You might also like
- OCULOPATHY - Disproves the orthodox and theoretical bases upon which glasses are so freely prescribed, and puts forward natural remedial methods of treatment for what are sometimes termed incurable visual defectsFrom EverandOCULOPATHY - Disproves the orthodox and theoretical bases upon which glasses are so freely prescribed, and puts forward natural remedial methods of treatment for what are sometimes termed incurable visual defectsNo ratings yet
- 009 MSK - Joint Dislocation and Fractures 2Document33 pages009 MSK - Joint Dislocation and Fractures 2نوال سائد عبداللطيف مسلماني نوال سائد عبداللطيف مسلمانيNo ratings yet
- ShoulderDocument91 pagesShoulderRazan AlayedNo ratings yet
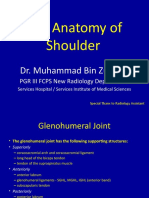
- MRI Anatomy of Shoulder: Dr. Muhammad Bin ZulfiqarDocument74 pagesMRI Anatomy of Shoulder: Dr. Muhammad Bin ZulfiqarhardboneNo ratings yet
- Disorders of The Scapula and ClavicleDocument19 pagesDisorders of The Scapula and ClavicleAbdul HadiNo ratings yet
- Miembro Superior 2Document88 pagesMiembro Superior 2DEYSI SOCUALAYA FERNANDEZNo ratings yet
- Wrist WikiRadDocument34 pagesWrist WikiRadGriggrogGingerNo ratings yet
- Opa 220-230Document11 pagesOpa 220-230Hijrana PutriNo ratings yet
- Zonal CME on Superior Shoulder Suspensory Complex (SSSC) InjuriesDocument31 pagesZonal CME on Superior Shoulder Suspensory Complex (SSSC) InjuriesheavyjayNo ratings yet
- Scapula FR EditDocument27 pagesScapula FR EditYoga ANo ratings yet
- Presentation1 150221070554 Conversion Gate01Document75 pagesPresentation1 150221070554 Conversion Gate01yellymarlianapatuNo ratings yet
- Wrist AppliedDocument78 pagesWrist AppliedBhargavNo ratings yet
- Kamars RadiologyDocument135 pagesKamars RadiologyNayantara Nair100% (1)
- William C. Cottrell, MD AbstractDocument4 pagesWilliam C. Cottrell, MD AbstractmalaNo ratings yet
- Lumber Spine and Pelvis RadiographyDocument84 pagesLumber Spine and Pelvis RadiographyMunish DograNo ratings yet
- Upper Limb Trauma X-Ray InterpretationDocument29 pagesUpper Limb Trauma X-Ray Interpretationmeita wulandariNo ratings yet
- Shoulder Orthopedic ExaminationDocument11 pagesShoulder Orthopedic ExaminationSherief MansourNo ratings yet
- Ould R: Applied AnatomyDocument4 pagesOuld R: Applied Anatomyayu feratywiNo ratings yet
- Upload Scribd 3Document5 pagesUpload Scribd 3Yoga AninditaNo ratings yet
- Imaging of Pelvis InjuryDocument9 pagesImaging of Pelvis Injuryalimran MahmudNo ratings yet
- Distal End Humerus Fractures: BY:-Dr. Anshu Sharma Guide:-Dr.A.K. MathurDocument76 pagesDistal End Humerus Fractures: BY:-Dr. Anshu Sharma Guide:-Dr.A.K. MathurToàn Đặng Phan VĩnhNo ratings yet
- Radiograph Interpretation of The Peripheral Skeleton: Author: Adam de Gruchy Last Review March 2013Document117 pagesRadiograph Interpretation of The Peripheral Skeleton: Author: Adam de Gruchy Last Review March 2013ChelseaNo ratings yet
- Anatomy and Sonoanatomy of The Shoulder: (See Fig. 4-1A and B)Document12 pagesAnatomy and Sonoanatomy of The Shoulder: (See Fig. 4-1A and B)Apollo MailNo ratings yet
- What Process Is Best Seen Using A Perpendicular CR With The Elbow in Acute Flexion and With The Posterior Aspect of The Humerus Adjacent To The Image ReceptorDocument22 pagesWhat Process Is Best Seen Using A Perpendicular CR With The Elbow in Acute Flexion and With The Posterior Aspect of The Humerus Adjacent To The Image ReceptorKalpana ParajuliNo ratings yet
- Shoulder 6 ExaminationDocument21 pagesShoulder 6 ExaminationAnil SoodNo ratings yet
- Draft 1Document33 pagesDraft 1RasYa DINo ratings yet
- Scaphoid Fracture, Bennett'S Fracture, Metacarpels, Phalanges FractureDocument61 pagesScaphoid Fracture, Bennett'S Fracture, Metacarpels, Phalanges FracturesenthilNo ratings yet
