UciDocument16 pagesDebilidad Muscular en UcipakokorreaNo ratings yet
- Crisis MiastenicaDocument12 pagesCrisis MiastenicaOsvaldo CortésNo ratings yet
- Update On Ocular Myasthenia GravisDocument12 pagesUpdate On Ocular Myasthenia GravisAnonymous QLadTClydkNo ratings yet
- Autoimmune Myasthenia Gravis: Emerging Clinical and Biological HeterogeneityDocument16 pagesAutoimmune Myasthenia Gravis: Emerging Clinical and Biological HeterogeneityGiuseppeNo ratings yet
- Search Criteria: Table 1Document16 pagesSearch Criteria: Table 1Armansyah Nur DewantaraNo ratings yet
- Myasthenia GravisDocument18 pagesMyasthenia GravisvandanaNo ratings yet
- Step 7 1. Mengapa Pada Skenario Pasien Merasakan Lemah Pada Kelopak Mata Dan Mengapa Paling Berat Dirasakan?Document11 pagesStep 7 1. Mengapa Pada Skenario Pasien Merasakan Lemah Pada Kelopak Mata Dan Mengapa Paling Berat Dirasakan?novkar9No ratings yet
- MG-New and Emerging Treatments (Bmjmed-2023)Document6 pagesMG-New and Emerging Treatments (Bmjmed-2023)Apostolos T.No ratings yet
- Presentation On Myasthenia Gravis: Presented By: Sandhya Harbola M.Sc. Nursing 1 Year PcnmsDocument32 pagesPresentation On Myasthenia Gravis: Presented By: Sandhya Harbola M.Sc. Nursing 1 Year PcnmsShubham Singh Bisht100% (3)
- 114 Clinical Evaluation and Management of Myasthenia Gravis - DONEDocument22 pages114 Clinical Evaluation and Management of Myasthenia Gravis - DONEpyshcotNo ratings yet
- Myasthenia Gravis: Submitted ToDocument6 pagesMyasthenia Gravis: Submitted ToRomans 6:23No ratings yet
- 156 FullDocument7 pages156 FullDorotea ArlovNo ratings yet
- A Case ReportDocument8 pagesA Case ReportYosephine MulianaNo ratings yet
- CME Article 2010 JulyDocument10 pagesCME Article 2010 JulyIlda EscalanteNo ratings yet
- Myasthenia Gravis: Moderator: DR Anitha PG: DR VijethaDocument45 pagesMyasthenia Gravis: Moderator: DR Anitha PG: DR VijethaJerusha VijethaNo ratings yet
- Myastenia GrvaisDocument4 pagesMyastenia GrvaisteenaNo ratings yet
- Anaesthesia and Myasthenia GravisDocument12 pagesAnaesthesia and Myasthenia Gravis37435rlcNo ratings yet
- Myasthenia GravisDocument11 pagesMyasthenia GravisSandeepSethiNo ratings yet
- Myasthenia Gravis - A Review of Current TherapeutiDocument7 pagesMyasthenia Gravis - A Review of Current TherapeutiZainal AbidinNo ratings yet
- ShwetaDocument9 pagesShwetasagar KumarNo ratings yet
- NEJMra 1602678Document12 pagesNEJMra 1602678Olga Manco GuzmánNo ratings yet
- NMJ Disorders: For Clinical I StudentsDocument49 pagesNMJ Disorders: For Clinical I StudentsdenekeNo ratings yet
- Myasthenia GravisDocument32 pagesMyasthenia GravisSandhya HarbolaNo ratings yet
- Maddison 2006Document10 pagesMaddison 2006Mayara MoraisNo ratings yet
- Myasthenia Gravis: by Neha Mhapralkar MSCBT 12015Document20 pagesMyasthenia Gravis: by Neha Mhapralkar MSCBT 12015Neha MhapralkarNo ratings yet
- Locuri A 2-A Specialitate NOIEMBRIE 2023Document2 pagesLocuri A 2-A Specialitate NOIEMBRIE 2023Mirela CiobanescuNo ratings yet
- Quinlan 2006Document5 pagesQuinlan 2006Mirela CiobanescuNo ratings yet
- Mks 054Document7 pagesMks 054Mirela CiobanescuNo ratings yet
