You might also like
- Master Patient Index FormDocument2 pagesMaster Patient Index Formapi-355199088No ratings yet
- Complaint to DOHDocument4 pagesComplaint to DOHNewsday EditorNo ratings yet
- Attending Physician's Statement for Death ClaimDocument2 pagesAttending Physician's Statement for Death ClaimLhen TrinidadNo ratings yet
- IPRFormDocument2 pagesIPRFormSuvendu SahaNo ratings yet
- D StatmentDocument8 pagesD StatmentHihiNo ratings yet
- Registration FormDocument1 pageRegistration Formkatie_luvstamiiNo ratings yet
- Checklist For New Patients or Prior Patients Not Seen Within 3 YearsDocument20 pagesChecklist For New Patients or Prior Patients Not Seen Within 3 YearsRebecca KnightNo ratings yet
- New-Medical History Form - Clearly Orthodontics With Social MediaDocument2 pagesNew-Medical History Form - Clearly Orthodontics With Social MediaAatekaNo ratings yet
- Registration Form: St. Jude General Hospital and Medical CenterDocument1 pageRegistration Form: St. Jude General Hospital and Medical CenterTon RiveraNo ratings yet
- 0960-0555 Sample MER Forms PDFDocument9 pages0960-0555 Sample MER Forms PDFAbhay SingaviNo ratings yet
- Registration Form Laboratorium Ilmu FaalDocument2 pagesRegistration Form Laboratorium Ilmu FaalYhusi KarinaNo ratings yet
- PT RegistrationDocument2 pagesPT Registrationparisa1No ratings yet
- Patient Medical Records RequestDocument2 pagesPatient Medical Records RequestTanessa WilliamsNo ratings yet
- Patient Registration FormDocument1 pagePatient Registration FormCosmin DanNo ratings yet
- Pranic Healing Patient Record FormDocument6 pagesPranic Healing Patient Record FormGuida Lourenco100% (2)
- RSA Death Claim FormDocument4 pagesRSA Death Claim FormMartha MtikaNo ratings yet
- Winter Retreat Health & Consent 2009Document2 pagesWinter Retreat Health & Consent 2009Andrew NelsonNo ratings yet
- Patient Admission Form: For Office Use OnlyDocument2 pagesPatient Admission Form: For Office Use OnlyCaca KhairunissaNo ratings yet
- Health Declaration FormDocument3 pagesHealth Declaration FormMaja Aira BumatayNo ratings yet
- Benjs Medicenter Patient InformationDocument1 pageBenjs Medicenter Patient InformationcharNo ratings yet
- Mississippi State Board of Medical Licensure: Complaint FormDocument5 pagesMississippi State Board of Medical Licensure: Complaint FormScott SistersNo ratings yet
- AcupunctureDocument8 pagesAcupunctureNabendu SahaNo ratings yet
- Youth Club App PhillyDocument3 pagesYouth Club App Phillyapi-357278378No ratings yet
- Med.014 - Penolakan Tindakan Kedokteran (English)Document3 pagesMed.014 - Penolakan Tindakan Kedokteran (English)Laila FerdiniNo ratings yet
- Pediatric Patient Registration Form TemplateDocument5 pagesPediatric Patient Registration Form TemplateHasfi YakobNo ratings yet
- Individual Death Claim Form Proposed Standard 2022Document3 pagesIndividual Death Claim Form Proposed Standard 2022Anirudh SagaNo ratings yet
- Merged Forms File For Website 5Document5 pagesMerged Forms File For Website 5ann hillNo ratings yet
- CSN Income Protection Claim Form AssistanceDocument9 pagesCSN Income Protection Claim Form AssistanceRahmaNo ratings yet
- Incident - Accident Report FormDocument1 pageIncident - Accident Report FormZai SenNo ratings yet
- Colorado Medical Marijuana Support Employee FormDocument12 pagesColorado Medical Marijuana Support Employee FormNickNo ratings yet
