You might also like
- A Sea of Broken Hearts: Patient Rights in a Dangerous, Profit-Driven Health Care SystemFrom EverandA Sea of Broken Hearts: Patient Rights in a Dangerous, Profit-Driven Health Care SystemNo ratings yet
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- STROKE: Handbook with activities, exercises and mental challengesFrom EverandSTROKE: Handbook with activities, exercises and mental challengesNo ratings yet
- High Blood Pressure: Safe alternatives without drugsFrom EverandHigh Blood Pressure: Safe alternatives without drugsRating: 5 out of 5 stars5/5 (2)
- Arretez de Vous Saboter Vous Etes Exceptionnel - BookysDocument164 pagesArretez de Vous Saboter Vous Etes Exceptionnel - BookysAbdelaziz Benbirouk100% (5)
- Torsade De Pointes, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandTorsade De Pointes, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsFrom EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsNo ratings yet
- Questions and Answers in Small Animal AnesthesiaFrom EverandQuestions and Answers in Small Animal AnesthesiaLesley J. SmithNo ratings yet
- EKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookFrom EverandEKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookNo ratings yet
- Oropharyngeal Nasopharyngeal SuctioningDocument3 pagesOropharyngeal Nasopharyngeal SuctioningMarie Kelsey Acena Macaraig100% (2)
- Pacemaker Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandPacemaker Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Clase 6 - IcdasDocument27 pagesClase 6 - IcdasdavidNo ratings yet
- Assessment of bleeding Shock in a Politraumatized PatientFrom EverandAssessment of bleeding Shock in a Politraumatized PatientNo ratings yet
- Central Venous Pressure: Its Clinical Use and Role in Cardiovascular DynamicsFrom EverandCentral Venous Pressure: Its Clinical Use and Role in Cardiovascular DynamicsNo ratings yet
- A Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisFrom EverandA Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisRating: 5 out of 5 stars5/5 (1)
- La Guía de La Startup A La Puntuación Neta de Promotores (NPS)Document7 pagesLa Guía de La Startup A La Puntuación Neta de Promotores (NPS)CARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Perfusion for Congenital Heart Surgery: Notes on Cardiopulmonary Bypass for a Complex Patient PopulationFrom EverandPerfusion for Congenital Heart Surgery: Notes on Cardiopulmonary Bypass for a Complex Patient PopulationRating: 5 out of 5 stars5/5 (2)
- Situación de La Salud en El PerúDocument3 pagesSituación de La Salud en El PerúNark RengifoNo ratings yet
- Orthostatic Hypotension in Older AdultsFrom EverandOrthostatic Hypotension in Older AdultsAhmet Turan IsikNo ratings yet
- Microcirculation: From Bench to BedsideFrom EverandMicrocirculation: From Bench to BedsideMaria DorobantuNo ratings yet
- Cardiorenal Syndrome in Heart FailureFrom EverandCardiorenal Syndrome in Heart FailureW. H. Wilson TangNo ratings yet
- Adult Congenital Heart Disease in Clinical PracticeFrom EverandAdult Congenital Heart Disease in Clinical PracticeDoreen DeFaria YehNo ratings yet
- Complications of Percutaneous Coronary Intervention: The Survival HandbookFrom EverandComplications of Percutaneous Coronary Intervention: The Survival HandbookAlistair LindsayNo ratings yet
- Practical Management of Systemic Sclerosis in Clinical PracticeFrom EverandPractical Management of Systemic Sclerosis in Clinical PracticeNo ratings yet
- Prostaglandins, Platelets, Lipids: New Developments in AtherosclerosisFrom EverandProstaglandins, Platelets, Lipids: New Developments in AtherosclerosisNo ratings yet
- Clinical Handbook of Cardiac ElectrophysiologyFrom EverandClinical Handbook of Cardiac ElectrophysiologyBenedict M. GloverNo ratings yet
- Median Arcuate Ligament Syndrome: Pathophysiology, Symptoms, Signs, and ManagementFrom EverandMedian Arcuate Ligament Syndrome: Pathophysiology, Symptoms, Signs, and ManagementNo ratings yet