- Guidelines ProcessDocument3 pagesGuidelines ProcessMirela CiobanescuNo ratings yet
- MKN 051Document5 pagesMKN 051Mirela CiobanescuNo ratings yet
- Diagnostics: Acute Labyrinthitis Revealing COVID-19Document3 pagesDiagnostics: Acute Labyrinthitis Revealing COVID-19Mirela CiobanescuNo ratings yet
- Enter Patient Weight in KG: Anticonvulsant and CNS DrugsDocument1 pageEnter Patient Weight in KG: Anticonvulsant and CNS DrugsMirela CiobanescuNo ratings yet
- Pre Operative Fasting in Children A Guideline.2Document22 pagesPre Operative Fasting in Children A Guideline.2Yulieth VanessaNo ratings yet
- Euroanaesthesia 2022 Full Programme - DBD May22Document53 pagesEuroanaesthesia 2022 Full Programme - DBD May22Mirela CiobanescuNo ratings yet
- SodiumChloridesharedcare Guideline14Document2 pagesSodiumChloridesharedcare Guideline14Mirela CiobanescuNo ratings yet
- Diploma Guide - English 2019 ApprovedDocument11 pagesDiploma Guide - English 2019 ApprovedMinaz PatelNo ratings yet
- Noradrenaline Infusion Rate BSUH Critical CareDocument4 pagesNoradrenaline Infusion Rate BSUH Critical CareAndreiCostei100% (1)
- 2021 ESC Guidelines On Cardiac Pacing andDocument94 pages2021 ESC Guidelines On Cardiac Pacing andLeo Purba100% (1)
- Antibiotic Guidelines (2020) - 0Document55 pagesAntibiotic Guidelines (2020) - 0yudhit bessieNo ratings yet
- ESPEN Guideline On Clinical Nutrition in The Intensive Care UnitDocument32 pagesESPEN Guideline On Clinical Nutrition in The Intensive Care UnitDiana MonroyNo ratings yet
- Dannandd PhillllDocument1 pageDannandd PhillllMirela CiobanescuNo ratings yet
- MetamizoleDocument15 pagesMetamizoleFahri AnugrahNo ratings yet
- Reasons Why Phil Lester Is Phil BesterDocument1 pageReasons Why Phil Lester Is Phil BesterMirela CiobanescuNo ratings yet
- Nume: Varsta: Conditii de Viata Si Munca: Motivele InternariiDocument7 pagesNume: Varsta: Conditii de Viata Si Munca: Motivele InternariiMirela CiobanescuNo ratings yet
- BM Notes SeniorDocument393 pagesBM Notes SeniorShreya KishorNo ratings yet
- Chapter 27 Chest Injuries Final TermDocument4 pagesChapter 27 Chest Injuries Final Termluwi vitonNo ratings yet
- Health Talk On AnemiaDocument15 pagesHealth Talk On Anemiasimonjosan89% (63)
- Endoscopy For Upper and Lower Gastrointestinal Procedures Standard Operating Procedure UHL Gastroenterology LocSSIPDocument15 pagesEndoscopy For Upper and Lower Gastrointestinal Procedures Standard Operating Procedure UHL Gastroenterology LocSSIPIlu SinghNo ratings yet
- 10 Penyakit Terbanyak Di Rawat Jalan Di Puskesmas Provinsi Dki Jakarta TW I Tahun 2019Document9 pages10 Penyakit Terbanyak Di Rawat Jalan Di Puskesmas Provinsi Dki Jakarta TW I Tahun 2019Klinik pratama Iqra' medical centreNo ratings yet
- Osmosis 4Document1 pageOsmosis 4dysa ayu shalsabilaNo ratings yet
- Allopurinol (Drug Study)Document2 pagesAllopurinol (Drug Study)Daisy PalisocNo ratings yet
- Cholecystitis: By: Myla Rojas. BalandraDocument5 pagesCholecystitis: By: Myla Rojas. BalandraMyla Rojas BalandraNo ratings yet