- Soccer Registration FormDocument2 pagesSoccer Registration FormmikevalhallNo ratings yet
- THAS - Referral Form 2022Document2 pagesTHAS - Referral Form 2022NemesisNo ratings yet
- Case HX SLP AdultDocument2 pagesCase HX SLP AdultHarshit AmbeshNo ratings yet
- One Step Med: General Medical Information Record Keeping ManualFrom EverandOne Step Med: General Medical Information Record Keeping ManualNo ratings yet
- Client Intake Form: Date Patient Last: First Initial Address City Zip Date of Birth Phone CellDocument6 pagesClient Intake Form: Date Patient Last: First Initial Address City Zip Date of Birth Phone Celljayson_tamayo2No ratings yet
- Cannalogue Medical DocumentDocument1 pageCannalogue Medical DocumentolgaNo ratings yet
- MIRAZUR HOSPITAL (Form)Document1 pageMIRAZUR HOSPITAL (Form)Mario GrizzlyNo ratings yet
- Adult PacketDocument5 pagesAdult PacketcentraltexasentNo ratings yet
- Patient admission formDocument1 pagePatient admission formTika Yulasni100% (5)
- Youth Club App11Document3 pagesYouth Club App11api-357278378No ratings yet
- Personal Information Form 08Document4 pagesPersonal Information Form 08Rizki AgustiantoNo ratings yet
- Health Statement FormDocument2 pagesHealth Statement FormRose Ann DuqueNo ratings yet
- Health Pre-Authorization Claim FormDocument2 pagesHealth Pre-Authorization Claim Formsachin vermaNo ratings yet
- Statement Regarding Marriage: SSA-753 (07-2015) Uf (07-2015)Document3 pagesStatement Regarding Marriage: SSA-753 (07-2015) Uf (07-2015)raex_innoNo ratings yet
- 1.formal ApplicationDocument8 pages1.formal ApplicationNaturalBite ChefNo ratings yet
- MSH Claim Form Dubai - GCCDocument1 pageMSH Claim Form Dubai - GCCWilliam IsaacNo ratings yet
- Practice Fusion - PrintChartDocument10 pagesPractice Fusion - PrintChartGet Well SoonNo ratings yet
- Patient Face Sheet TemplateDocument5 pagesPatient Face Sheet TemplateAdrienn Krisztina VargaNo ratings yet
- KS - RegisterDocument2 pagesKS - RegisterhcbbNo ratings yet
- IKATAN DOKTER INDONESIA FORMULIR ADocument2 pagesIKATAN DOKTER INDONESIA FORMULIR ARhadian Wira FebiantoNo ratings yet
- Claimant Statement Form (Death Claims) : Customer Helpline No: 1860 266 7766Document3 pagesClaimant Statement Form (Death Claims) : Customer Helpline No: 1860 266 7766Tarun RustagiNo ratings yet
- Opening FormDocument40 pagesOpening FormNetra VasoyaNo ratings yet
- Authorization For Release of Medical InformationDocument1 pageAuthorization For Release of Medical Informationcig3fNo ratings yet
- File accident claim forms and submit required documentationDocument9 pagesFile accident claim forms and submit required documentationDan McGeeNo ratings yet
- New Employee Details Form - October 2019Document3 pagesNew Employee Details Form - October 2019LEahNo ratings yet
- DMC Patient FormsDocument6 pagesDMC Patient FormsScott cosentinoNo ratings yet
- Victorian AOD Intake ToolDocument5 pagesVictorian AOD Intake ToolHarjotBrarNo ratings yet
- Protect your health by completing this contact tracing formDocument2 pagesProtect your health by completing this contact tracing formIrfan MustafaiNo ratings yet
- Veterans Administration Claims: What You Need to Know to Be SuccessfulFrom EverandVeterans Administration Claims: What You Need to Know to Be SuccessfulNo ratings yet