- 2.8 Additional Radio Graphic Views of The Thoracic Limb in DogsDocument8 pages2.8 Additional Radio Graphic Views of The Thoracic Limb in DogsMiri MorganNo ratings yet
- RADIOLOGY OF KNEE For StudentDocument70 pagesRADIOLOGY OF KNEE For Studentjamie mutucNo ratings yet
- radio-UL, Pelvic, LLDocument125 pagesradio-UL, Pelvic, LLsirfayNo ratings yet
- The Shoulder Anatomy & Approaches: Abdulaziz F. Ahmed, MBBS PGY-2Document61 pagesThe Shoulder Anatomy & Approaches: Abdulaziz F. Ahmed, MBBS PGY-2Abdulaziz Al-Akhras100% (1)
- Seminar on Managing Pelvic FracturesDocument89 pagesSeminar on Managing Pelvic FracturesAndreas RendraNo ratings yet
- Aco102 085dDocument2 pagesAco102 085dDonny HendrawanNo ratings yet
- Sprengel's ShoulderDocument21 pagesSprengel's ShoulderNahayo Xavier100% (1)
- Analisa X-Ray Fraktur Pada Tulang BelakangDocument77 pagesAnalisa X-Ray Fraktur Pada Tulang BelakangKurniadi BiasasajaNo ratings yet
- PELVIC INJURY CAUSES, SIGNS AND TREATMENTDocument44 pagesPELVIC INJURY CAUSES, SIGNS AND TREATMENTabhishek chaudharyNo ratings yet
- Pediatric Elbow Fractures GuideDocument97 pagesPediatric Elbow Fractures Guiderajul guptaNo ratings yet
- Primary Hip Arthroplasty Templating On Standard Radiographs A Stepwise ApproachDocument31 pagesPrimary Hip Arthroplasty Templating On Standard Radiographs A Stepwise ApproachMarius Chirila100% (1)
- Pelvic Fractures PksDocument48 pagesPelvic Fractures PksprinceveettoorNo ratings yet
- Pelvis and HipDocument90 pagesPelvis and Hipalsead798No ratings yet
- Pelvic Fracture and Hip DislocationDocument62 pagesPelvic Fracture and Hip DislocationAbdulsalam DostNo ratings yet
- CVJ Anomalies Diagnosis and Management 2011Document63 pagesCVJ Anomalies Diagnosis and Management 2011munoliNo ratings yet
- Bankurt RadiologyDocument22 pagesBankurt RadiologyVajja SwatiNo ratings yet
- Applied Radiology Featured Article (Via Radrounds)Document7 pagesApplied Radiology Featured Article (Via Radrounds)radRounds Radiology Network100% (1)
- Shoulder DislocationDocument58 pagesShoulder DislocationSri MahadhanaNo ratings yet
- The Vertebral Column Anatomy and PositioningDocument93 pagesThe Vertebral Column Anatomy and Positioningwintleah4No ratings yet
- Surgical Techniques for Repairing Canine Scapula FracturesDocument12 pagesSurgical Techniques for Repairing Canine Scapula FracturesasheneyNo ratings yet
- (Radio A) 2.1 Imaging of The ThoraxDocument69 pages(Radio A) 2.1 Imaging of The ThoraxJoshua AgawinNo ratings yet
- Radiographic EvaluationDocument12 pagesRadiographic EvaluationLuis Gerardo Castillo MendozaNo ratings yet
- Spine x ray final May 2023Document64 pagesSpine x ray final May 2023sayedoooovNo ratings yet
- Fractures and Dislocations About The Elbow in The Pediatric PatientDocument65 pagesFractures and Dislocations About The Elbow in The Pediatric PatientPeter HubkaNo ratings yet
- Chest RadiographyDocument19 pagesChest RadiographyClaraMonet PalomoNo ratings yet
- Elbow - Fractures in Children: Fracture MechanismDocument31 pagesElbow - Fractures in Children: Fracture MechanismhendoramuNo ratings yet
- Humerus and Elbow: Episode OverviewDocument16 pagesHumerus and Elbow: Episode OverviewHoward ChangNo ratings yet
- Lateral Condylar Fracture in ChildrenDocument19 pagesLateral Condylar Fracture in ChildrenMuhammed Muzzammil SanganiNo ratings yet
- Kinesiology Chap 6 TransesDocument4 pagesKinesiology Chap 6 TranseschloegmndzNo ratings yet
- Radio-Ulnar SynostosisDocument16 pagesRadio-Ulnar SynostosisVenkatanarasimhan BNo ratings yet