- Sports Taping Techniques Expected OutcomesDocument5 pagesSports Taping Techniques Expected OutcomesMarc Angelo DareNo ratings yet
- PSW1365 Care of The Client With Dementia Assignment Revsion S2023Document11 pagesPSW1365 Care of The Client With Dementia Assignment Revsion S2023Odia OaikhenaNo ratings yet
- Sars-Cov-2 (Covid 19) Detection (Qualitative) by Real Time RT PCRDocument3 pagesSars-Cov-2 (Covid 19) Detection (Qualitative) by Real Time RT PCRShivam GarodiaNo ratings yet
- Majorsol CottonDocument5 pagesMajorsol CottonAries Agro LimitedNo ratings yet
- Anatomy and Physiology of The EyeDocument22 pagesAnatomy and Physiology of The EyeBalkos 61No ratings yet
- Contact Dermatitis BADDocument13 pagesContact Dermatitis BADDurgaMadhab TripathyNo ratings yet
- Chapter I 5Document51 pagesChapter I 5RamNo ratings yet
- Mathematical Modeling of COVID-19 Spreading With Asymptomatic Infected and Interacting PeoplesDocument23 pagesMathematical Modeling of COVID-19 Spreading With Asymptomatic Infected and Interacting PeoplesYjhvhgjvNo ratings yet
- Formative Test DMS 2021-2022Document37 pagesFormative Test DMS 2021-2022Lidwina ChandraNo ratings yet
- Myofascial and Endodontics. 2022Document15 pagesMyofascial and Endodontics. 2022David MonroyNo ratings yet
- Spinal Cord Injury: Barrios, Kevin George BDocument52 pagesSpinal Cord Injury: Barrios, Kevin George B乔治凯文No ratings yet
- AARC Clinical Practice Guideline - Management of Airway EmergenciesDocument7 pagesAARC Clinical Practice Guideline - Management of Airway EmergenciesdoterofthemosthighNo ratings yet
- COVID-19 Travel Recommendations by Destination - CDCDocument5 pagesCOVID-19 Travel Recommendations by Destination - CDCAli Ben HusseinNo ratings yet
- Implementation of New Safety Protocols of Calle Arco Restaurant in Pagsanjan, Laguna During Pandemic CrisisDocument42 pagesImplementation of New Safety Protocols of Calle Arco Restaurant in Pagsanjan, Laguna During Pandemic CrisisOliveros John Brian R.No ratings yet
- Pune CME 2011 BrochureDocument4 pagesPune CME 2011 BrochuredrpajaniNo ratings yet
- Endodontics Principles and Practice (139 279)Document141 pagesEndodontics Principles and Practice (139 279)Daniel Ricardo Moreno HernandezNo ratings yet
- Effect of Social Media Health Communication On Knowledge Attitude and Intention To Adopt Health-Enhancing BehavDocument170 pagesEffect of Social Media Health Communication On Knowledge Attitude and Intention To Adopt Health-Enhancing Behavchukwu solomonNo ratings yet
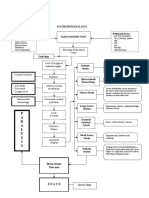
- Pathophysiology: P A R A L Y S I SDocument1 pagePathophysiology: P A R A L Y S I SJordan Garcia AguilarNo ratings yet
- Lower Limb BlocksDocument5 pagesLower Limb BlocksParvathy R NairNo ratings yet
- Bones and Joints Quiz Questions - Footprints-Science GCSE Science Animations and QuizzesDocument1 pageBones and Joints Quiz Questions - Footprints-Science GCSE Science Animations and Quizzescpcp6n7tc5No ratings yet
- Common River Medicinal Plant Handbook FINAL4Document40 pagesCommon River Medicinal Plant Handbook FINAL4Shime EthiopianNo ratings yet
- Cholinergic DrugsDocument22 pagesCholinergic Drugsmug ashNo ratings yet