- David Jennings: Debit Account Transactions Date Description Type Amount Available Matthew SteversonDocument4 pagesDavid Jennings: Debit Account Transactions Date Description Type Amount Available Matthew Steversondolapo BalogunNo ratings yet
- Screenshot 2022-10-03 at 6.15.00 PMDocument2 pagesScreenshot 2022-10-03 at 6.15.00 PMdolapo BalogunNo ratings yet
- Scott Luman 5929 FM 711 CENTER, TX 75935-000Document6 pagesScott Luman 5929 FM 711 CENTER, TX 75935-000dolapo BalogunNo ratings yet
- Form 1099 MISC David Kovach-1Document1 pageForm 1099 MISC David Kovach-1dolapo BalogunNo ratings yet
- File your 1040 tax return onlineDocument2 pagesFile your 1040 tax return onlineSammi Bowe100% (1)
- Wells Fargo Combined Statement of AccountsDocument6 pagesWells Fargo Combined Statement of Accountsdolapo Balogun100% (1)
- 8448 20 002 1010441 0282 Auto Pay NoticeDocument4 pages8448 20 002 1010441 0282 Auto Pay Noticedolapo BalogunNo ratings yet
- Profit or Loss From Business: I I I I I I I IDocument1 pageProfit or Loss From Business: I I I I I I I Idolapo BalogunNo ratings yet
- Wells Fargo Combined Statement of AccountsDocument6 pagesWells Fargo Combined Statement of Accountsdolapo Balogun100% (1)
- Raymond William Enyeart PO Box 1527 Calipatria CA 92233-1527Document1 pageRaymond William Enyeart PO Box 1527 Calipatria CA 92233-1527dolapo BalogunNo ratings yet
- f1040 Schedule C Expenses PDFDocument2 pagesf1040 Schedule C Expenses PDFVallery FisherNo ratings yet
- Raymond William Enyeart PO Box 1527 Calipatria CA 92233-1527Document1 pageRaymond William Enyeart PO Box 1527 Calipatria CA 92233-1527dolapo BalogunNo ratings yet
- f1040 Schedule C Expenses PDFDocument2 pagesf1040 Schedule C Expenses PDFVallery FisherNo ratings yet
- Wells Fargo Combined Statement of AccountsDocument6 pagesWells Fargo Combined Statement of Accountsdolapo Balogun100% (1)
- f1040 Schedule C Expenses PDFDocument2 pagesf1040 Schedule C Expenses PDFVallery FisherNo ratings yet
- Raymond William Enyeart PO Box 1527 Calipatria CA 92233-1527Document1 pageRaymond William Enyeart PO Box 1527 Calipatria CA 92233-1527dolapo BalogunNo ratings yet
- Mary White: Simonette GeraldDocument2 pagesMary White: Simonette Geralddolapo BalogunNo ratings yet
- Account Summary: 1-800-427-2200 EnglishDocument2 pagesAccount Summary: 1-800-427-2200 Englishdolapo Balogun100% (1)
- Passionate love letter longing for commitmentDocument2 pagesPassionate love letter longing for commitmentFaboyede Temmy86% (7)
- Notes 200607 155224 565Document3 pagesNotes 200607 155224 565dolapo BalogunNo ratings yet
- Check Messages & Responses ReceivedDocument1 pageCheck Messages & Responses Receiveddolapo BalogunNo ratings yet
- Test Bank For Goulds Pathophysiology For The Health Professions 6th Edition by HubertDocument6 pagesTest Bank For Goulds Pathophysiology For The Health Professions 6th Edition by HubertFranklin Roberts100% (37)
- The Acute Hemoabdomen: Topic OverviewDocument23 pagesThe Acute Hemoabdomen: Topic OverviewWeiwei CierraNo ratings yet
- (Equine Veterinary Journal 2010-Jan 05 Vol. 37 Iss. 2) W. W. MUIR - Pain Therapy in Horses (2010) (10.2746 - 0425164054223831) - Libgen - LiDocument3 pages(Equine Veterinary Journal 2010-Jan 05 Vol. 37 Iss. 2) W. W. MUIR - Pain Therapy in Horses (2010) (10.2746 - 0425164054223831) - Libgen - LiAcupuntura de EquinosNo ratings yet