- Upper Limb Dislocation: Presented by Elias Godfrey Supervisor DR Swai 20 November 2017Document67 pagesUpper Limb Dislocation: Presented by Elias Godfrey Supervisor DR Swai 20 November 2017albertjosephNo ratings yet
- Cervical X-RayDocument8 pagesCervical X-RayRio Yus RamadhaniNo ratings yet
- Vi. Ûrxm: ®vôtôw ® Øû/LsDocument4 pagesVi. Ûrxm: ®vôtôw ® Øû/Lsbgk_usNo ratings yet
- Ethical Issues of Unrelated Hematopoietic Stem Cell Transplantation in Adult Thalassemia PatientsDocument7 pagesEthical Issues of Unrelated Hematopoietic Stem Cell Transplantation in Adult Thalassemia PatientsMcullfy JohnNo ratings yet
- Shigella SPP, Vibrio SPPDocument6 pagesShigella SPP, Vibrio SPPtomal7811islamNo ratings yet
- American Journal of Emergency MedicineDocument7 pagesAmerican Journal of Emergency MedicineVirgi AgustiaNo ratings yet
- PharmNotesDocument210 pagesPharmNoteschiragvetsNo ratings yet
- Care of The Acutely Unwell FinalDocument100 pagesCare of The Acutely Unwell Finalgireeshsachin100% (1)
- IDAO - TYPOLOGY 1st & 2nd ASSESSMENTDocument2 pagesIDAO - TYPOLOGY 1st & 2nd ASSESSMENTJingjing BelanoNo ratings yet
- NCM 106 - Pharmacology Principles of Medication AdministrationDocument10 pagesNCM 106 - Pharmacology Principles of Medication AdministrationEarl BenedictNo ratings yet
- Uterine Rupture and Cervical TearDocument16 pagesUterine Rupture and Cervical Tearsangita patil0% (1)
- PDFDocument298 pagesPDFaliakbar178No ratings yet
- Acute CholangitisDocument12 pagesAcute CholangitisWira LinNo ratings yet
- N220 W9 Nursing Care PlanDocument3 pagesN220 W9 Nursing Care PlanVivian PhamNo ratings yet
- Dengue Shock SyndromeDocument17 pagesDengue Shock SyndromehwelpNo ratings yet
- Effect of Intraoperative Dexmedetomidine On Post-Craniotomy PainDocument9 pagesEffect of Intraoperative Dexmedetomidine On Post-Craniotomy PainIva SantikaNo ratings yet
- AscariasisDocument7 pagesAscariasisMia Angela Del MundoNo ratings yet
- Cad NCPDocument1 pageCad NCPKrizzia Mae F. MayoresNo ratings yet
- Escherichia ColiDocument31 pagesEscherichia ColiLizzie Fizzie100% (1)
- Faktor Risiko, Diagnosis, Dan Tatalaksana Dermatitis Atopik Pada Bayi Dan AnakDocument11 pagesFaktor Risiko, Diagnosis, Dan Tatalaksana Dermatitis Atopik Pada Bayi Dan AnakPutry MelindaNo ratings yet
- Achilles Tendinopathy What Runners Should Know FinitoDocument4 pagesAchilles Tendinopathy What Runners Should Know FinitoAdmirNo ratings yet
- Complex Regional Pain Syndrome (CRPS) Type I: Historical Perspective and Critical IssuesDocument7 pagesComplex Regional Pain Syndrome (CRPS) Type I: Historical Perspective and Critical IssuesSheilaNo ratings yet
- Case Study On Prostate CancerDocument16 pagesCase Study On Prostate Cancerferdz02100% (5)
- Complications Bariatric SurgeryDocument8 pagesComplications Bariatric SurgeryThita Orrego100% (1)
- The Montgomery Borgatta Caregiver Burden ScaleDocument22 pagesThe Montgomery Borgatta Caregiver Burden ScalehjhjkNo ratings yet
- Angiogenesis in CancerDocument4 pagesAngiogenesis in CanceranonymousNo ratings yet
- Definisi & PICO 3, 4Document5 pagesDefinisi & PICO 3, 4Dionisius KevinNo ratings yet
- Hemorrhoidectomy: Prepared By: Kristine Anne M. Lacorte BSN Iii-CDocument13 pagesHemorrhoidectomy: Prepared By: Kristine Anne M. Lacorte BSN Iii-CRita Honrade HernandezNo ratings yet
- Biliary Tree LectureDocument58 pagesBiliary Tree Lecturesgod34No ratings yet
- Helicobacter Pylori Infection: Ivth Brazilian Consensus Conference OnDocument25 pagesHelicobacter Pylori Infection: Ivth Brazilian Consensus Conference OnhugotavioNo ratings yet
- Medical AbbreviationsDocument6 pagesMedical AbbreviationsEina CarmonaNo ratings yet
- Daftar PustakaDocument4 pagesDaftar PustakaDeasy Arindi PutriNo ratings yet