- Posterior Circulation Stroke: Advances in Understanding and ManagementFrom EverandPosterior Circulation Stroke: Advances in Understanding and ManagementJong S. KimNo ratings yet
- Coronary Vasomotion AbnormalitiesFrom EverandCoronary Vasomotion AbnormalitiesHiroaki ShimokawaNo ratings yet
- Difficult Acute Cholecystitis: Treatment and Technical IssuesFrom EverandDifficult Acute Cholecystitis: Treatment and Technical IssuesNo ratings yet
- Postural Tachycardia Syndrome: A Concise and Practical Guide to Management and Associated ConditionsFrom EverandPostural Tachycardia Syndrome: A Concise and Practical Guide to Management and Associated ConditionsNicholas GallNo ratings yet
- Proteasomal AAA ATPases Struct - 2012 - Biochimica Et Biophysica Acta BBA - MDocument16 pagesProteasomal AAA ATPases Struct - 2012 - Biochimica Et Biophysica Acta BBA - MCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Science 1202393Document8 pagesScience 1202393CARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Sala Situacional de Dengue Sub Region de Salud Morropon Huancabamba SE: 15, AÑO 2022Document48 pagesSala Situacional de Dengue Sub Region de Salud Morropon Huancabamba SE: 15, AÑO 2022CARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Ijo 11 05 858Document16 pagesIjo 11 05 858CARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Posición en RampaDocument3 pagesPosición en RampaCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Douetal 2014 SpringerDocument19 pagesDouetal 2014 SpringerCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- ISNO Consensus Guidelines For Practical Adaptation of The WHO 2016 Classification of Adult Diffuse GliomasDocument11 pagesISNO Consensus Guidelines For Practical Adaptation of The WHO 2016 Classification of Adult Diffuse GliomasCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Chloride and Hydrogen Ion Distribution Between Human Red Cells and PlasmaDocument12 pagesChloride and Hydrogen Ion Distribution Between Human Red Cells and PlasmaCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Triple Control Implications Cardiac Disease: of RelaxationDocument7 pagesTriple Control Implications Cardiac Disease: of RelaxationCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Dirk L. Brutsaert 1980Document16 pagesDirk L. Brutsaert 1980CARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Structure and Function of The AAA - 2012 - Biochimica Et Biophysica Acta BBADocument13 pagesStructure and Function of The AAA - 2012 - Biochimica Et Biophysica Acta BBACARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Dirk L. Brutsaert 2007-1Document9 pagesDirk L. Brutsaert 2007-1CARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Dirk L. Brutsaert 2007Document9 pagesDirk L. Brutsaert 2007CARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Valoración Preoperatoria de La Ví - A Aérea Difí - Cil ¿Hay Algo NuevoDocument23 pagesValoración Preoperatoria de La Ví - A Aérea Difí - Cil ¿Hay Algo NuevoCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- 111742Document6 pages111742CARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Ventilación DifícilDocument8 pagesVentilación DifícilCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Apendicitis Aguda - Guías de Práctica ClínicaDocument9 pagesApendicitis Aguda - Guías de Práctica ClínicaCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Aguilera p144 v46n3 2020Document9 pagesAguilera p144 v46n3 2020CARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Acid-Base And: Respiratory Properties of A Butrered Bovine Erythrocyte Perfusion MediumDocument6 pagesAcid-Base And: Respiratory Properties of A Butrered Bovine Erythrocyte Perfusion MediumCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Ponce Santiago Adriana EvelynDocument72 pagesPonce Santiago Adriana EvelynCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Multidimensional Scaling of Diffuse Gliomas ApplicDocument15 pagesMultidimensional Scaling of Diffuse Gliomas ApplicCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Net Promoter Score o NPS, Qué Es y para Qué SirveDocument4 pagesNet Promoter Score o NPS, Qué Es y para Qué SirveCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Caso CADDocument4 pagesCaso CADCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Adenomas HipofisiariosDocument13 pagesAdenomas HipofisiariosCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- A Nomogram For The Interpretation of Acid-Base Data: Summary: A Diagnostic Nomogram Based On Log pCODocument4 pagesA Nomogram For The Interpretation of Acid-Base Data: Summary: A Diagnostic Nomogram Based On Log pCOCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
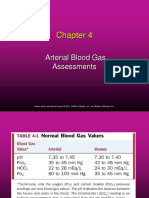
- Arterial Blood Gas AssessmentsDocument55 pagesArterial Blood Gas AssessmentsCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Resonancia Magnética en Adenomas de HipófisisDocument9 pagesResonancia Magnética en Adenomas de HipófisisCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Restauración Nacional Comas: Plan de GobiernoDocument49 pagesRestauración Nacional Comas: Plan de GobiernoCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- RM e HipófisisDocument15 pagesRM e HipófisisCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Acta de Conformidad 2022Document2 pagesActa de Conformidad 2022elena alfaroNo ratings yet
- Bilirubin Induced Neurologic DamageDocument10 pagesBilirubin Induced Neurologic DamageAbd. Rahim MubarakNo ratings yet
- Insuficiencia RespiratoriaDocument12 pagesInsuficiencia Respiratoriaapi-326940690No ratings yet
- Cómo Realizar RCPDocument4 pagesCómo Realizar RCPAguita De horchataNo ratings yet
- CONVIDADocument1 pageCONVIDACarlos ExcusasNo ratings yet
- Pengenalan DiabetesDocument57 pagesPengenalan DiabetesAsma MandaNo ratings yet
- Trastornos en La InfanciaDocument25 pagesTrastornos en La Infanciaandy laihoNo ratings yet
- El Peligro Del Uso Interno de Los Aceites EsencialesDocument2 pagesEl Peligro Del Uso Interno de Los Aceites EsencialesKetty UesuNo ratings yet
- Adultez MediaDocument44 pagesAdultez MediaMaria José MolinaNo ratings yet
- Abscesos y Fístulas AnorrectalesDocument2 pagesAbscesos y Fístulas AnorrectalesDavid Lepín MelillánNo ratings yet
- Max Life Insurance Company Limited: Proposal NumberDocument9 pagesMax Life Insurance Company Limited: Proposal NumberBhardwaj JinnyNo ratings yet
- PROYECTO Modelo IMC.Document28 pagesPROYECTO Modelo IMC.Jesús AquinoNo ratings yet
- Taller3 de La Actividad 4Document11 pagesTaller3 de La Actividad 4Marcela ErazoNo ratings yet
- InflamaciónDocument35 pagesInflamacióndiana ortegaNo ratings yet
- SIMULACIÓN CASO 2 Parte 2Document4 pagesSIMULACIÓN CASO 2 Parte 2Valeria Grande100% (1)
- Cuestionario Sanitaria 1 AirmDocument10 pagesCuestionario Sanitaria 1 AirmDanielNo ratings yet
- TUSIDocument18 pagesTUSINidia CárcamoNo ratings yet
- AmbulationDocument48 pagesAmbulationShristi RanaNo ratings yet
- Evaluacion Biologia Segundo Periodo Ciclo IvDocument3 pagesEvaluacion Biologia Segundo Periodo Ciclo Ivjohana carrilloiNo ratings yet
- Protocolo Atencion Al LesionadoDocument30 pagesProtocolo Atencion Al LesionadoJennifer AfricanoNo ratings yet
- 276-Texto Del Artículo-1866-3-10-20200903Document16 pages276-Texto Del Artículo-1866-3-10-20200903Luis678No ratings yet
- formato-de-solicitud-de-expediente-clinico-imss (3)Document2 pagesformato-de-solicitud-de-expediente-clinico-imss (3)Odeth MontsNo ratings yet
- Dysgraphia Hand OutsDocument14 pagesDysgraphia Hand OutsRachelle Garobo BisaNo ratings yet
- Aspectos Farmacologicos de KetaminaDocument32 pagesAspectos Farmacologicos de KetaminaRaulDagaNo ratings yet
- Indice Onomastico Del Volumen 28 2012Document123 pagesIndice Onomastico Del Volumen 28 2012Jessie Romero ChauxNo ratings yet
- GUIA DE APRENDIZAJE GUILLAIN BARRET - Cuidado Del Niño y Adulto I.Document2 pagesGUIA DE APRENDIZAJE GUILLAIN BARRET - Cuidado Del Niño y Adulto I.Maria Fernanda Zuluaga MuñozNo ratings yet