- Common Signs and Symptoms of Drug Dependence and AddictionDocument4 pagesCommon Signs and Symptoms of Drug Dependence and AddictionAbbygail WasilNo ratings yet
- Course Exercise - PALS Precourse Self-Assessment and Precourse WorkDocument3 pagesCourse Exercise - PALS Precourse Self-Assessment and Precourse WorkPRICINo ratings yet
- ATI RN Mental Health Online Practice BDocument38 pagesATI RN Mental Health Online Practice Bseansdrew2No ratings yet
- Urology1 UPDATEDDocument44 pagesUrology1 UPDATEDmarwanNo ratings yet
- Social Studies SbaDocument26 pagesSocial Studies SbaKeasha Jones100% (1)
- Dosimetric comparison of Cyberknife vs. Linac for lung cancer SBRTDocument26 pagesDosimetric comparison of Cyberknife vs. Linac for lung cancer SBRTraheel252No ratings yet
- Immune System Drugs - FinalDocument56 pagesImmune System Drugs - FinalSarte Rachelle AnneNo ratings yet
- Primary Hyperaldosteronism - StatPearls - NCBI BookshelfDocument7 pagesPrimary Hyperaldosteronism - StatPearls - NCBI BookshelfCecil-An DalanonNo ratings yet
- Marcil 2001Document4 pagesMarcil 2001Mariana JuravleNo ratings yet
- Monica Shukla CV 01-16-2023Document13 pagesMonica Shukla CV 01-16-2023medical HunterNo ratings yet
- Dyspepsia in Children IFFGDDocument2 pagesDyspepsia in Children IFFGDNorman Alexander TampubolonNo ratings yet
- Pancreatic CancerDocument2 pagesPancreatic CancerSwag MasterNo ratings yet
- MDCG 2020-10-2 - Saf Rep Clin Inv MDDocument715 pagesMDCG 2020-10-2 - Saf Rep Clin Inv MDLorenaNo ratings yet
- 8 Surgical InfectionDocument34 pages8 Surgical InfectionAhed ShaerNo ratings yet
- Gradenigos Syndrome A ReviewDocument5 pagesGradenigos Syndrome A ReviewPaola SanchezNo ratings yet
- Medical Treatment Recuperation Convalescence With HomoeopathyDocument4 pagesMedical Treatment Recuperation Convalescence With HomoeopathyEditor IJTSRDNo ratings yet
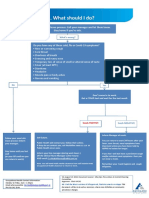
- What To Do If Youre Sick FlowchartDocument1 pageWhat To Do If Youre Sick FlowchartfuckyouNo ratings yet
- Service: Medicine Attending Physician: Dr. Santos Date/Time 06/10/21 1400Document4 pagesService: Medicine Attending Physician: Dr. Santos Date/Time 06/10/21 1400Andrea Kyla Dela PazNo ratings yet
- NCM 118 - CCN - THEORY - MidtermsDocument19 pagesNCM 118 - CCN - THEORY - MidtermsSTEFFANIE VALE BORJANo ratings yet
- A Comprehensive Guide For COVID-19 Longhaulers and Physicians - The PASC Master DocumentDocument24 pagesA Comprehensive Guide For COVID-19 Longhaulers and Physicians - The PASC Master DocumentVirginia Ferrer UrbanoNo ratings yet
- Advances in Cancer Immunotherapy 2019 - Latest TrendsDocument21 pagesAdvances in Cancer Immunotherapy 2019 - Latest TrendsSWAGATIKA CHANDANo ratings yet
- First Aid & Bandaging Techniques GuideDocument35 pagesFirst Aid & Bandaging Techniques GuideJoel VelasquezNo ratings yet
- Novolin and HumulinDocument3 pagesNovolin and HumulinChynnaNo ratings yet
- Medicine GBS: Guillain Barre SyndromeDocument4 pagesMedicine GBS: Guillain Barre SyndromedinakarNo ratings yet
- The Different Perspectives of DisasterDocument27 pagesThe Different Perspectives of DisasterWincer CaballesNo ratings yet
- Kode ICdDocument5 pagesKode ICdAudiah F HadinataNo ratings yet
- Argumentitive Essay About Bariatric SurgeryDocument2 pagesArgumentitive Essay About Bariatric SurgeryNourNo ratings yet